
Remember me




Idiopathic pneumonia syndrome (IPS) is a spectrum of acute interstitial lung injuries observed after the early posthematopoietic stem cell transplantation (HSCT) period. IPS diagnosis should be confirmed to exclude lower respiratory tract infection, cardiac dysfunction, acute renal failure, and fluid overload.1, 2 The cumulative incidence of IPS increases from 2% to 10% according to the strength of conditioning, and its onset occurs at 4–106 (median, 19) days after HSCT.1 The prognosis is exceedingly poor, with mortality rates of 60%–80% in most studies.1, 3 Thus, novel therapeutic strategies are required for HSCT-related IPS.
In human idiopathic pulmonary fibrosis (IPF), Janus kinase (JAK) 2 and signal transducer and activator of transcription (STAT) 3 are activated.4 Thus, their dual inhibitor is implicated as a potential therapeutic strategy for IPF.5 Ruxolitinib is a selective JAK1 and JAK2 inhibitor approved for the treatment of myeloproliferative neoplasms and steroid-refractory acute and chronic graft-versus-host disease (GVHD).6-9 Ruxolitinib blocks JAK1, JAK2, and STAT signaling pathways, suppresses immune responses, and has positive effects on interstitial pneumonia associated with idiopathic juvenile arthritis, bronchiolitis obliterans after HSCT, and COVID-19-related acute respiratory distress syndrome.10-13 In this study, we report administration of ruxolitinib in a patient with myelodysplastic syndrome (MDS) who developed IPS after second HSCT.
2 CASE PRESENTATIONAn 11-year-old girl presented with recurrent fever, prolonged leukopenia, and anemia for several months. Repeated bone marrow aspirations revealed hypocellular marrow with trilineage dysplasia. Blasts (8.8% of nucleated cells) were negative for specific and nonspecific esterases. Flow cytometry analysis revealed that the blasts expressed CD13, CD15, CD33, CD38, CD58, CD117, HLA-DR, and cytoplasmic myeloperoxidase. Chromosomal G-banding detected 46, XX, −5, −7, −9, −10, −13, −14, +6 mar in 14 of 20 cells that were analyzed. Spectral karyotyping-fluorescence in situ hybridization (SKY-FISH) revealed complex chromosomal aberrations with three chromosomal translocations involving chromosome 7. DNA-FISH revealed 7q31 deletion in 88% of cells. Taken together, she was diagnosed with MDS-EB-1.
She underwent AML99 protocol remission induction therapy and achieved complete remission.14 One course of intensification therapy was conducted, followed by HSCT from her HLA-haploidentical mother with post-transplantation cyclophosphamide. Conditioning regimen was fludarabine 120 mg/m2 total dose, busulfan every 6 h for 16 doses (target AUC, 75 mg/L*h), and melphalan 140 mg/m2 total dose (Table 1). GVHD prophylaxis was provided by cyclophosphamide 50 mg/kg/dose i.v. on days 3 and 4, followed by mycophenolate mofetil 15 mg/kg orally three times daily from days 5 to 35, and tacrolimus i.v. daily (Table 1). However, hemophagocytic lymphohistiocytosis (HLH) developed after transplantation, and the donor cells were rejected. CT scan showed no evidence of active pneumonia on day 50 after first HSCT (Figure 1A). Second HSCT was conducted by HLA 6/8-matched cord blood transplantation (CBT) on day 65 after first HSCT (Table 1). Conditioning regimen was fludarabine 125 mg/m2 total dose, etoposide 450 mg/m2 total dose, melphalan 80 mg/m2 total dose, and total body irradiation 4 Gy (Table 1). GVHD prophylaxis was tacrolimus and short methotrexate (Table 1). Engraftment syndrome developed with desaturation and oxygen requirement on day 9. Methylprednisolone (1 mg/kg/day) was initiated on day 16. Oxygenation gradually improved, and oxygen was discontinued on day 24. Neutrophil engraftment was achieved on day 29.
TABLE 1. Transplantation characteristics and clinical outcomes 1st transplantation 2nd transplantation Interval (d) – 65 Donor Haploidentical mother UCBHLA disparity
Mismatched alleles
5/8
B, C, DR
6/8
B, DR
Source BM CB ConditioningBu (cAUC 75 mg*h/L)
Flu (120)
Mel (140)
Flu (125)
Mell (80)
VP−16 (450)
TBI 4 Gy
GVHD prophylaxisCy
MMF
TAC
MTX
TAC
ComplicationsHLH
Cystitis
HLH
IPS
Acute GVHD grade II (gut)
TMA
Outcome RejectionAlive (day 524)
Chimerism >95% (day 365)
Abbreviations: BM, bone marrow; Bu, busulfan; CB, cord blood; Flu, fludarabine; GVHD, graft-versus-host disease; HLA, human leukocyte antigen; HLH, hemophagocytic lymphohistiocytosis; IPS, idiopathic pneumonia syndrome; Mel, melphalan; MMF, mycophenolate mofetil; MTX, methotrexate; TAC, tacrolimus; TBI, total body irradiation; TMA, thrombotic microangiopathy; UCB, unrelated cord blood; VP-16, etoposide.
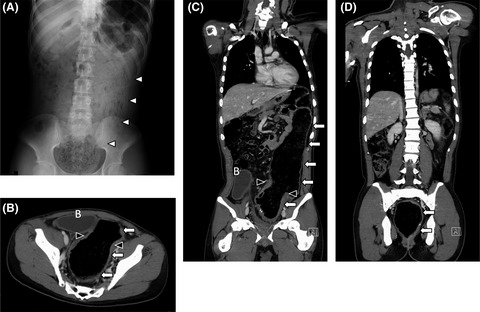
Radiographic findings for the patient. (A) CT scan before the second transplantation on day 15. (B) CT scan at presentation of idiopathic pulmonary syndrome (IPS) on day 61. Left panel shows slightly dominant ground-glass opacities (GGO) on the dorsal lungs. Right panel shows a sagittal view of the CT scan with GGO infiltration throughout the lungs. (C) IPS progression on day 69, at 5 days before ruxolitinib administration. GGO progression is observed in the entire lungs (left and right) with infiltration in the dorsal part of the pleural membranes (left). (D) CT scan on day 96 after 13 days of ruxolitinib administration (left and right), showing resolution of GGO
The patient developed stage III gut GVHD around day 30 that was refractory to methylprednisolone and started budesonide (6 mg/day) orally once daily on day 55. However, budesonide was discontinued on day 64 due to thrombotic microangiopathy with continuous low haptoglobin below the cut off and increased transfusion requirements (Figure 2A). Oxygenation gradually decreased with progressing nonproductive cough and dyspnea along with elevation of serum KL-6 and surfactant protein D (SP-D) around day 50 after CBT (Figure 2A,B). CT scan showed remarkable progression of infiltration in the entire lung fields on days 61 and 69 (Figure 1B,C). Respiratory condition deteriorated, and high-flow nasal cannula (HFNC) oxygenation was required on day 73 (Figure 2A). Cardiac dysfunction, renal failure, and iatrogenic fluid overload were absent. Multiplex PCRs including cytomegalovirus, Pneumocystis jirovecii, SARS-CoV-2, and other viral pathogens, as documented in the Appendix S1, were negative in sputum specimens. Beta-d-glucan was not elevated in this condition. Although invasive procedures such as lung biopsy and bronchoalveolar lavage could not be applied to the patient because of the poor respiratory condition, we considered the patient to have IPS concomitant with GVHD and HLH. Six of the eight HLH 2004 diagnostic criteria were fulfilled, namely, fever, splenomegaly, pancytopenia, hypertriglyceridemia (maximum, 5180 mg/dl), hemophagocytic lymphocytes in bone marrow, and hyperferritinemia (maximum, 17,509 ng/ml).15 We conducted methylprednisolone pulse therapy (10 mg/kg/day, 3 days). Furthermore, based on a recent report regarding resistance to steroid and antitumor necrosis factor therapy in patients with IPS,16 we simultaneously started ruxolitinib (20 mg/day) on day 74 (Figure 2A). Because ruxolitinib was not approved for refractory GVHD in Japan, administration of ruxolitinib was approved by the Evaluation Committee for Unapproved or Off-label Drugs at Tokyo Medical and Dental University (No: 2019-038), and written informed consent was obtained from a parent of the patient. Respiratory status remarkably improved, with successful cessation of HFNC oxygenation on day 85 and no further requirement for oxygenation on day 89 (Figure 2A). CT scan revealed no infiltration shadows on day 96 (Figure 1D). Stool condition also gradually improved after ruxolitinib administration and became normal on day 91 (Figure 2A). Although SP-D rapidly decreased during the first month, KL-6 slowly reduced over 2 months (Figure 2B). Serum ferritin, soluble interleukin-2 receptor (sIL-2R), and C-reactive protein (CRP) sharply improved (Figure 2B). Neutropenia (grade 3), anemia (grade 3), and thrombocytopenia (grade 3) were manageable by reduction in ruxolitinib to 5 mg/day on day 131 (Figure 2C). However, KL-6 started to elevate, and ruxolitinib was increased to 10 mg/day on day 145 (Figure 2B). Complete chimerism was confirmed by short-tandem repeat analysis on days 64, 98, and 365. The MDS clone was not detected by chromosome 7q deletion FISH on days 98 and 365. Ruxolitinib and tacrolimus were successfully stopped on days 378 and 519, respectively. The patient has remained without any respiratory symptoms with stable KL-6, after cessation of ruxolitinib and tacrolimus (Figure 2B).

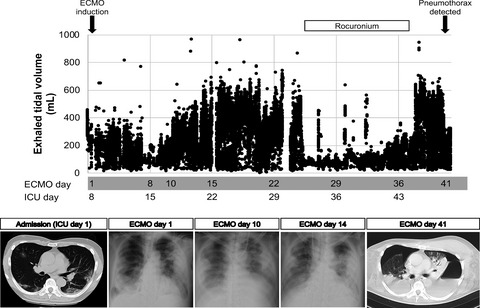
Clinical findings for the patient. (A) Active phase of gut graft-versus-host disease (GVHD) and idiopathic pulmonary syndrome (IPS) from days 32 to 93. Upper panel shows immunosuppressive treatments including budesonide, methylprednisolone (mPSL), tacrolimus, and ruxolitinib. Middle panel shows oxygen requirements during the active phase of IPS. Nasal cannula (NC) oxygenation was started on day 57. High-flow nasal cannula (HFNC) oxygenation was started on day 73. Bottom panel shows exaggeration of diarrhea on day 32. Counts of diarrhea per day are shown. Stool condition normalized on day 91. FiO2 inspired oxygen concentration. (B) Entire clinical course for second hematopoietic stem cell transplantation from days 16 to 330. Upper panel shows immunosuppressive treatments including mPSL, tacrolimus, and ruxolitinib. Middle panel shows IPS markers including KL-6 and pulmonary surfactant protein D (SP-D). Bottom panel shows inflammatory markers including ferritin, soluble IL-2 receptor (sIL-2R), and C-reactive protein (CRP). (C) Upper panel shows white blood cell (WBC), neutrophil (Neu), and lymphocyte (Ly) counts. Bottom panel shows hemoglobin (Hb) levels and platelet counts with red blood cell (RBC) and platelet concentrate (PC) transfusions
3 LITERATURE SEARCHWe searched for relevant literature using the key phrase “idiopathic pneumonia syndrome hematopoietic transplantation” in PubMed. Among 127 articles identified, we selected 11 articles after excluding case reports, duplicates, meta-analyses, reviews, text in languages other than English, biological studies, other lung complications, and autologous stem cell transplantation. The incidences of IPS were 6.7%–11.8% in children and 8.3%–12% in adults with myeloablative conditioning, which tended to be higher than the corresponding rates in patients with nonmyeloablative conditioning. Despite treatments involving steroids, positive pressure ventilation, mechanical ventilation, and anti-inflammatory biologics, the mortality rates of IPS were 55%–87.5% in children and 70%–85% in adults. Prospective studies using etanercept showed high response rates in children but found resistance in adults (Table 2).
TABLE 2. Literature review: transplantation characteristics and clinical outcomes of IPS in retrospective cohort and prospective studies Author (Year; ref.) IPS N (Total N of SCT), % Age group Disease type HLA N (%) Donor type N (%) Conditioning N (%) Treatment N (%) Outcome N (%) GVHD before onset of IPS N (%) Pediatric retrospective Keates-Baleeiro (2006)25 11 (93), 11.8% 8 (0.6–20) ALL, AML, CML, MDS, Hurler syndromeMRD 9.1%,
MMRD 90.9%
BM 72.7%
CB 27.3%
Myeloablative (Cy + TBI 12 Gy) 63%
Nonmyeloablative (non-TBI) 37%
Mechanical ventilation 4 (36.4%)
PAP 1 (9.1%)
Oxygen 6 (54.5%)
8 (72.7%) died 100% Sakaguchi (2012)26 20 (251), 8% 6.6 (0.9–15.2)Hematological malignancy
Malignant solid tumors
Benign disease
MRD 7 (35.0%)
MURD 3 (15.0%)
MMRD 3 (15.0%)
MMURD 1 (5.0%)
MMCB 3 (15.0%)
Auto 2 (10.0%)
BM 15 (75.0%)
CB 3 (15.0%)
Auto-HCT 2 (10.0%)
TBI-containing 7 (35.0%)
Bu-containing 12 (60.0%)
Steroid therapy 19 (95.0%)
Mechanical ventilation 9 (45.0%)
Infliximab 2 (10.0%)
Basiliximab 1 (5.0%)
11 (55.0%) died within 5 years of HCT
7 (35.0%) grade II–IV Sano (2014)17 14 (210), 6.7% 9.5 (0–16) ALL, AML, MDS, non-malignantMatched 50%
Mismatched 50%
BM 57.1%
PB 7.1%
CB 35.7%
Myeloablative 11 (78.6%)
Nonmyeloablative 3 (21.4%)
High-dose steroid 12 (86%)
Mechanical ventilation 9 (64%)
10 (71.4%) died within 120 days of HCT
11 (78.6%) died within 365 days of HCT
2 (14.3%) grade I–II
5 (35.7%) grade III–IV
Altman (2018)27 8 (313), 2.9% NA ADA, CHARGE, RAG1, RAG2, JAK3, CgC, ArtemisMRD 2 (25%)
MURD 3 (37.5%)
MMRD 3 (37.5%)
BM 4 (50%)
CB 4 (50%)
None 2 (25%)
Bu 1 (12.5%)
Bu + Cy 1 (12.5%)
Flu + Mel 1 (12.5%)
Treo + Cy 1 (12.5%)
Treo + Flu 2 (25%)
Mechanical ventilation 7 (87.5%)1 (12.5%) alive
7 (87.5%) died
2 (25%) grade I
1 (12.5%) grade II
1 (12.5%) cGVHD
Pediatric prospective Yanik (2015)28 28 11 (1–17) ALL, AML/MDS, lymphoma, non-malignantRelated 4 (14%)
Unrelated 24 (86%)
BM 14 (50%)
PB 3 (11%)
CB 11 (39%)
TBI containing 14 (50%)
TBI not containing 14 (50%)
Myeloablative 27 (96%)
Nonmyeloablative 1 (4%)
Etanercept and corticosteroidsOS 89% at day 28
OS 75% at day 56
OS 63% at 1 year
NA Adult retrospective Fukuda (2003)29 77 (917), 8.4% 41 (1–66) AA, AL, CML, MDS, Lymphoma, CLL, MM, PID, etc.MRD 46.8%,
MMRD 6.0%,
Unrelated 47.2%
PB 34.6%,
BM 65.4%
Myeloablative 917 (83.3%) Mechanical ventilation 50 (62%) 60 (74%) died 25% grade III–IV 4 (183), 2.2% 53 (1–73)MRD 65.6%,
Unrelated 34.4%
PB 90.7%
BM 9.3%
Nonmyeloablative 183 (16.7%) 21% grade III–IV Yanik (2008)30 15 21 (1–60) AA, ALL, AML, MDS, CML, NHL, PIDMRD 13.3%
MURD 69.2%
MMURD 20%
PB 46.7%
BM 46.7%
CB 6.7%
Myeloablative 13 (86.7%)
Nonmyeloablative 2 (13.3%)
Etanercept 15 (100%)
Mechanical ventilation 8 (53.3%)
Oxygen 15 (100%)
12 (80%) died6 (40%) grade II
3 (20%) grade III–IV
Zhu (2008)31 23 (192), 12% 24.3 (5–45) ALL, AML, CMLMRD 6 (26.1%)
MURD 9 (39.1%)
MMRD 5 (21.7%)
MMURD 3 (13.0%)
NA Bu + Cy PAP or mechanical ventilation 20 (87%)3 (13%) survived without PAP and mechanical ventilation
16 (69.6%) died within 120 days of HCT
20 (87.0%) died within 365 days of HCT
19 (82.6%) aGVHD
11 (47.8%) grade III–IV
16 (69.6%) aGVHD of gut
Vande Vusse (2016)32 75 (906), 8.3% 44 (32-56) AL, CL, MDS, lymphoma, otherMRD 33 (44%)
MMRD 2 (3%)
Unrelated 40 (53%)
BM 49 (65%)
PB 26 (35%)
Non-TBI 21 (28%)
TBI 12 35 (47%)
TBI > 12 19 (25%)
NA(76%) died within first 120 days of HCT
(85%) died within first 2 years of HCT
37% severe GVHD Wenger (2020)33 67 (1829), 3.7% 51.9 (37.9–58.3) ALL, AML, CML, MDS, lymphoma, CLL, MMMRD 35.8%
MURD 31.4%
MMURD 17.9%
PB 62.7%
BM 22.4%
CB 14.9%
Nonmyeloablative 25 (37.3%)
Myeloablative TBI < 12 Gy 20 (29.9%)
Myeloablative TBI > 12 Gy 22 (32.8%)
Mechanical ventilation 39 (58%)31 (46.3%) died within 120 days of HCT
47 (70.1%) died within 365 days of HCT
11 (16.4%) grade III–IV) Adult prospective Yanik (2014)34 16 47.9 (22.9–70.1) AML, MDS, ALL, lymphoma, other NA NAMyeloablative 9 (56.2%)
Nonmyeloablative 7 (43.8%)
Etanercept OS 23% at 1 year NA 18 47.8 (21.8–68.8)Myeloablative 11 (61.1%)
Nonmyeloablative 7 (38.9%)
Placebo OS 17% at 1 year Abbreviations: AA, aplastic anemia; ADA, adenosine deaminase; AL, acute leukemia; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; Auto, autologous; BM, bone marrow; Bu, busulfan; CB, cord blood; CgC, common gamma chain; CL, chronic leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myelogenous leukemia; Cy, cyclophosphamide; Flu, fludarabine; GVHD, graft-versus-host disease; HCT, hematopoietic cell transplantation; HLA, human leukocyte antigen; IPS, idiopathic pneumonia syndrome; JAK, Janus kinase; MDS, myelodysplastic syndrome; Mel, melphalan; MM, multiple myeloma; MMCB, mismatched cord blood; MMRD, mismatched related donor; MMURD, mismatched unrelated donor; MRD, matched related donor; MURD, matched unrelated donor; N, number; NHL, non-Hodgkin's lymphoma; OS, overall survival; PAP, positive airway pressure; PB, peripheral blood; PID, primary immunodeficiency; RAG, recombination activating gene; TBI, total body irradiation; Treo, treosulfan; UCB, unrelated cord blood. 4 DISCUSSIONThe findings for the present case suggest that ruxolitinib is effective with permissible adverse effects for HSCT-related IPS. Rapid resolution of respiratory symptoms, gut GVHD, secondary HLH, radiographic findings, and inflammatory markers was observed. Transfusion independence, methylprednisolone discontinuation, hospital discharge, and management in the outpatient setting were also achieved after ruxolitinib administration.
Patients with IPS following HSCT tended to develop acute GVHD (grades II–IV) compared with non-IPS patients.17 The IPS group contained more patients with prior HSCT.17 Thus, IPS etiology may involve combined effects of cellular injury, including toxic effects of conditioning, immune-mediated injury, and occult infections.1, 2 Consistent with these past reports, our patient developed IPS plausibly associated with repeated conditioning for second HSCT, steroid-refractory GVHD, and secondary HLH. Ruxolitinib effectively alleviated not only progressive IPS but also all of the other complications.
Ruxolitinib is a potent and selective inhibitor of JAK1 and JAK2, has strong selectivity against JAK3, and modestly inhibits Tyk2.13 Ruxolitinib maximally inhibited cytokine-induced phosphorylated STAT3 (pSTAT3) at 1–2 h after administration. A return to normal pSTAT3 was observed 24 h after cessation of ruxolitinib.18 In an animal model, a dual inhibitor of JAK2 and STAT3 alleviated bleomycin-induced lung fibrosis along with reduction in collagen deposition.4 In the clinical setting, ruxolitinib potentially inhibited JAK/STAT pathway-derived cytokines, including IL-6, IFN-gamma, and several others associated with refractory GVHD, primary or secondary HLH, IPF, and COVID-19-related acute respiratory distress syndrome.4, 12, 19-23 Remarkable reductions in ferritin and sIL-2R were observed in our patient, resembling the reported response pattern for secondary HLH.21, 23 KL-6 and SP-D were useful markers for tracking the patient's disease status.
Plasma IL-6 is significantly elevated in patients with IPS, and pulmonary-derived IL-6 often exacerbates IPS, leading to resistance to steroids and antitumor necrosis factor therapy.16 We speculate that the elevated CRP in our patient may have been due to IL-6 dysregulation.24 Although no definite conclusion can be drawn without measuring the cytokine profiles, including the IL-6 concentration, the reduction in CRP along with other inflammatory markers in our patient plausibly reflected IL-6/JAK/STAT pathway inhibition after ruxolitinib administration (Figure 2B).
In conclusion, ruxolitinib was effective for IPS without any severe adverse effects except for manageable pancytopenia in our patient. Ruxolitinib may be an alternative choice for not only HSCT-related IPS under steroid-refractory GVHD but also other secondary cytokine-mediated interstitial lung diseases. However, this study involves only one case without measurement of precise cytokine profiles. Further prospective studies are warranted to determine whether ruxolitinib salvage therapy is effective for IPS after HSCT.
ACKNOWLEDGEMENTSThis work was supported in part by the Grants-in-Aid for Young Scientists (18K15661 and 21H02878). The authors thank Ms. Naomi Terada at the Department of Pediatrics and Developmental Biology, Tokyo Medical and Dental University (TMDU), for performing the multiplex PCR on the patient's sputum samples, and staff at the Department of Laboratory Medicine, TMDU, for performing the SARS-CoV-2 PCR. The authors also thank Alison Sherwin, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
CONFLICT OF INTERESTThe authors declare that they have no conflict of interest regarding this article.
AUTHOR CONTRIBUTIONSAll authors contributed to conception and design of the study. DT, TI, NM, MY, AM, TT, TO, TK, and MY contributed to data acquisition. DT, TI, NM, MY, and TT contributed to systematic review. All authors contributed to analysis and/or interpretation of data. DT, TI, HK, and MT drafted the manuscript. All authors critically revised the manuscript for important intellectual content. All authors reviewed the manuscript before publication.
CONSENTWritten informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Filename Description ccr35242-sup-0001-Appendixs1.docxWord 2007 document , 22.3 KB Appendix s1Please note: The publisher is not responsible for the content or functionality of any supporting information supplied by the authors. Any queries (other than missing content) should be directed to the corresponding author for the article.
REFERENCES
1Cheng G-S, Madtes DK. Acute pulmonary complications of bone marrow and stem cell transplantation. In: JS Lee, MP Donahoe, eds. Hematologic Abnormalities and Acute Lung Syndromes. Springer International Publishing; 2017: 147- 171. 2Haider S, Durairajan N, Soubani AO. Noninfectious pulmonary complications of haematopoietic stem cell transplantation. Eur Respir Rev. 2020; 29(156):190119. 3Broglie L, Fretham C, Al-Seraihy A, et al. Pulmonary complications in pediatric and adolescent patients following allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2019; 25(10): 2024- 2030. 4Milara J, Hernandez G, Ballester B, et al. The JAK2 pathway is activated in idiopathic pulmonary fibrosis. Respir Res. 2018; 19(1): 24. 5Damsky W, Peterson D, Ramseier J, et al. The emerging role of Janus kinase inhibitors in the treatment of autoimmune and inflammatory diseases. J Allergy Clin Immunol. 2021; 147(3): 814- 826. 6Verstovsek S, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012; 366(9): 799- 807. 7Vannucchi AM, Kiladjian JJ, Griesshammer M, et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera. N Engl J Med. 2015; 372(5): 426- 435. 8Zeiser R, von Bubnoff N, Butler J, et al. Ruxolitinib for glucocorticoid-refractory acute graft-versus-host disease. N Engl J Med. 2020; 382(19): 1800- 1810. 9Zeiser R, Polverelli N, Ram R, et al. Ruxolitinib for glucocorticoid-refractory chronic graft-versus-host disease. N Engl J Med. 2021; 385(3): 228- 238. 10Uygun V, Karasu G, Daloglu H, et al. Ruxolitinib salvage therapy is effective for steroid-refractory graft-versus-host disease in children: a single-center experience. Pediatr Blood Cancer. 2020; 67(4):e28190. 11Bader-Meunier B, Hadchouel A, Berteloot L, et al. Effectiveness and safety of ruxolitinib for the treatment of refractory systemic idiopathic juvenile arthritis like associated with interstitial lung disease: a case report. Ann Rheum Dis. 2020:2020-216983. 12Cao Y, Wei J, Zou L, et al. Ruxolitinib in treatment of severe coronavirus disease 2019 (COVID-19): a multicenter, single-blind, randomized controlled trial. J Allergy Clin Immunol. 2020; 146(1): 137- 146.e133. 13Quintás-Cardama A, Vaddi K, Liu P, et al. Preclinical characterization of the selective JAK1/2 inhibitor INCB018424: therapeutic implications for the treatment of myeloproliferative neoplasms. Blood. 2010; 115(15): 3109- 3117. 14Nakayama H, Tabuchi K, Tawa A, et al. Outcome of children with relapsed acute myeloid leukemia following initial therapy under the AML99 protocol. Int J Hematol. 2014; 100(2): 171- 179. 15Henter JI, Horne A, Aricó M, et al. HLH-2
Comments (0)