
記住我




Osteomyelitis is commonly known as inflammation of bone tissue caused by infection. This can occur either hematogenous route (bacteremia, sepsis) or direct contact (trauma, surgery).1 This condition can present suddenly, slow/mild onset or chronically, depending on the source of the infection. Symptoms ranges from fever, bone pain on the affected area, edema with hyperemia of the affected area, warmth, to difficulty bearing weight or movement on the affected bone.
Reiter's syndrome, on the other hand, is a form of arthritis that is triggered by an infection in another part of the body.2 It also presents with joint pain, swelling, redness, and similar symptoms with osteomyelitis. What sets these two diseases apart is that the latter presents with clinical symptoms such as conjunctivitis, sores in the soft palate, urinary tract infection, and in some cases, body rashes. It is very uncommon to see a patient presenting with Reiter's syndrome with an underlying diagnosis of osteomyelitis. Here, we present such case.
2 CASE PRESENTATIONA 16-year-old boy was brought to the hospital by his mother with complaints of fever, fatigue, abdominal pain, and anorexia in the last 5 months. Patient's mother assumed that he had stomach bug and administered 400 mg of flagyl (metronidazole) tablet and tylenol which relieved the symptoms. Three months after the first episode, abdominal pain returns, but this time it is accompanied with conjunctivitis, urethritis, left knee, ankle and pain on 2nd and 3rd toes, fever (104°F), anorexia, and fatigue. Patient was unable to bear weight on the left leg, which prompted his mother to seek medical attention.
Patient has no prior medical history of osteomyelitis or chronic health condition. His vaccination was up to date. He is not sexually active and is not on any prescription for medication except multivitamins. There is no family history of chronic illness. BMI is 22 kg/m2. He was admitted having had a slight cut on his left thigh while playing soccer in school which was cleansed with sterile solution and treated by the school nurse 6 months prior.
On clinical examination, he had edema, erythema, and tenderness of his left knee and left 2nd & 3rd metatarsal joints which felt warm to touch. He was unable to bear weight at all on his left leg. The right leg appeared normal. On palpation of the abdomen, there was tenderness on the suprapubic region. Further examination revealed bilateral conjunctivitis with clear watery discharge and crust. Temperature was 102°F, tachypnea at 20 breath per minute (BPM), and tachycardia at 110 beats per minute (bpm). Blood pressure was normal at 115/72 mmHg. Patient appeared toxic and fatigued.
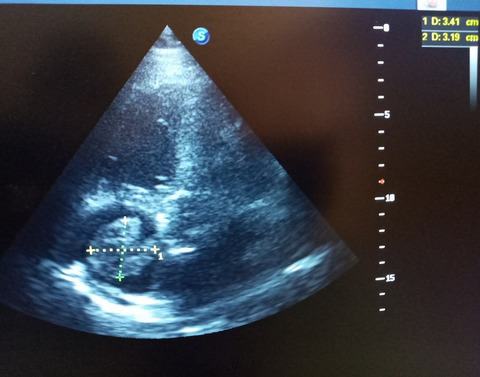
Clinical investigations were started. Urinalysis, blood culture, complete blood count, Widal test, serology for gonorrhea and chlamydia, and arthrocentesis were ordered. MRI of the left leg was also done. Nucleic acid amplification test (NAAT) was negative for gonorrhea and chlamydia. Widal test was also negative for typhoid fever. Urinalysis revealed leukocytosis and no bacteriuria. However, arthrocentesis analysis was positive for staph. Aureus infection and leukocytosis. MRI revealed osteomyelitis of left knee (Figure 1). There was also evidence of soft tissue swelling on the scan (Figure 2). A final diagnosis of osteomyelitis of the left knee was made. It was obvious that the bone infection was what triggered the Reiter's syndrome in our patient.

MRI scan of the sagittal section of left knee with the blue arrow depicting bone deformation indicative of osteomyelitis. This was taken on day 1 of hospital admission. There are evidence of soft tissue swelling as we can see on the scan. Significant joint effusion is seen in the supra patellar recess and joint space

MRI scan of the anterior surface of left knee showing soft tissue reaction (blue arrow heads) and presence of copious fluid collection medial to the iliotibial band within muscles (red arrow head)
Treatment for osteomyelitis was initiated immediately with antibiotics (IV 500 mg vancomycin) every 6 h at 10 mg/min on days 1 and 2. On Day 3, it was switched to oral 1 g BID for 4 weeks upon discharge from hospital. Oral Bactrim (two tablets BID) was administered and was also to be continued for 5 days after discharge. Patient's overall health condition was stabilized on Day 3 of in-hospital treatment, and he was discharged home on the third day with a planned follow-up visit with his primary care physician. Six months after hospital discharge, patient's bone scans and laboratory workups showed complete resolution of all symptoms, and since he had returned to his regular activities and school.
3 DISCUSSIONThere are few other disease conditions that have similar clinical presentations with osteomyelitis. They are gout arthritis, disseminated gonococcal arthritis, and Ewing sarcoma (EWS). The disease conditions can be seen in patients of similar age group as our patient. Reiter's syndrome can be triggered any infection especially bacteria, and on few occasion viruses.3 It can also be seen in patients with gout, and EWS and so this syndrome could mask any inflammatory condition resulting in misdiagnosis of serious diseases. EWS and gout affect the knee with similar clinical symptoms. Knee pain in gout arthritis is caused by accumulation of uric acid crystals in the knee joints which can be detected by special staining of needle aspirate from synovial fluid.4 These crystals (negative birefringent) were absent in our patient which ruled out gouty arthritis. EWS on radiography, often have features such as a wide transition zone, a Codman triangle, and periosteal reaction resembling onion skinning.5 These were not evident on our patient's MRI scan, which again rules out EWS. More so, African Americans are more likely to have osteomyelitis, compared with white population who are more likely to have EWS. According to the results of multiple regression analysis based on ethnicity, African Americans are more likely to have osteomyelitis, while Whites are more likely to develop Ewing sarcoma. On few occasions, EWS has been misdiagnosed as osteomyelitis, which presented with similar features on MRI as osteomyelitis.6 Other than ethnicity, EWS and septic arthritis can present with same clinical features. In some cases, even biopsy finding can be inconclusive in diagnosing EWS.7 Unfortunately, there is no definitive radiologic diagnostic feature of EWS, thus prompting the need for invasive diagnostic testing such as open and percutaneous biopsies in children with diagnosis of osteomyelitis.
Gonococcal arthritis is grouped under septic arthritis and can be diagnosed with NAAT of synovial fluid. This was negative in our patient who never had any sexual activities prior to symptom onset, ruling out septic arthritis due to STIs.
In conclusion, reactive arthritis (Reiter's syndrome) should not be diagnosed as a disease condition, but rather, as a forerunner of a more serious health condition. Our patient's osteomyelitis could be due to the injury he acquired 6 months prior, which was not adequately treated, and was masked with classical Reiter's syndrome. So, it is very important that clinicians should endeavor to screen patients who presents with this syndrome of other underlying diseases.
ACKNOWLEDGEMENTSI would like to thank all the staffs at the department of pediatric and adolescent medicine, who assisted in the care of my patient.
CONFLICT OF INTERESTThe author has no conflict of interest.
AUTHOR CONTRIBUTIONSThe author confirms sole responsibility for the manuscript preparation, referencing, and submission processes.
ETHICAL APPROVALI confirm that the present study confirms ethical standards and guidelines of the journal.
CONSENTWritten informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
The data that support the findings of this study are openly available.
REFERENCES
1 Mayo clinic. 2020. Osteomyelitis. Mayo clinic: https://www.mayoclinic.org/diseases-conditions/osteomyelitis/symptoms-causes/syc-20375913 2Barth WF, Segal K. Reactive arthritis (Reiter's Syndrome). Am Fam Physician. 1999: 60(2): 499- 503. 3Wu IB, Schwartz RA. Reiter's syndrome: the classic triad. J Am Acad Dermatol. 2008; 59(1): 113- 121. 4Morris H, Grant K, Khanna G, White AJ. Gout in a 15-year-old boy with juvenile idiopathic arthritis: a case study. Pediatr Rheumatol. 2014; 12(1): 12– 1. 5McCarville MB, Chen JY, Coleman JL, et al. Distinguishing osteomyelitis from Ewing sarcoma on radiography and MRI. AJR Am J Roentgenol. 2015; 205(3): 640- 651. 6Jordanov MI, Block JJ, Gonzalez AL, Green NE. Transarticular spread of Ewing sarcoma mimicking septic arthritis. Pediatr Radiol. 2009; 39(4): 381- 384. 7Murphey MD, Senchak LT, Mambalam PK, Logie CI, Klassen-Fischer MK, Kransdorf MJ. From the Radiologic Pathology Archives: Ewing Sarcoma Family of Tumors: Radiologic-Pathologic Correlation. RadioGraphics. 2013; 33(3): 803– 831. doi:10.1148/rg.333135005
留言 (0)