Endoscopic retrograde cholangiopancreatography (ERCP) is a well-established modality for diagnostic and therapeutic maneuvers in various pancreaticobiliary disorders, with a success rate of over 95% in patients with normal anatomy. However, patients with surgically altered anatomy who require ERCP pose unique challenges. These include identifying and accessing the afferent limb, maneuvering around acutely angled anastomoses, identifying the papilla or pancreaticobiliary anastomosis, and cannulation of the native papilla or stenotic anastomosis without the benefit of the elevator mechanism. Patients with Billroth II reconstruction may undergo successful ERCP using conventional endoscopes such as side-viewing, forward-viewing, and anterior oblique-viewing. However, in patients with Roux-en-Y reconstruction, access to the papilla or pancreaticobiliary anastomosis can be extremely difficult or impossible, even by using a push enteroscope or pediatric colonoscope. Recently, with the advent of device-assisted enteroscopy (DAE), such as single balloon, double balloon, and spiral enteroscopy, various endoscopic pancreaticobiliary interventions can be performed with a relatively high success rate, even in patients with Roux-en-Y reconstruction.1-5
However, even using DAE, endoscopists are sometimes faced with difficulty identifying the Y anastomosis or afferent limb in patients with Roux-en-Y reconstruction, as if they got lost in a labyrinth. If endoscopists are exhausted because of time consumed in endoscope insertion due to difficulty identifying the Y anastomosis or afferent limb, their fatigue may affect the performance of the ERCP procedures after reaching the papilla or pancreaticobiliary anastomosis.
Several techniques have been reported to advance the endoscope to the correct route at the jejunojejunal anastomosis during balloon endoscopy-assisted ERCP (BE-ERCP).6-9 Yano et al.6 reported a technique to identify the afferent limb by sprinkling indigo carmine into the intestine on the oral side of the Y anastomosis, evaluating the influx of indigo carmine into both limbs at the Y anastomosis, and judging the one with less influx to be the afferent limb, with an accuracy rate of 70.2%. Fukuba et al.7 reported that when reaching the jejunojejunal anastomosis, CO2 enterography was performed after inserting an endoscope into the limb on one side and inflating the balloon to occlude the limb to confirm whether it was an afferent limb, resulting in a significant reduction in scope insertion time (26 vs. 38 min). Tsutsumi et al.8 reported that in patients with Roux-en-Y hepaticojejunostomy who underwent side-to-side jejunostomy if three-pronged lumens could be identified at the anastomosis, the endoscope could be advanced to the central lumen, which is the afferent limb. Iwasaki et al.9 focused on the difference in the direction of peristalsis between the afferent and efferent limb at the Y anastomosis. The finding of intestinal mucosal involvement in the attachment seen in retrograde peristalsis was named the “tidal wave sign”, and the lumen that was positive for this sign was judged to be the afferent limb, with an accuracy rate of 83.9%. However, these techniques, while better than random endoscope insertion, were not perfect.
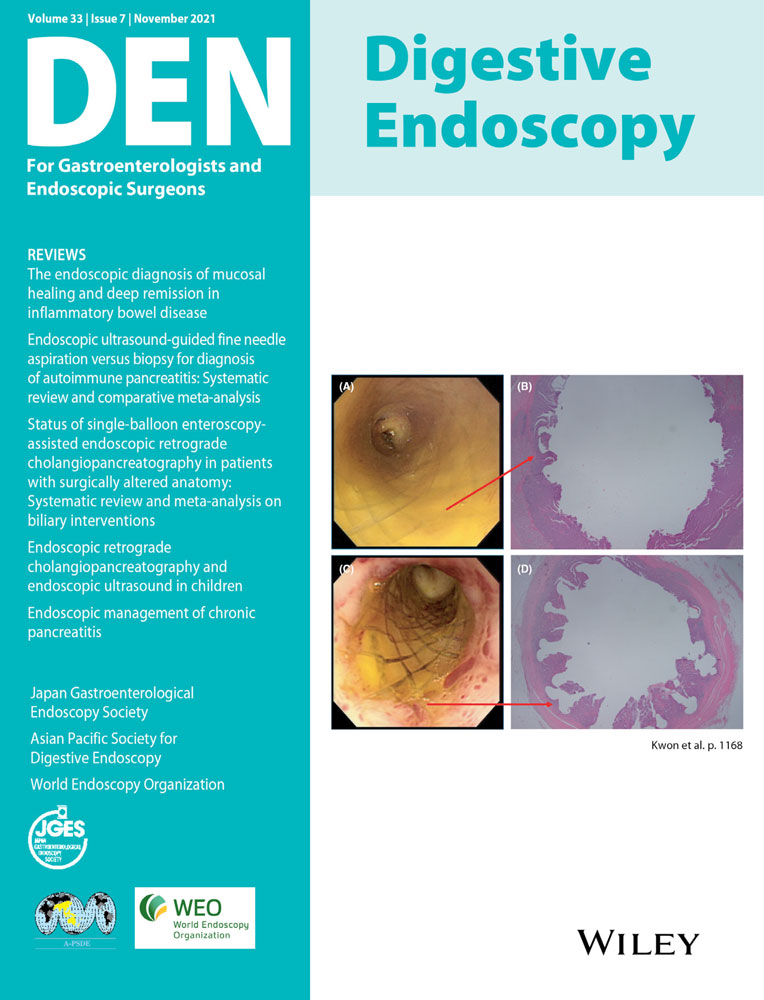
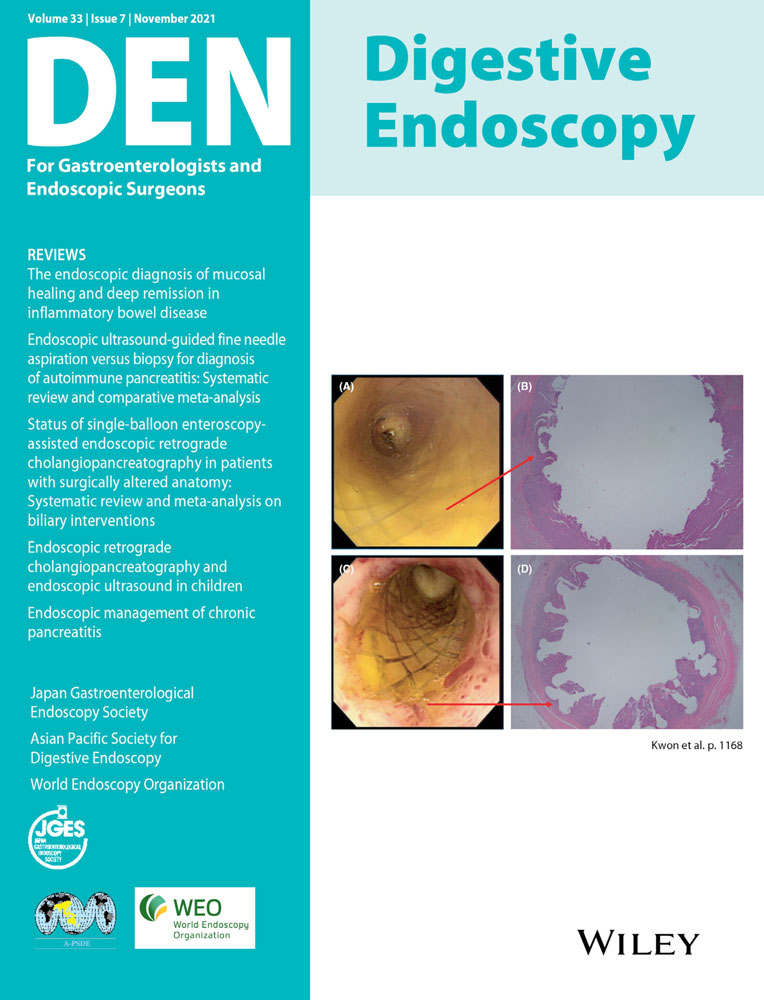
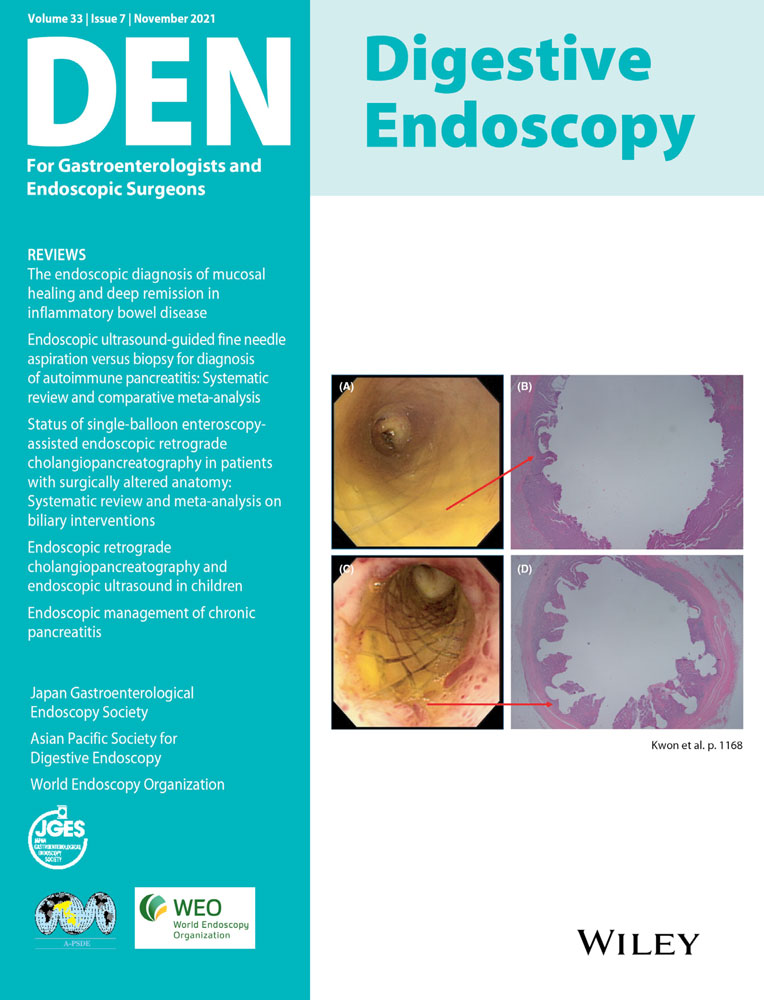
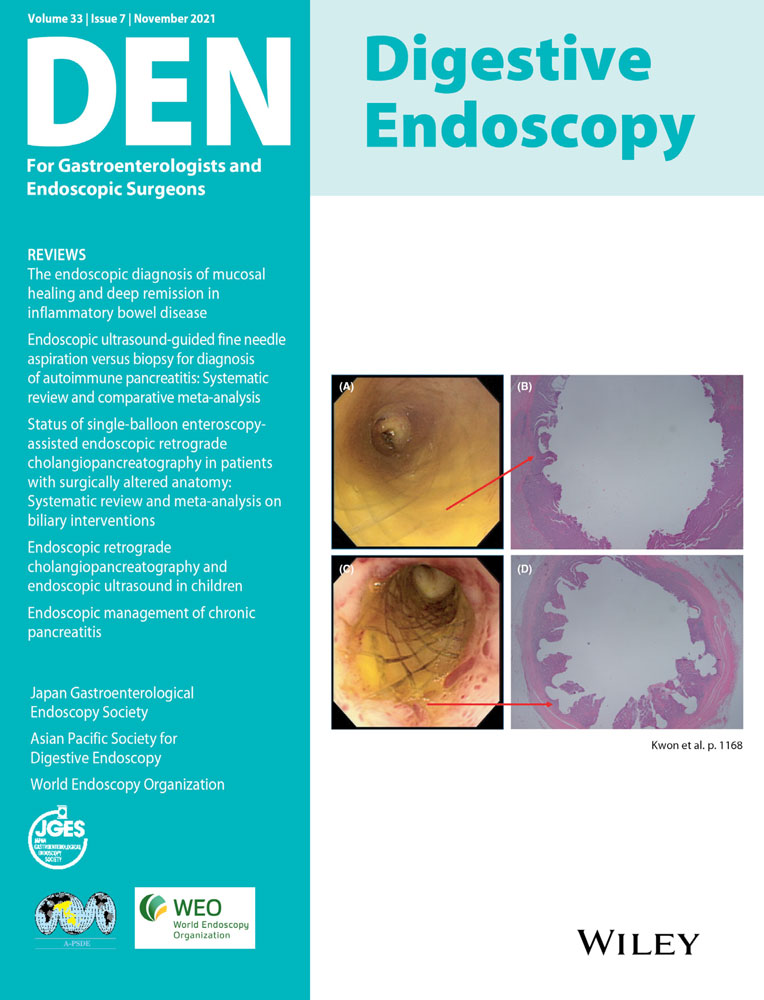
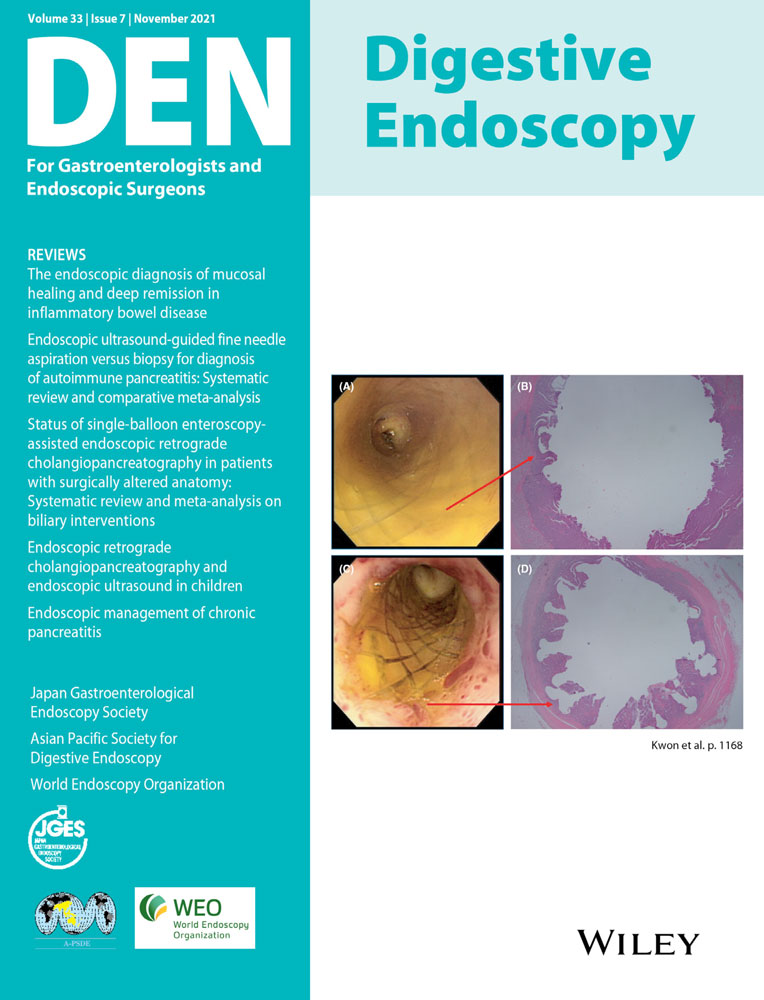
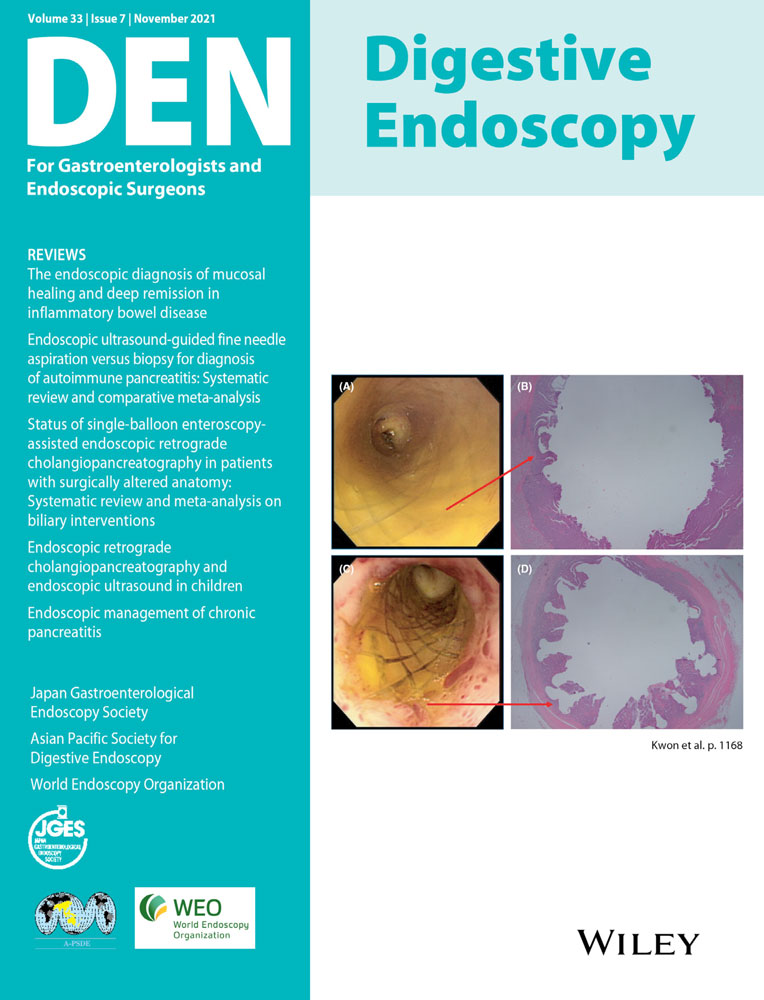
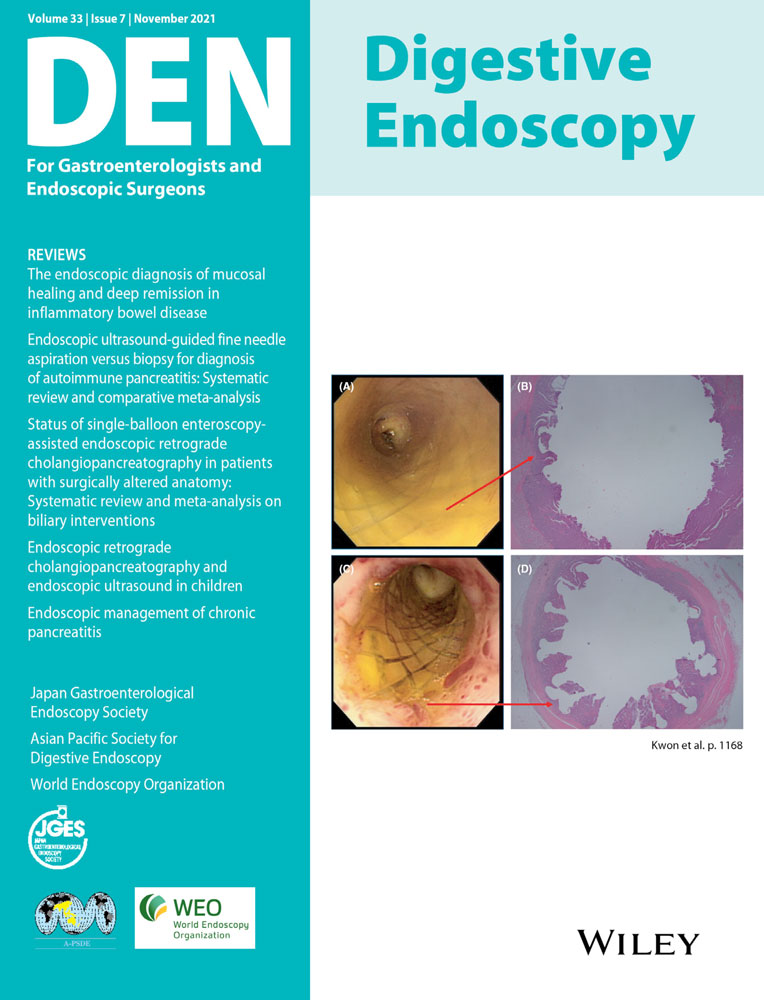
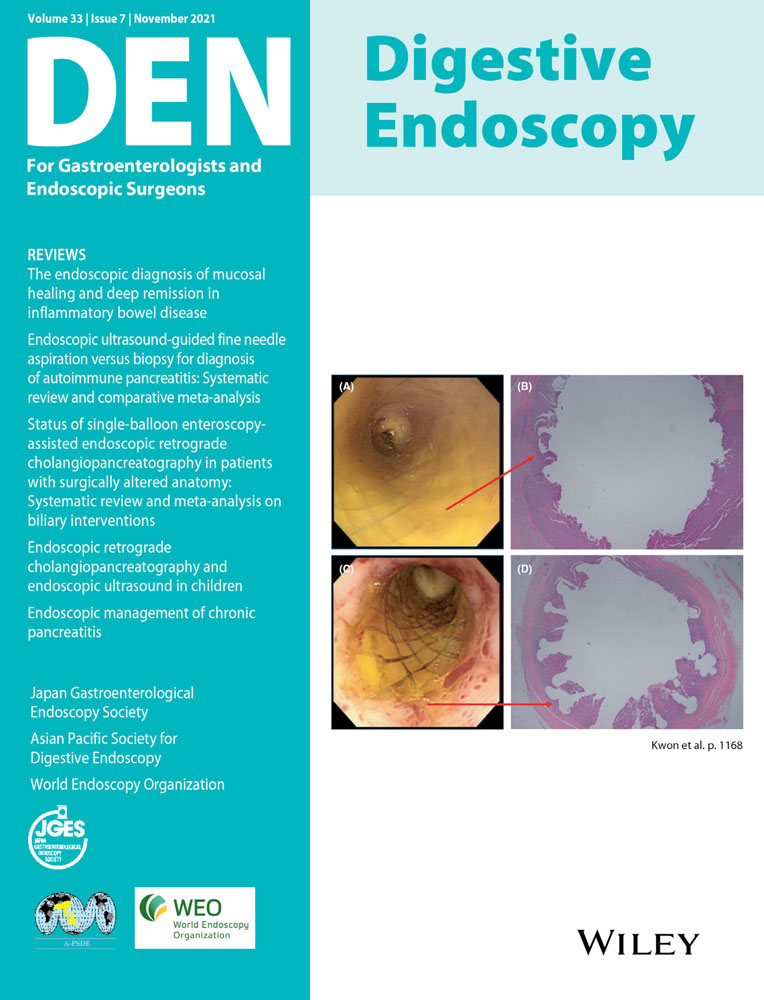
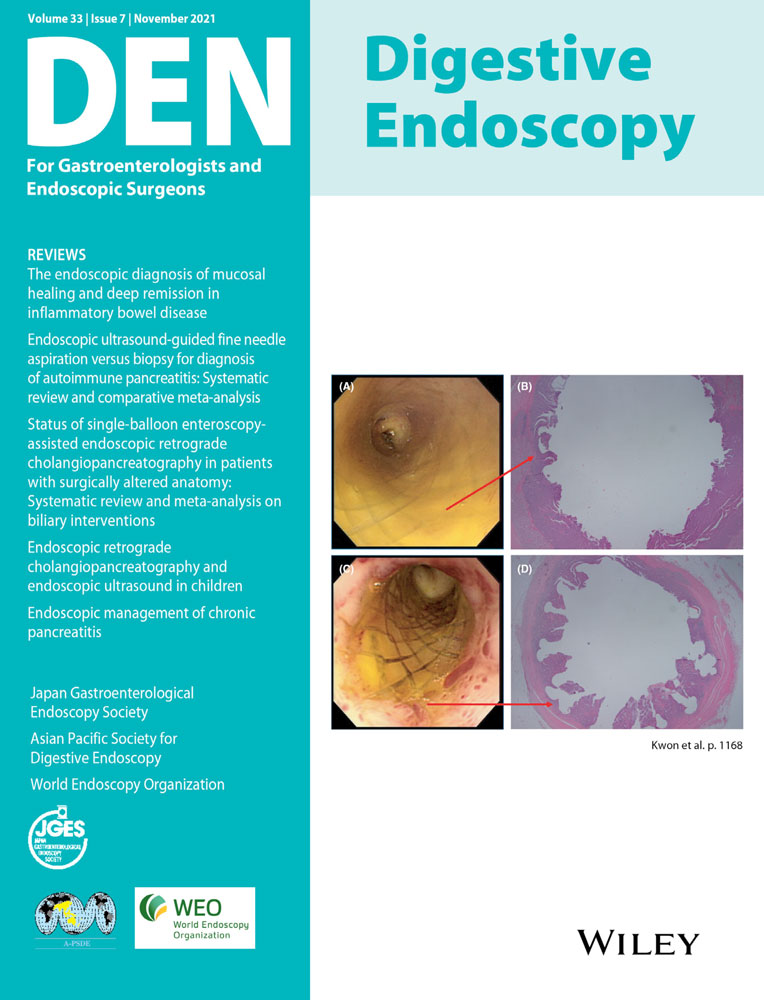
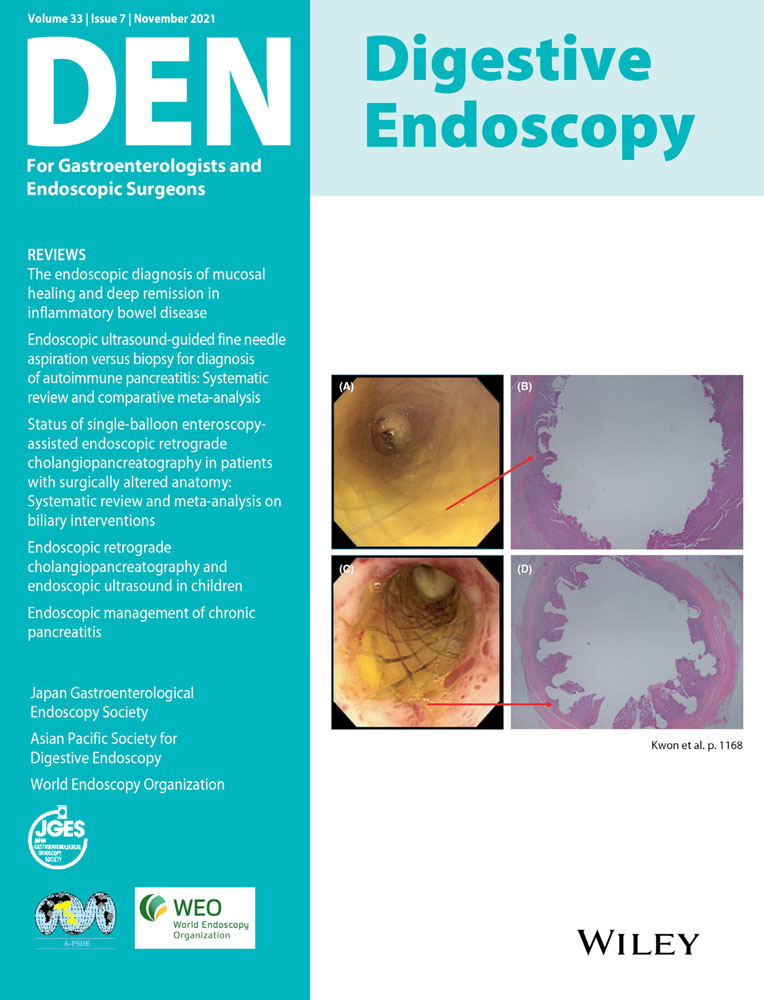
In this issue of Digestive Endoscopy, Kanno et al. conducted a prospective study to evaluate the accuracy of the “fold disruption” sign to identify the afferent limb in patients who had undergone Roux-en-Y gastrectomy.10 In patients with Roux-en-Y gastrectomy, the cut jejunum is elevated and anastomosed to the remnant stomach or esophagus. Since the afferent limb formed by the duodenum and subsequent jejunum is anastomosed to the slit of the elevated jejunum, the transverse folds are disrupted at the slit site. Meanwhile, the opposite wall continues from the oral jejunum to the efferent limb. They named this distinguishable finding the “fold disruption” (FD) sign.
In this study, 30 patients with Roux-en-Y gastrectomy who underwent BE-ERCP were enrolled, of which 29 patients could be observed for Y anastomosis, and FD sign could be evaluated. In the one remaining patient, the scope was inserted into the target lumen without recognizing the Y anastomosis. Of the 29 patients in whom the FD sign could be assessed, one could not reach the target lumen because of severe intestinal adhesion. Still, the scope was inserted into the target lumen in all 28 remaining patients, and the accuracy of the FD sign was 100%.
The FD sign can be applied to both end-to-side and side-to-side manners of anastomosing the afferent limb to the elevated jejunum in cases after Roux-en-Y gastrectomy. However, the limitation is that it cannot be applied in other cases of Roux-en-Y reconstruction such as Roux-en-Y choledochojejunostomy.
The greatest advantage of the FD sign is that it can identify the afferent limb with theoretically 100% accuracy as long as the Y anastomosis is recognized. Additionally, unlike other methods, the FD sign can be judged only by endoscopic observation without any time and effort.
In conclusion, the FD sign must serve as a light for endoscopists to get out of the labyrinth when performing DAE-ERCP in patients with Roux-en-Y gastrectomy.
Author Y.N. is an Associate Editor of Digestive Endoscopy. The other authors declare no conflict of interest for this article.

Comments (0)