
Remember me
Insulin is a protein hormone that promotes glucose uptake from the blood into liver, fat, and skeletal muscle cells.[1] Structurally, it consists of two polypeptide chains (A and B) that are formed through cleavage of a single chain and linked together by two disulfide bonds (with an additional disulfide bond within the A chain;[2]). Insulin is produced in pancreatic beta cells, where it is packaged into secretory granules that accumulate in the cytoplasm close to the plasma membrane. When beta cells are appropriately stimulated, insulin is secreted by exocytosis into islet capillary blood prior to systemic transport through the circulation.[3] Once insulin reaches target cells, it binds to cognate receptors which belonging to the receptor tyrosine kinase family. Insulin receptor isoforms (IR-A or IR-B) are differentially expressed on the surface of a range of cell types and act to regulate its physiological functions.[4] Despite its importance for global insulin signaling, the factors that control the molecular dynamics of insulin in the circulation, following its release from beta cells, are poorly understood.
1.1 Insulin is stored in a Zn2+-bound hexameric form prior to pancreatic secretionThe insulin secretory granules in pancreatic beta cells accumulate high concentrations of ionic zinc (Zn2+; ca. 20 mM;[5]) through the action of the ZnT8 zinc transporter.[6] Insulin readily binds Zn2+ in a manner that leads to the formation of Zn2+-insulin hexamers (Zn2Insulin6; Figure 1) that precipitate with further Zn2+ in a microcrystalline form inside the secretory granules.[7] Formation of hexamers and crystallization are thought to suppress insulin degradation and fibrillation during storage in the pancreas.[8] In these complexes, the two Zn2+ ions are each bound to three His-B10 residues from separate insulin molecules.[9] The Kd of the monomeric 1:1 Zn–insulin complex is 400 nM.[10] However, the affinity for Zn2+ to insulin in the hexameric complex is much higher. Using a competitive ITC approach (using EDTA; ethylenediaminetetraacetic acid), the Kd values of the first and second Zn2+ sites were calculated to be ∼50 and∼500 pM, respectively.[8] Depending on the presence of allosteric effectors, insulin molecules within the hexamer adopt one of two conformations: T (tense), with its B1−9 residues in an elongated conformation, or R (relaxed), with its B1−9 residues in an α-helix, which exposes a hydrophobic phenol-binding pocket. Three different forms of the hexamer are stabilized by coordinating anions (e.g., Cl−) and phenols: T6 (Zn2+), T3R3 (Zn2+, Cl−), and R6 (Zn2+, Cl−, phenol).
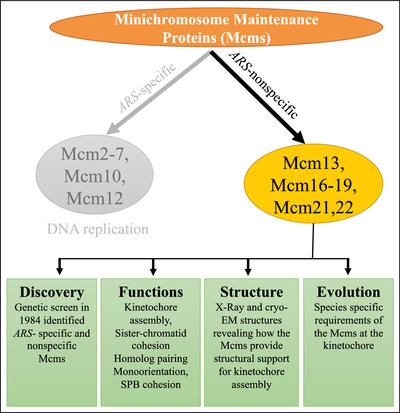
 Insulin decomplexation and the proposed role of HSA. Under normal conditions the HSA protein effectively binds Zn2+ at site A and aids insulin hexamer decomplexation. In the presence of elevated NEFA levels, binding of the NEFA molecule at site FA2 causes a structural change in the HSA molecule whereby His67 moves ∼7–8 Å from His247 and Asp249 ligands dramatically reducing the affinity for Zn2+ inhibiting insulin decomplexation. The following PDB structures are represented: R6-insulin hexamer and monomer, PDB: 1AIY[78]; HSA-Zn2+ complex, PDB: 5IJF [40]; HSA-palmitate complex, PDB: 1E7H [42]
Insulin decomplexation and the proposed role of HSA. Under normal conditions the HSA protein effectively binds Zn2+ at site A and aids insulin hexamer decomplexation. In the presence of elevated NEFA levels, binding of the NEFA molecule at site FA2 causes a structural change in the HSA molecule whereby His67 moves ∼7–8 Å from His247 and Asp249 ligands dramatically reducing the affinity for Zn2+ inhibiting insulin decomplexation. The following PDB structures are represented: R6-insulin hexamer and monomer, PDB: 1AIY[78]; HSA-Zn2+ complex, PDB: 5IJF [40]; HSA-palmitate complex, PDB: 1E7H [42]
Exocytotic insulin release is regulated by a complex of three SNARE proteins (SNAP25, syntaxin and synaptobrevin; [11]), which promote plasma and vesicle membrane fusion to form an ∼1.5 nm ion channel-like fusion pore. This pore connects the secretory granules with the extracellular space, enabling release of vesicular content.[12, 13] Insulin secretion is mediated through expansion of the lipidic fusion pore to up to 12 nm.[14] Structures of T6 and R6 insulin hexamers reveal these complexes to be ∼5 nm in diameter, easily transportable through the fully open lipidic fusion pore. Dissolution of the crystals, breakdown of the hexamers to dimers and then monomers, and the subsequent transport of the monomers to the liver and other tissues occurs via the bloodstream.
1.2 Pharmacological preparations of insulins used to treat diabetes often contain zincClinical insulin preparations are classified as rapid-acting, short-acting, intermediate-acting, or long-acting according to their varying pharmacodynamic profiles. Rapid- and short-acting insulin helps reduce blood glucose levels before mealtimes, while intermediate or long-acting insulin serve the body's general needs, with effects often lasting for a day, or even longer.[15] Most clinical insulins are administered in hexameric forms in formulations that contain zinc. One such form, termed “regular insulin” is a short-acting human insulin, consisting of zinc-insulin crystals dissolved in a clear solution. Following subcutaneous administration, regular insulin dissociates into dimers then monomers. Insulin hexamers must dissociate to monomer units to pass across the capillary endothelium. For this reason, regular insulin typically exhibits a lag phase of approximately 30 min before it appears in the circulation.[16] This time window limits its effectiveness and duration of action for control of postprandial glucose in some individuals. Biosynthetic human insulins and their analogues, introduced in the late 1980s, have revolutionized treatment of diabetes. These recombinant analogues, many of which contain additional Zn2+ in their pharmaceutical formulations, are also characterized by subtle structural deviations altering the pharmacodynamic and pharmacokinetic properties of the molecule after injection.[17] These structural modifications are often targeted at the C-terminus of insulin's B-chain (residues B26-B30), as this region is not critical for insulin receptor recognition.[18] Rapid-acting analogues, such as insulin lispro and insulin aspart, are bioengineered in such a way as to enhance the rate of monomer formation, thereby enabling more rapid absorption into the bloodstream and faster turnover of the insulin effect.[19] Conversely, one example of a long-acting (basal) analogue is insulin glargine, where an amino acid substitution and two arginine additions to the carboxy terminus shift the isoelectric point of insulin (pI 5.4) towards physiological pH, reducing its solubility in tissues.[20] Following subcutaneous injection, the rise in pH (ca. 7.4) causes the acidic glargine to precipitate out of solution generating aggregates of hexameric insulin. As a result, insulin glargine offers prolonged durations of action, more predictable glycemic control and fewer incidences of nocturnal hypoglycemia—the most common side effect of insulin therapy.[21, 22] Another long-acting insulin, insulin detemir, possesses a fatty acid moiety conjugated to the C-terminal end of the B-chain. It binds to serum albumin via the fatty acid chain, thereby providing slow absorption and a prolonged metabolic effect.[23]
1.3 Insulin hexamers dissociate into monomers after pancreatic secretionInsulin hexamers, whether made up of endogenous or pharmacological insulins, are unable to activate insulin receptors,[24, 25] as most of the receptor binding region is masked within the complex.[26, 27] Receptor binding is not only of importance for insulin actions in a range of cells and tissues, but also for clearance of insulin from the bloodstream by the liver.[28] Thus, both activation and clearance of insulin requires the dissociation of the Zn2Insulin6 complex. This dissociation occurs in multiple steps and is thought to begin with the release of one Zn2+ ion. This then leads to the release of two insulin molecules (as a dimer) from the hexamer to form a tetramer. Release of a second Zn2+ ion then leads to breakdown of the tetramer to form two further dimers.[8] The dissociation process in vivo is quite fast; it has been demonstrated that insulin is detectable as a monomer within a few seconds of entering the portal vein, although the proportion of total secreted insulin this represents is not known.[29] For endogenous insulin, it is likely that there is an optimal rate of dissociation of insulin from the hexamer that allows effective local autocrine/paracrine signaling within the pancreas as well as endocrine signaling to distal cells located at other sites in the body.
Zn2+-insulin complex formation—and dissociation of this complex—is an equilibrium process; it is hence clear that concentrations of both Zn2+ and insulin affect the proportion of hexamer vs. monomer.[30] At pH 7.3, it is well-established that Zn2+ coordination stabilizes the hexamer, thus secretion of insulin into an (extracellular) environment where available Zn2+ is markedly reduced has been proposed as a mechanism to facilitate Zn2+-insulin hexamer breakdown.[31] Therefore, the available Zn2+ concentration in plasma influences insulin dissociation.[32] When insulin is secreted, a “puff” of free Zn2+ is also released that will increase temporo-spatial Zn2+ availability.[33] A similar phenomenon is likely to occur when clinical insulins are injected as part of a Zn2+-containing formulation. At sites of release (or injection), it is thus possible that a significant fraction of insulin does not immediately dissociate into monomers and that some exchange of Zn2+ with other molecules is required to facilitate adequate hexamer dissociation. It has recently been proposed that serum albumin, the most abundant protein and primary carrier of Zn2+ in plasma and other extracellular fluids, serves this purpose and may control Zn2+ availability in a manner that acts to control insulin pharmacodynamics.[34]
1.4 Control of circulatory zinc dynamics by serum albuminFor the topic of this discussion, it is not total plasma zinc that is of interest, but only the “exchangeable pool”, which amounts to 75%–90% of the total.[35] Within this pool, the majority (∼90%) of zinc is bound to human serum albumin (HSA), with the remainder bound to other proteins and small molecules such as histidine.[36, 37] HSA is a 66.5 kDa plasma protein that binds Zn2+ with moderate affinity (Kd at pH 7.4; physiological ionic strength = 3.7 μM; [38]). It consists of three homologous domains (I–III),[39] and tightly regulates the concentration of Zn2+ in plasma at an optimal level by acting as both a chelator and systemic transporter. HSA-Zn2+ complexes have been studied using X-ray crystallography, confirming the major zinc binding site (site A) to be located at the interface between domains I and II. Zn2+-coordination at this site involves His67, His247, Asp249, and a water molecule,[40] and has been shown to engage in considerable interplay with the binding of non-esterified fatty acids (NEFAs) that are also transported by HSA.
NEFAs play critical roles in mammalian energy metabolism. HSA is the major NEFA carrier in human plasma.[41] There are seven medium-to-high affinity NEFA binding sites across the three domains of HSA (termed FA1-7;.[42, 43] When a NEFA molecule occupies site FA2, one of the highest affinity sites on HSA, it allosterically disrupts Zn2+-binding at site A by triggering a movement of His67 (from domain I) by ∼7–8 Å relative to His247 and Asp249 (from domain II; [37, 40]). HSA typically carries 0.1–2 molar equivalents of NEFAs under basal physiological conditions. However, plasma NEFA levels are dynamic and rise following dietary intake, after prolonged fasting, and during periods of intense exercise. Also, chronically elevated NEFA levels are associated with a range of disorders including obesity,[44, 45] type 2 diabetes mellitus (T2DM; [46]), fatty liver disease,[47] and cancer.[48] In obese individuals the plasma concentrations of NEFAs (at rest) are ∼2–3 times higher than controls.[43]
Crucially, the addition of myristate decreases the zinc-binding capacity of both bovine serum albumin (BSA),[49] and HSA.[38] Consequently, in fetal bovine serum or human plasma, addition of myristate decreases the proportion of Zn2+ bound to serum albumins in these fluids,[35] with “liberated” Zn2+ predominantly shifting to other plasma proteins with zinc-binding ability. More recently, we have shown that these NEFA-mediated alterations in human plasma zinc speciation impact on zinc-regulated aspects of hemostasis, and that such alterations are reflected in type 2 diabetic patients.[46] Since insulin is also a protein with zinc-binding ability, we hypothesize that it may be affected by NEFA-induced alterations in zinc speciation as well.
1.5 Hypothesis: Elevated fatty acid concentrations in disease states may influence insulin decomplexation through binding to HSARadioimmunoassays and insulin tolerance tests in rats have confirmed that the presence of serum albumin aids the dissociation of insulin hexamer into active monomer.[34] Zn2+-free or Zn2+-insulin preparations, pre-incubated in the presence and absence of 3% BSA, were administered to rats and the subsequent effect of each on the pharmacokinetic characteristics of insulin was determined. A greater decrease in plasma glucose was observed in the rats treated with either Zn2+-free or the BSA/Zn2+-insulin preparation compared to those treated with the Zn2+-insulin preparation without BSA. This demonstrates that Zn2+-chelation by serum albumin may be important for breakdown of insulin into active subunits after exocytosis—a process not fully understood nor appreciated on a quantitative level, but central to blood glucose control. Interestingly, guinea pigs, a species of rodent that originated in the Andes of South America (where zinc availability is very low), are the only known mammal that do not store insulin bound to Zn2+ [50] Guinea pigs are also the only known mammal whose albumin lacks site A (they possess Ala instead of His at position 67), suggesting that zinc-binding to insulin and albumin is intrinsically linked in mammalian evolution. Given that the ability of HSA to bind Zn2+ is reduced by NEFAs, and that plasma NEFA levels are elevated in disease states, the hypothesis that NEFAs adversely influence insulin decomplexation and pharmacodynamics through reduced HSA-Zn2+ binding (as summarized in Figure 1) is compelling.
1.6 Elevated fatty acids are associated with insulin resistance and altered insulin pharmacodynamicsNumerous studies suggest that high plasma NEFA concentrations may play a significant role in the modulation of IR,[51, 52] although the molecular underpinnings of this dynamic are likely to be highly complex. Several studies in rats and humans showed that an increase in plasma NEFA concentration inhibits insulin activation of insulin receptor substrate-1-associated phosphatidylinositol 3-kinase activity in skeletal muscle and adipose tissue.[52-54] Boden et al. reviewed the mounting evidence of a relationship between NEFAs and IR and concluded that although there has been a vast amount of data illustrating the interplay between elevated NEFAs and IR and beta cell dysfunction, further work is required to decipher the exact molecular mechanisms.[55] They also concluded that elevated NEFAs should represent an important therapeutic target in obesity and T2DM.
T2DM is associated with other co-morbidities such as cardiovascular diseases and obesity, which have a significant impact on both the quality and length of life in people with diabetes. Obesity is associated with elevated plasma total NEFA levels, primarily as a result of increased release from adipocytes. NEFA release from adipocytes is enhanced by their resistance to the antilipolytic effect of insulin and inability of “obese adipocytes” to effectively recycle NEFAs via re-esterification.[56, 57] Both human and animal studies indicate that weight loss and gain correlate closely with increasing and decreasing insulin sensitivity, respectively. It has been shown that weight loss of around 15 kg or bariatric surgery significantly improves insulin sensitivity, resulting in reversal of T2DM.[58-60] It is also established that treatment with pemafibrate, a drug effective in reducing plasma NEFA levels, can lead to improvement in IR in patients with metabolic syndrome.[61] We hypothesize that lowered lipids (due to either weight loss or treatment with NEFA-lowering fibrates) may play a part in improving insulin actions in such individuals by protecting the Zn2+-binding capacity of HSA and thus allowing more favorable physiological (and pharmacological) insulin decomplexation.
Several factors may alter the pharmacokinetic and pharmacodynamic profiles of insulin analogues in patients with T2DM. One example is of course obesity, which as described above, is associated with elevated plasma NEFA levels and increased IR. Obesity has been shown to influence the activity of the rapid-acting insulin analogue aspart, where prescribing information states that clearance, a process that requires insulin receptor binding,[28] is reduced by 28% in patients with a body mass index (BMI) exceeding 32 kg/m2.[62] Insulin dose-response curves generated by administration of exogenous insulin into both lean and non-diabetic obese subjects suggest that lean individuals have faster glucose clearance rates, potentially indicating different pharmacokinetics, when compared with obese individuals.[63] Euglycemic clamp studies have also enabled assessment of the role of adiposity on the pharmacodynamics of long-acting insulins such as glargine and detemir. For example, Porcellati et al. demonstrated that a high BMI is associated with reduced suppression of endogenous glucose clearance in T2DM subjects administered with insulin detemir.[64] In addition, high plasma NEFA concentrations, as are associated with a high BMI, may reduce insulin detemir-HSA binding to some degree through competition for binding sites. Nevertheless, as insulin therapy itself is commonly associated with weight gain,[65] individualized monitoring of T2DM patients is already needed to ensure that this does not undermine the improved glycemic control offered by insulin analogues.
1.7 Establishing the role of NEFAs in insulin decomplexation using fluorescence-based methodsTaken together, the above considerations strongly suggest that there is an urgent need to further understand insulin dynamics in vivo, and in particular, the influence of HSA, and its interaction with NEFAs, on insulin decomplexation. Insulin concentrations in plasma are in the high pM range,[66] whilst the HSA concentration is ∼600 μM.[41] This generates dynamic range and sensitivity issues for investigating their competition for Zn2+ under native conditions experimentally. Insulin decomplexation has been studied using various methods including isothermal titration calorimetry,[8] and electron paramagnetic resonance spectroscopy.[67] However, such approaches are unsuitable to study insulin decomplexation at physiological insulin concentrations due to their low sensitivity. In order to examine insulin complexes at low nM concentrations, fluorescence-based studies are likely to provide the best option. For example, insulins labelled with fluorescein isothiocyanate (FITC), Cy3, Cy5, and related dyes are commercially available and have been used to visualize insulin complexes in cells.[68] Site-specific incorporation of amine-reactive fluorescent molecules into insulin has been mostly achieved through attachment to primary amines A1 (Gly), B1 (Phe) and the ε-amino group of B29 (Lys). The order of reactivity of these amines was found to be B1 > A1 > B29; it has been shown that mono-conjugates of insulin labelled at B1 can be obtained by carefully controlling the labelling conditions,[69] and that B1 conjugates have the same biological activity as native insulin.[70] Thus, examination of Zn2+-induced insulin complexation, and subsequently, HSA-mediated decomplexation using HSA preparations containing different concentrations of NEFAs, should be possible using fluorescent mono-conjugates of insulin if a method can be developed where the fluorescent properties change upon complexation/decomplexation.
Potentially the simplest fluorescence-based approach to investigate insulin (de)complexation will be to use mixtures of insulins labelled with fluorophores that form Förster resonance energy transfer (FRET) pairs. FRET is based on the dipole-dipole interaction between two fluorescent molecules and involves the transfer of excitation energy upon absorption of light from a donor molecule to an acceptor molecule in close proximity.[71] Because the efficiency of energy transfer depends on the inverse of the 6th power of the distance, FRET has been used as a molecular ruler to measure nanometer size distances between 10–80 Å in biomolecules and to study the association of interacting partners in multi-subunit complexes (Figure 2A; [72]). T6 hexameric insulin has a size of around 40 Å which is well within the distance range that can be measured by FRET. For instance, based on crystal structures of T6 human insulin (PDB: 1MSO), the predicted Cα-Cα distance between the B1 residues is 39 Å in the dimer configuration (Figure 2B). Even considering the increase in distance (∼10 Å) due to the linker used to covalently attach the fluorophore, the resulting donor-acceptor distance is within the range of distances accessible by the Cy3/Cy5 and other FRET pairs (i.e., FITC/Cy3). In the case of higher oligomeric states (tetramers and hexamers), an additional shorter distance of (∼12 Å) involving B1 residues from different dimers would also be expected, producing an enhanced FRET signal (relative to that of the dimer) and thus providing a direct measurement of Zn2+-induced complexation and decomplexation by HSA (Figure 2C). It is interesting to note that although the application of FRET methods at single-molecule level (smFRET) during the last decade has revolutionized our understanding of protein-protein interactions,[73] their use in the context of insulin complexation has not been reported. We hypothesize that smFRET (Figure 2D), and other single molecule approaches such as stepwise photobleaching to count fluorescently labelled monomers in each insulin oligomer (Figure 2E; [74]), might offer unique insights into the mechanism of insulin (de-)complexation that are difficult to quantify by other techniques. This includes resolving the equilibrium populations of each oligomeric species, their interconversion dynamics and how these might be altered during HSA-mediated decomplexation (Figure 2D and 2E), with and without NEFA, for native insulin and therapeutic analogues. Importantly, the high sensitivity of smFRET to detect sub-picomolar concentrations of fluorescently labelled species is ideal to evaluate insulin (de-)complexation models in native conditions both in vitro and in vivo. Two important considerations for such experiments are (i) the optimization of insulin and zinc concentrations when forming complexes to prevent (metal-induced) aggregation and fibrillation,[8] and (ii) to evaluate the impact of these fluorescent reporters in the self-assembly properties of labelled insulin compared to label-free insulin using dynamic light scattering, analytical centrifugation or sedimentation profiles. The latter is particularly important because there is little information regarding the impact of fluorescent labelling on the complexation/decomplexation mechanism of insulin. Given that the characterization of HSA-mediated insulin assembly only requires the presence of a single FRET pair per hexamer, any potential impact in this process due to the presence of the dyes should be minimized by using sub-stoichiometric amounts of labelled insulin with respect to unlabeled monomers. In addition, the relatively bulky cyanine dyes (MW ∼1200) can be replaced by smaller molecules such as BODIPY derivatives (MW ∼420) that are also available in FRET-pair combinations. These molecules have a molecular size closer to nitroxide spin labels (MW ∼200) that have been used to investigate the hexameric structure of insulin in a frozen state.[67] Lastly, it might be worth to consider alternative labelling routes based on the covalent attachment of sub-stoichiometric concentrations of donor and acceptor molecules to pre-formed hexameric complexes. Although, to our knowledge, this strategy has not been explored in the context of insulin but has been successfully used to site-specifically incorporate a FRET pair within multimeric structure of membrane proteins.[75]

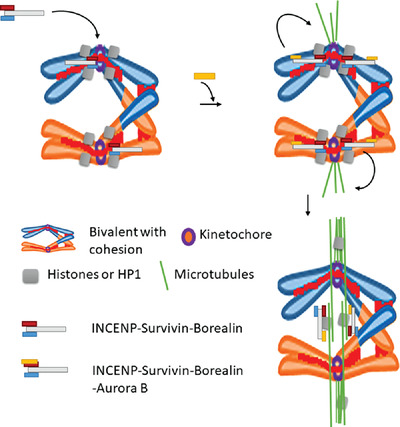
Fluorescence-based strategies to investigate insulin complexation/decomplexation and the proposed role of HSA. (A) Dependence of FRET efficiency with the donor-acceptor distance for the Cy3-Cy5 FRET pair. The Förster distance at which 50% FRET efficiency is obtained (53 Å) is also shown. R0 Red (Cy3, donor), Blue (Cy5, acceptor). (B) Estimated intra-dimer Cα-Cα distance (39 Å) between the two B1 residues (Phe). (C) Estimated inter-dimer Cα-Cα distances between B1 residues in the tetramer and hexamer configurations. Donor (Cy3) and acceptor (Cy5) dyes and linkers attached to B1 residues are shown only for displaying purpose and not drawn to scale. (D) Schematics of FRET measurements at the single molecule level. FRET labelled insulin hexamers are immobilized on the quartz slide using biotin-streptavidin interactions. The Cy3 (red) and Cy5 (blue) intensities and the FRET efficiency (gray) of each spatially separated hexamer is individually collected for each molecule thus providing access to changes in the distribution of distances in the presence of Zn2+ and upon addition of HSA. To avoid non-specific binding of insulin the microscope slide is passivated with a polyenthyleneglycol (PEG) layer where ∼1% of PEG carries a biotin group (green). (E) Schematics of single-molecule stepwise photobleaching methods to determine insulin stoichiometry. Briefly, insulin molecules are immobilized using biotin-streptavidin and continuous laser irradiation leads to dye photobleaching in a single and irreversible step. The number of photobleaching steps observed in each immobilized molecule allows the number of monomers in each insulin molecule to be quantified and thus the equilibrium distribution from monomers to hexamers upon injection of Zn2+ or HSA
In addition to direct monitoring of (de-)complexation, the influence NEFA-free and NEFA-loaded HSA on insulin signaling could be examined using suitable in vitro or ex vivo cell culture models. A wide range of cell types, including adipocytes, hepatocytes and endothelial cells, express insulin receptors at their surface and would be suitable for study. Hexameric Zn2+-insulin complexes (which may include clinical insulin formulations) may be added to culture media containing HSA with or without NEFAs and insulin signaling monitored at different time-points. There are multiple well-established assays that can be employed to examine insulin signaling focused on activation of downstream kinases and other enzymes (e.g., AKT serine/threonine kinase 1, endothelial nitric-oxide synthase (eNOS), extracellular signal-regulated kinases 1 and 2, p38 mitogen-activated protein kinase and Jun N-terminal kinase). Recent progress has been made in the development of fluorescent probes for detection and bioimaging of nitric oxide, potentially allowing eNOS signaling to monitored in cells in real time.[76] Luciferase-based assays which monitor insulin-dependent gene expression are also available,[77] and may be employed to measure insulin receptor pathway activation in relevant cell models at different time points.
1.8 Future implications for diabetes managementHere we present a novel and potentially testable hypothesis, namely that elevated plasma NEFAs may contribute to altered insulin decomplexation through modulation of Zn2+-HSA interactions in metabolic disease states. We speculate that this mechanism contributes to IR and the unpredictable dose-response profiles observed for certain insulin-based drugs in some individuals. This mechanism can be targeted through various dietary and pharmacological interventions. Such interventions may include: (1) Altering the saturated/unsaturated NEFA ratio in the diet, as the degree of saturation of the NEFAs appears to influence Zn2+-HSA interactions.[45] (2) The use of fibrate drugs to reduce plasma NEFA levels. (3) Targeting fatty acid synthase to reduce de novo synthesis of NEFAs. (4) Design and administration of a small molecule able to inhibit binding of NEFA molecules specifically at the FA2 site on HSA, yet allowing NEFA transport via other binding sites whilst not impairing Zn2+ binding to site A.
We propose that further investigation of the hypothesis presented here will lead to better understanding of the molecular mechanisms that regulate insulin pharmacodynamics and diabetes management including the potential development of more specific, personalized treatments for diabetes.
ACKNOWLEDGMENTSThe authors thank the Leverhulme Trust (grant no. RPG-2017-214), the Scottish Funding Council (through a St Andrews Restarting Research Fund award) and the Wellcome Trust (through an Institutional Strategic Support Fund award; grant no. 204821/Z/16/Z) for funding.
AUTHOR CONTRIBUTIONSConceptualisation, J. Carlos Penedo, Claudia A. Blindauer and Alan J. Stewart; writing, Swati Arya, Adam J. Gourley, J. Carlos Penedo and Alan J. Stewart; review and editing, all authors.
Comments (0)