
Remember me




Invasive cribriform carcinoma (ICC) is a rare type of invasive breast carcinoma that was first described by Page et al. in 19831, accounting for approximately 0.4% of all primary breast carcinomas.1-4 Its main characteristic is a unique structure with most of its invasive components arranged in a cribriform pattern. The prognosis of patients with pure and classical ICC is excellent.1-3 This case was incidentally discovered on Computed tomography (CT) as part of a preoperative examination for gynecological surgery. This quite rare case is reported along with a literature review.
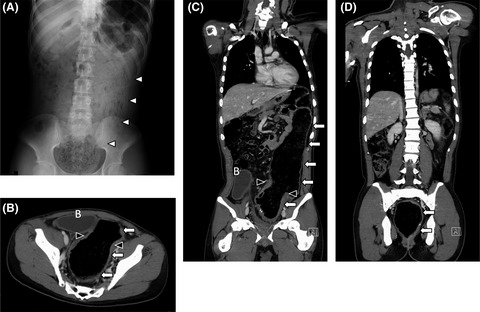
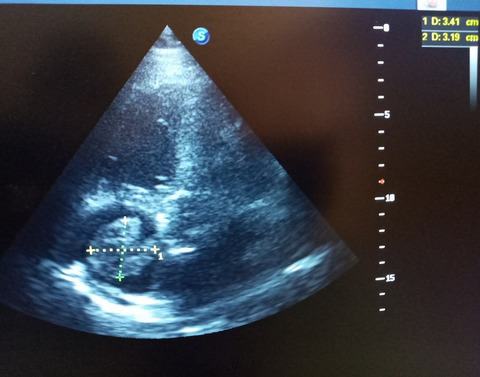
2 CASE REPORTA 68-year-old woman was scheduled to undergo surgery for pelvic organ prolapse at the Department of Obstetrics and Gynecology in our institute. No family member of the patient had a history of breast or ovarian carcinoma. Contrast-enhanced CT performed as part of the preoperative examination showed a 1.4-cm-diameter tumor in the upper lateral quadrant of the left breast (Figure 1A,B). The tumor shadow was suspected to be a breast carcinoma, and the patient was referred to our department. The patient had no complaints of nipple discharge or pain. On physical examination, there was a mobile, irregular mass of 1 cm in the largest clinical diameter. In the preoperative diagnostic workup, the patient underwent a bilateral mammogram (MMG) which showed a high-density mass with no calcification in the breast parenchyma, highly suspicious for malignancy (Figure 1C). Breast ultrasonography (US) showed a 1.3-cm, irregularly shaped, hypoechogenic mass (Figure 1D). Serum tumor markers were within normal limits. A core needle biopsy of the mass demonstrated malignant cells proliferating in a cribriform or papillary pattern.

Preoperative examination (Plain CT, MMG, US). (A and B) Plain CT shows an irregularly shaped tumor (arrow) with a diameter of 14 mm in the upper-outer region of the left mammary gland. No left axillary lymphadenopathy is observed. (C) MMG in the medio-lateral oblique view, a tumor shadow (arrow heads) is seen in the upper region of the left mammary gland. (D) US shows a 1.3-cm, irregularly shaped, hypoechogenic mass in the upper-outer region of the left mammary gland
With a diagnosis of invasive ductal carcinoma, tubule forming type, in the upper lateral quadrant of the left breast, the patient underwent total mastectomy and sentinel lymph node biopsy. The patient chose total mastectomy to avoid postoperative radiotherapy. As a result, it was no longer necessary to evaluate the test for intraductal extension, and intensive MRI was not performed. Intraoperative pathological examination confirmed that the two sentinel lymph nodes sampled in the axilla were negative for metastasis, and no axillary node dissection was performed.
The surgical specimen contained a hard, grayish, solid, and lobulated tumor with defined margins with a diameter of 1.5 cm (Figure 2A). Microscopically, the tumor was composed entirely of packed epithelial islands with a cribriform appearance (Figure 2B). The islands were irregularly shaped with an ovoid outline and separated by relatively thin fibrous connective tissue. Well-defined, rounded spaces (cribriform growth pattern) were formed within the islands, and proliferating tumor cells were columnar and rather uniform, having rounded to ovoid nuclei with nuclear pleomorphism grade of G1 (Figure 2C). Cribriform ductal carcinoma in situ (DCIS) was seen around the tumor; on pathological examination, total tumor area was 2.7 cm × 1.5 cm and invasive area was 1.5 cm × 1.0 cm. No lymphovascular invasion was identified, and the surgical margins were free of the tumor. On immunohistochemistry, the tumor islands had no positive cells for the myoepithelial marker CD10 (Figure 3B), whereas myoepithelial cells were preserved around the DCIS (Figure 3A). The tumor was classified as an invasive cribriform carcinoma of pure type. Nuclear immunoreactivity was strong for both estrogen receptor (ER) and progesterone receptor (PgR) and seen in 90% of the tumor cells (Figure 3C,D). Human epidermal growth factor receptor 2 (HER2) expression was absent (Figure 3E), and the Ki-67 labeling index was low (7%) (Figure 3F). Two axillary sentinel lymph nodes were examined intraoperatively and showed no metastasis. In accordance with the 8th edition of the Union for International Cancer Control (UICC) TNM classification, the tumor was staged as StageⅠA (pT1cN0M0).

Findings of the resected specimen, (A) Grayish white, solid, and lobulated tumor (arrow) in the mammary gland. (B) HE staining shows tumor cells growing in a cribriform, partly papillary pattern in a low-power field. (C) Most of the tumor shows a cribriform pattern in the high-power field

Immunohistological findings. (A) Tumor islands have no positive cells for CD10, whereas myoepithelial cells are preserved around the DCIS. (B) No CD10-positive cells were found in the invasive cribriform cancer area. (C) ER is strongly stained. (D) PgR is strongly stained. (E) HER2 expression is judged as score 0. (F) Ki-67 staining is observed in 7% of all cells
The patient is presently free from local recurrence and metastasis 10 months after surgery on adjuvant hormone therapy. We are treating with an aromatase inhibitor, and planning 5 years of treatment.
3 DISCUSSIONInvasive cribriform carcinoma is a unique type of invasive breast carcinoma that was first described by Page et al. in 1983.1 ICC consists of invasive epithelial islands containing well-defined, rounded spaces similar in appearance to cribriform-type ductal carcinoma in situ (DCIS). The islands have an ovoid or angular outline and are set within a desmoplastic stroma. They consist of multilayered epithelial cells of small to intermediate size, forming secondary glandular structures lined by cuboidal to columnar cells. The World Health Organization (WHO) classification (5th edition) requires an invasive breast carcinoma to have >90% of the tumor composed of cribriform islands of epithelial cells with low-grade nuclei and sparse mitoses. ICCs are typically ER-positive (95%–100%), PgR-positive (69%–89%) and HER2-negative.5, 6 The present case showed that most of the tumor showed a cribriform pattern and was classified as pure ICC. Pure ICC tends to have a smaller tumor size and a lower rate of lymph node metastasis than mixed ICC.4 However, there is no report yet on whether there is a difference in prognosis between the two types.
Adenoid cystic carcinoma (ACC) and secretory carcinoma (SC) may also exhibit cribriform patterns. However, the cribriform spaces in ACC lesions contain basaloid cells (myoepithelial-like cells) and basement membrane material, and they are negative for ER, PgR, and HER2.7 SC characterize to present with extensive secretion, and is positive for a-lactoalbumin in the cytoplasm of the tumor cells.8
The radiological features of ICC are indistinguishable from those of other breast carcinomas.9 The image findings of the present case showed no diagnostic features.
The mortality rate of patients with ICC is reported to be lower than that of those with non-specific types of invasive ductal carcinoma (IDC), and the 5-year survival rate is reported to be over 95%2, 3, 5, 10 The reasons for the excellent prognosis of ICC seem to be related to its characteristics. First, tumor size tends to be small, less than 2 cm, 75% of which are T1a to T1c. Second, ICC has less nodal metastasis. Third, ICC has higher rates of positive ER and PgR staining, which means that it is hormone-sensitive, and negative HER2 expression.
In fact, ICC pathologically has smaller tumor diameters than IDC, and has a higher rate of lumpectomy in the previous study by Liu et al. However, in this case, the tumor diameter of the invasive cancer was 1.5 × 1.0 cm, but the pathological tumor size was 2.7 × 1.5 cm, which was 1.2 cm larger. Although ICC is a tumor type with a good prognosis, we must consider the intraductal growth of the tumor and measure the exact size of the tumor in ICC cases. ICC requires rapid intraoperative pathological diagnosis and postoperative radiation therapy, and if not, ICC is a tumor type that should be considered for total mastectomy.
There is no consensus on ICC drug therapy yet. Colleoni recommended that favorable luminal special type tumors may be suitable for no therapy or endocrine therapy alone.11 However, one must be cautious to make the decision. The case of pure ICC could still have distant metastases (bones) if left untreated for a long period of time (13 years).12
The patient is doing well and remains disease-free 10 months after surgery on adjuvant hormone therapy.
4 CONCLUSIONA case of pure ICC of the breast with a good prognosis was presented. Further studies of more patients with longer follow-up are needed.
CONFLICT OF INTERESTThe authors declare that they have no competing interests.
AUTHOR CONTRIBUTIONSYasuhiro Adachi drafted the manuscript. Takefumi Katsuki drafted and proofed the manuscript. Takakazu Sasaguri and Keiji Hirata proofed the manuscript. Naoki Nagata had given final approval of the version to be published. All authors read and approved the final manuscript.
ETHICAL APPROVALNot applicable.
CONSENTThe patient provided written, informed consent to publish this case report and any accompanying images.
The data are not available for public access because of patient privacy concerns but are available from the corresponding author on reasonable request.
REFERENCES
1Page DL, Dixon JM, Anderson TJ, Lee D, Stewart HJ. Invasive cribriform carcinoma of the breast. Histopathology. 1983; 7: 525- 536. 2Marzullo F, Zito FA, Marzullo A, et al. Infiltrating cribriform carcinoma of the breast. A clinico-pathologic and immunohistochemical study of 5 cases. Eur J Gynaecol Oncol. 1996; 17: 228- 231. 3Venable JG, Schwartz AM, Silverberg SG. Infiltrating cribriform carcinoma of the breast: a distinctive clinicopathologic entity. Hum Pathol. 1990; 21: 333- 338. 4Zhang W, Zhang T, Lin Z, et al. Invasive cribriform carcinoma in a Chinese population: comparison with low-grade invasive ductal carcinoma-not otherwise specified. Int J Clin Exp Pathol. 2013; 6: 445- 457. 5 WHO Classification of Tumors Editorial Board e. WHO classification of tumors. 5th ed. Breast Tumors. International Agency for Research on Cancer; 2019. 6Cserni G. Histological type and typing of breast carcinomas and the WHO classification changes over time. Pathologica. 2020; 112: 25- 41. 7Law YM, Quek ST, Tan PH, Wong SL. Adenoid cystic carcinoma of the breast. Singapore Med J. 2009; 50(1): e8- 11. 8Rosen PP, Oberman HA. Invasive carcinoma. In: Tumors of the mammary gland. (Atlas of tumor pathology, 3rd series, fascicle 7) Armed Forces Institute of Pathology. 1993; 157- 257. 9Lee YJ, Choi BB, Suh KS. Invasive cribriform carcinoma of the breast: mammographic, sonographic, MRI, and 18 F-FDG PET-CT features. Acta Radiol. 2015; 56: 644- 651. 10Liu XY, Jiang YZ, Liu YR, Zuo WJ, Shao ZM. Clinicopathological characteristics and survival outcomes of invasive cribriform carcinoma of breast: a SEER population-based study. Medicine (Baltimore). 2015; 94:e1309. 11Colleoni M, Russo L, Dellapasgua S. Adjuvant therapies for special types of breast cancer. Breast. 2011; 20: 153- 157. 12Zhang W, Lin Z, Zhang T, Liu F, Niu Y. A pure invasive cribriform carcinoma of the breast with bone metastasis if untreated for thirteen years: a case report and literature review. World J Surg Oncol. 2012; 10: 251. doi:10.1186/1477-7819-10-251
Comments (0)