
Remember me




Endotracheal tube cuffs create a seal between the endotracheal tube and the trachea, preventing aspiration of fluids and pathogens from the pharynx to the lungs and ventilation leaks. Consensus suggests that the cuff pressure of endotracheal tubes should range from 20 to 30 cmH2O.1 In clinical practice, however, cuff pressures of >30 cmH2O may be required to create a seal in the trachea.2 One possible reason for this is that the cuff size may be unsuitable.
Global guidelines currently lack clear guidance or consensus on selection of the most appropriate oral endotracheal tube model.3 Studies outside China suggest that an endotracheal tube with an inner diameter (ID) of 7.0–8.0 mm is usually chosen for women and that a tube with an ID of 8.0–8.5 mm is usually chosen for men. A formula based on age is traditionally used to predict the most appropriate size of endotracheal tube for children. For example, Cole's formula4 for an endotracheal tube without the cuff is ID in mm = (0.25 × age in years) +4.0, and Motoyama's formula5 for an endotracheal tube with the cuff is ID in mm = (0.25 × age in years) +3.5. Thus, there is no consensus on the choice of endotracheal tubes for patients, and an accurate and feasible method is urgently needed.
2 CASE PRESENTATIONA 70-year-old woman was referred to our hospital because lung cancer had been found by chest X-ray computed tomography (CT) in October 2019. Chest CT showed right lower lung cancer with mediastinal and right hilar lymph node metastasis, multiple small nodules in the right lower lung, chronic bronchitis, emphysema, and multiple bullae in both lungs. Her height was 158 cm, and her weight was 50 kg. Her blood pressure was 169/99 mmHg, and her heart rate was 65 bpm. The patient underwent lobectomy and lymph node dissection via thoracoscopy in October 2019. She received endotracheal intubation and ventilator-assisted respiration after the operation in the thoracic and cardiac surgery intensive care unit. Her cuff pressure was maintained with the minimum leak technique and measured with a cuff pressure gauge.6 Subsequent cuff manometer measurement demonstrated a pressure of 100 cmH2O.
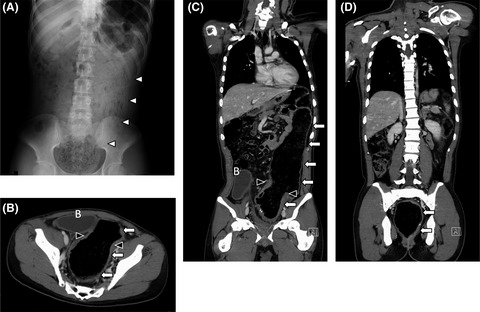
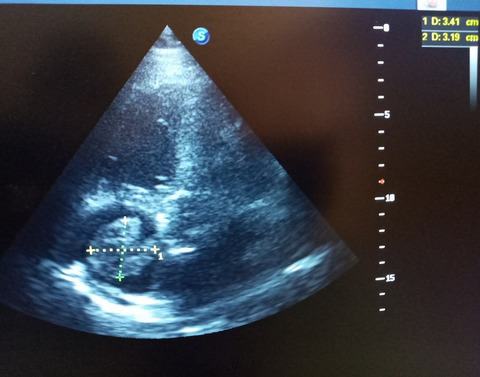
3 RADIOGRAPHIC IMAGINGUsing the patient's tracheal cross-sectional area at different vertebrae, endotracheal tube cuff undersizing was diagnosed by chest CT. The endotracheal tube was inserted through the mouth, and CT showed that the tracheal area at the T2 vertebra was 584.2 mm2 (Figure 1A), that at the T3 vertebra was 646.2 mm2 (Figure 1B), and that at the T4 vertebra was 498.8 mm2 (Figure 1C). The ID of the endotracheal tube was 7.0 mm (Guangzhou Weili Medical Equipment Co., Ltd.), the cuff diameter was 22 mm, and the cuff cross-sectional area was 380.13 mm2. The patient's tracheal cross-sectional area was greater than the cross-sectional area of the cuff (380.13 mm2) (Figure 2).

Computed tomography images used for measurement of tracheal cross-sectional area at different upper vertebral levels. (A) T2 vertebra (584.2 mm2). (B) T3 vertebra (646.2 mm2). (C) T4 vertebra (498.8 mm2)

Comparison of cross-sectional area of endotracheal tube cuff and patient's trachea at T2, T3, and T4 vertebra
4 DISCUSSIONAljatlany et al.7 introduced the following formula for measuring the cross-sectional area of the trachea: Cross-sectional area = −171.834 + (0.5850 × age in years) + (86.8685 × sex) + (2.3953 × height in cm), where sex is denoted by “1” for men and “0” for women). The final calculated tracheal cross-sectional area of the patient in the present case was 247.5734 mm2. According to the height-based nomogram for endotracheal tube size selection derived from the CT-imaging study by Cao et al.,8 the final predicted endotracheal tube size of the patient was 6.5 or 7.0 mm. Theoretically, according to the above two selection methods, the cuff of the endotracheal tube can effectively seal the airway when the intracuff pressure is 30 cmH2O. However, the true tracheal cross-sectional area of the patient in the present case was unusual.
The cuff seals the airway during mechanical ventilation. An endotracheal cuff pressure of 20–30 cmH2O is adequate for most patients, but lack of a tracheal seal still occurs in a small number of patients.9, 10 The airway of the patient in our case could be completely sealed only when the cuff pressure of the endotracheal tube reached 100 cmH2O. The diagnosis of cuff undersizing was made by chest X-ray CT. Our main finding was that the actual cross-sectional area of the airway was significantly larger than the cross-sectional area of the cuff. The real cross-sectional area of the airway in our patient obviously exceeded that of the general population. Thus, this case illustrates the importance of rapid diagnosis of undersizing by chest CT to prevent mismatch between the cuff and airway to ensure that the selected endotracheal tube matches the patient's airway.
Consensus suggests that the cuff pressure of the endotracheal tube should range from 20 to 30 cmH2O.1 Excessively high or low cuff pressures have been associated with complications such as tracheal stenosis, air leakage, microaspiration of secretions, and ventilator-associated pneumonia.11 As shown in Figure 1, the cross-sectional area of the trachea was significantly larger than the cross-sectional area of the cuff; thus, only when the cuff pressure was 100 cmH2O could the cuff seal the airway. According to expert consensus, such patients are prone to ventilator-associated pneumonia.
5 CONCLUSIONThe cross-sectional area of the trachea should be periodically evaluated by chest CT during anesthesia to assure that mismatch is not present. When the intracuff pressure is 20–30 cmH2O, some patients' trachea cannot be effectively sealed.
ACKNOWLEDGEMENTSNo external funding or competing interests declared.
CONFLICTS OF INTERESTSThe authors declare that they have no competing interests.
AUTHOR CONTRIBUTIONHong-Lei Wu and Pei-pei Ji: were actively involved in the clinical care of the patient. Hong-Lei Wu and Yan-Man Zhang: wrote the manuscript. Jia-hai Shi and Wang-Qin Shen: revised the manuscript.
ETHICAL APPROVALThis case report is a small part of our big study. All patients provided informed consent for inclusion before they participated in the study. The study was registered with the Chinese Clinical Trial Registry (ChiCTR-COC-15006459) on 29 May 2015.
CONSENTWritten informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor in chief of this journal.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
1Wang WZ, Zhou YY, Wang ZJ, et al. A mobile terminal application program was used for endotracheal tube cuff pressure measurement. J Clin Monit Comput. 2021; 35(3): 463- 468. 2Peters JH, Hoogerwerf N. Prehospital endotracheal intubation; need for routine cuff pressure measurement? Emerg Med J. 2013; 30(10): 851- 853. 3Ritchie-Mclean S, Ferrier V, Clevenger B, et al. Using middle finger length to determine the internal diameter of uncuffed tracheal tubes in paediatrics. Anaesthesia. 2018; 73(10): 1207- 1213. 4Cole F. Pediatric formulas for the anesthesiologist. AMA J Dis Child. 1957; 94(6): 672- 673. 5Motoyama EK. Anesthesia and the upper airway in infants and children. Int Anesthesiol Clin. 1992; 30(4): 17- 19. 6Nazari R, Salehpour OM, Sharif NH, et al. Effect of head position change on endotracheal cuff pressure in mechanically ventilated patients: a quasi-experimental study. Tanaffos. 2020; 19(2): 129- 134. 7Aljathlany Y, Aljasser A, Alhelali A, et al. Proposing an endotracheal tube selection tool based on multivariate analysis of airway imaging. Ear Nose Throat J. 2020; 100(5_suppl): 629S- 635S. 8Cao AC, Rereddy S, Mirza N. Current practices in endotracheal tube size selection for adults. Laryngoscope. 2020; 131(9): 1967- 1971. 9Harvie DA, Darvall JN, Dodd M, et al. The minimal leak test technique for endotracheal cuff maintenance. Anaesth Intensive Care. 2016; 44(5): 599- 604. 10Hongyun T, Xiuling C, Wanjie Y, et al. A clinical study on the determination of cuff pressure in artificial airway by minimum air leakage method. Chin Crit Care Med. 2020; 32(4): 439- 442. 11Vorobeichik L, Yoo SJ, Cybulski KA. Inadvertent endotracheal cuff hyperinflation diagnosed by magnetic resonance imaging. Anesthesiology. 2018; 128(1): 141.
Comments (0)