
Remember me

Clinical manifestations of coronavirus disease 2019 (COVID-19), caused by the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), range from mild upper respiratory tract symptoms to severe acute respiratory distress syndrome (ARDS). The natural course of recovery from severe COVID-19 pneumonia remains unclear. Many survivors with severe COVID-19 pneumonia show long-term residual abnormalities on chest computed tomography (CT) scans. However, there is little information on whether this condition represents an irreversible disease. Moreover, the histopathological features of lung sequelae post-COVID-19 have not been reported extensively. Thus, increasing recognition of the histopathological characteristics may lead to more appropriate and effective treatment strategies for lung sequelae post-COVID-19.
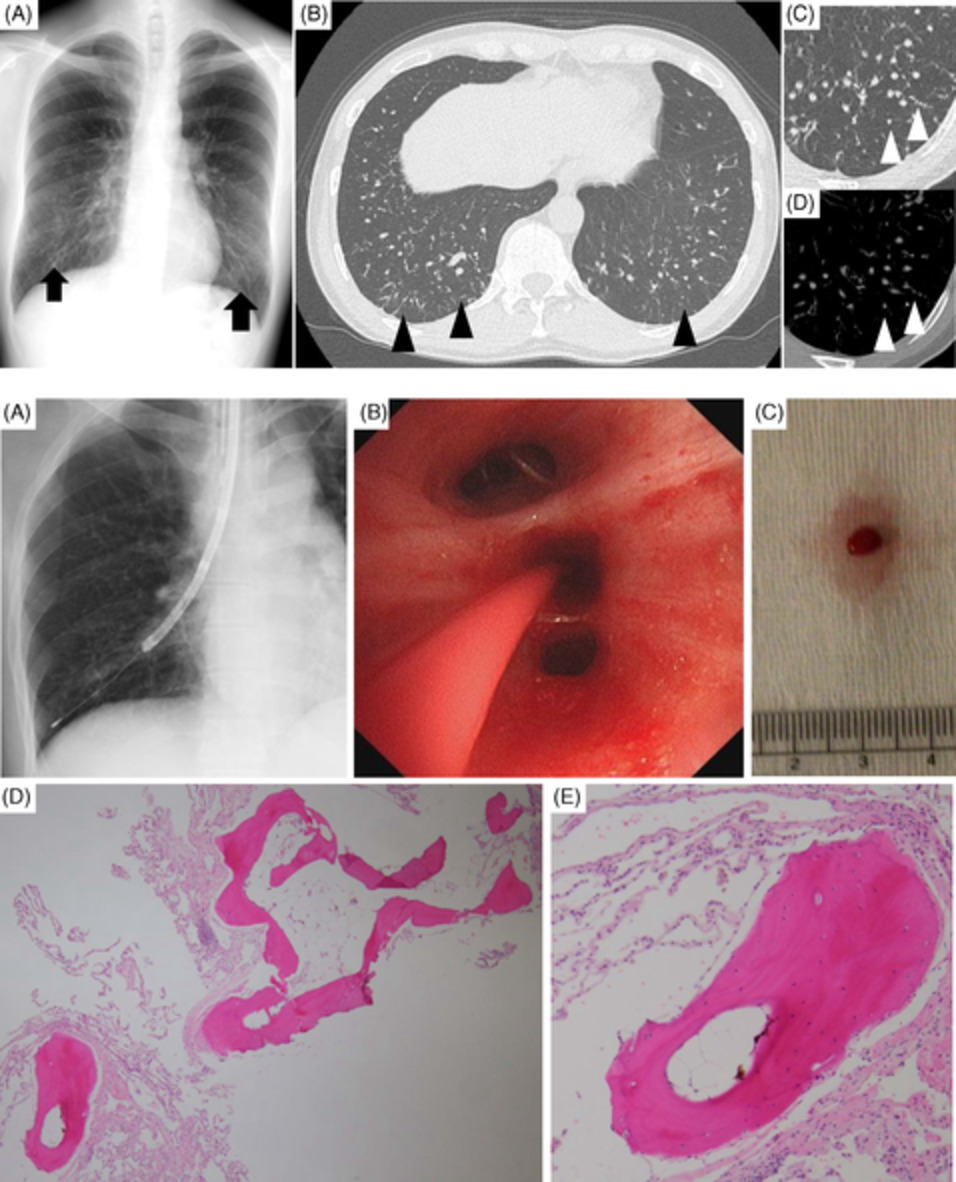
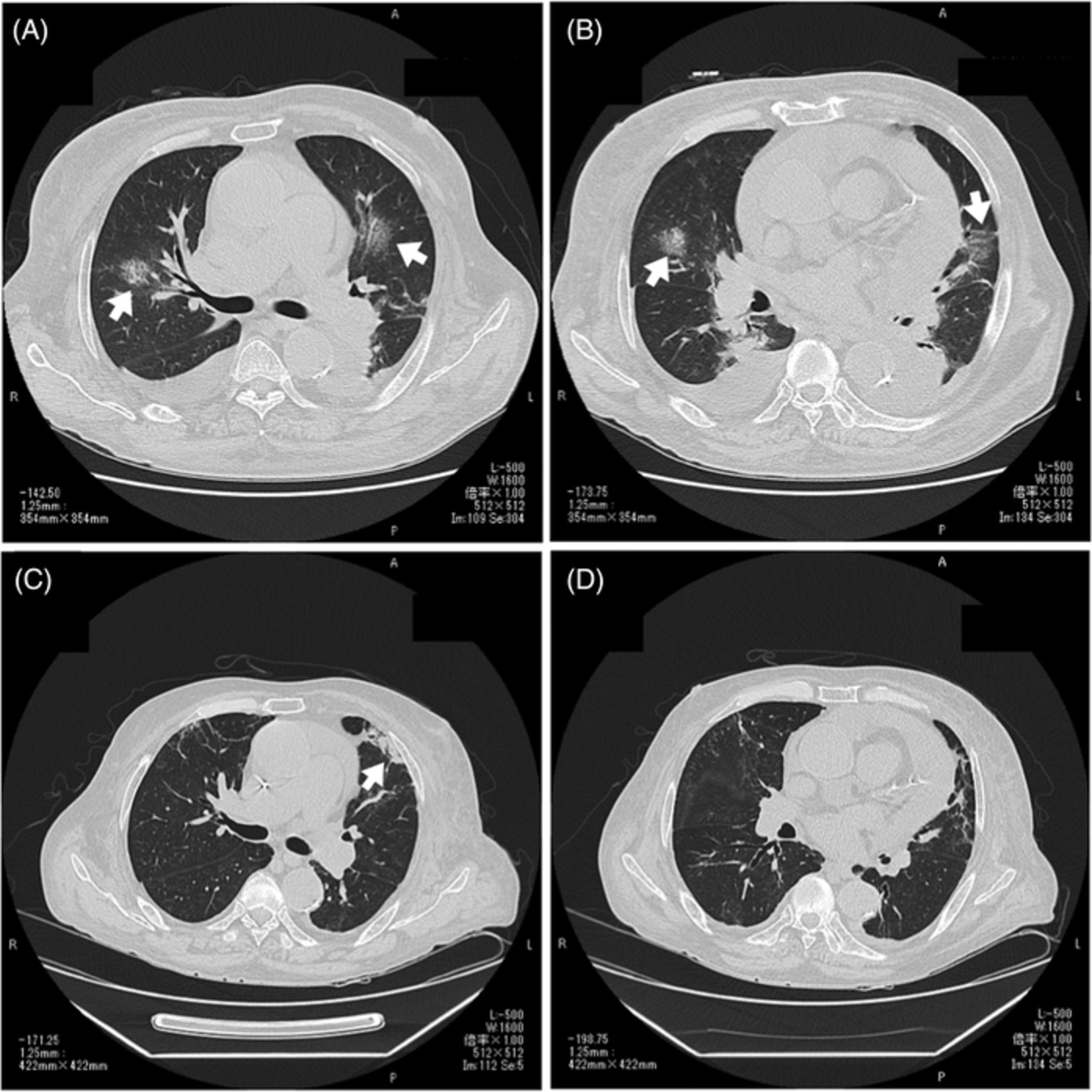
CASE REPORT Case 1A 76-year-old Japanese man with a 30-year history of diabetes mellitus and hypertension and who was obese (body mass index, 32.7 kg/m2) was presented to our hospital for lung sequelae post-COVID-19. At a previous hospital, high-resolution CT (HRCT) of the chest showed peripheral ground-glass opacities (GGOs) with some consolidation predominantly in the left lung (Figure 1A,B). He was treated with methylprednisolone (125 mg/day) intravenously for 3 days, followed by dexamethasone (6.6 mg/day for 5 days), favipiravir (1.8 g twice per day on day 1, followed by 0.8 g twice per day for 2 days), remdesivir (intravenously with a loading dose of 200 mg and a daily maintenance dose of 100 mg for a total of 5 days), camostat mesylate (600 mg/day for 10 days) and tocilizumab (8 mg/kg). However, he continued to have severe hypoxaemia. HRCT imaging revealed peripheral GGOs with interlobular septal thickening predominantly in the left lung, as well as traction bronchiectasis and perilobular bands of consolidation in both lungs (Figure 1C,D). We decided to perform video-assisted thoracoscopic surgery (VATS) in order to determine appropriate future therapy. During VATS, the histopathological findings were consistent with apparent intra-alveolar and mural plugs and alveolitis with a great number of inflammatory cell infiltration. No histopathological features of diffuse alveolar damage (DAD) were evident (Figure 1I,J). SARS-CoV-2 detection using reverse transcription polymerase chain reaction on formalin-fixed paraffin-embedded sections of the lung biopsy resulted negative. Therefore, he was treated with intravenous methylprednisolone (1000 mg/day) for 3 days. Then, we tapered the dosage based on his respiratory condition. We initiated a combination therapy with cyclosporine (150 mg/day) as a calcineurin inhibitor and prednisolone (30 mg/day). During prednisolone tapering, his clinical conditions and radiological findings improved dramatically over the next month (Figure 1E,F). Six months after combination therapy was initiated, chest HRCT showed further improvement (Figure 1G,H). In addition, forced vital capacity (FVC) and diffusing capacity for carbon monoxide (DLCO) increased from 1.65 to 1.8 L, and from 8.33 to 10.73 ml/min/mmHg, respectively. Serum Krebs von den Lungen-6 (KL-6) also decreased from 604 to 184 U/ml. The patient had no relapse or adverse effects in the subsequent 6 months.

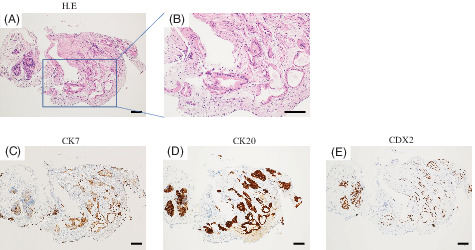
Serial changes in high-resolution computed tomography (HRCT) of the chest in case 1. (A, B) At the previous hospital, HRCT revealed peripheral ground-glass opacities (GGOs) with some consolidation predominantly in the left lung. (C, D) Upon admission, HRCT revealed peripheral GGOs with interlobular septal thickening, predominantly in the left lung, and traction bronchiectasis and perilobular bands of consolidation in both lungs. (E, F) One month after we initiated combination therapy with corticosteroid and calcineurin inhibitors, some interlobular septal thickening and residual GGOs were observed. (G, H) Six months after the start of therapy, chest HRCT showed obvious resolution of the abnormalities. (I) Histopathological findings of lung biopsy specimens obtained by video-assisted thoracoscopic surgery. Low-magnification microscopy showed diffuse and temporally uniform interstitial thickening (Elastica van Gieson stain; bar represents 500 μm). (J) High-magnification microscopy showed apparent intra-alveolar and mural plugs and alveolitis with a great number of inflammatory cell infiltration (haematoxylin–eosin stain; bar represents 100 μm)
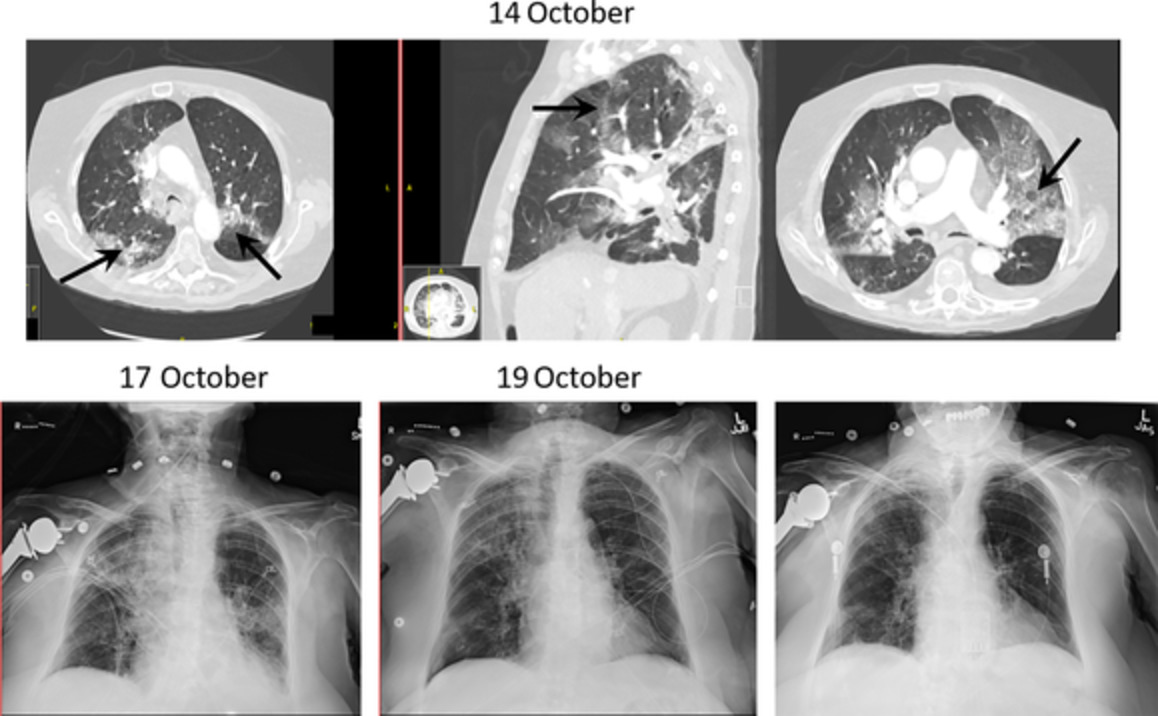
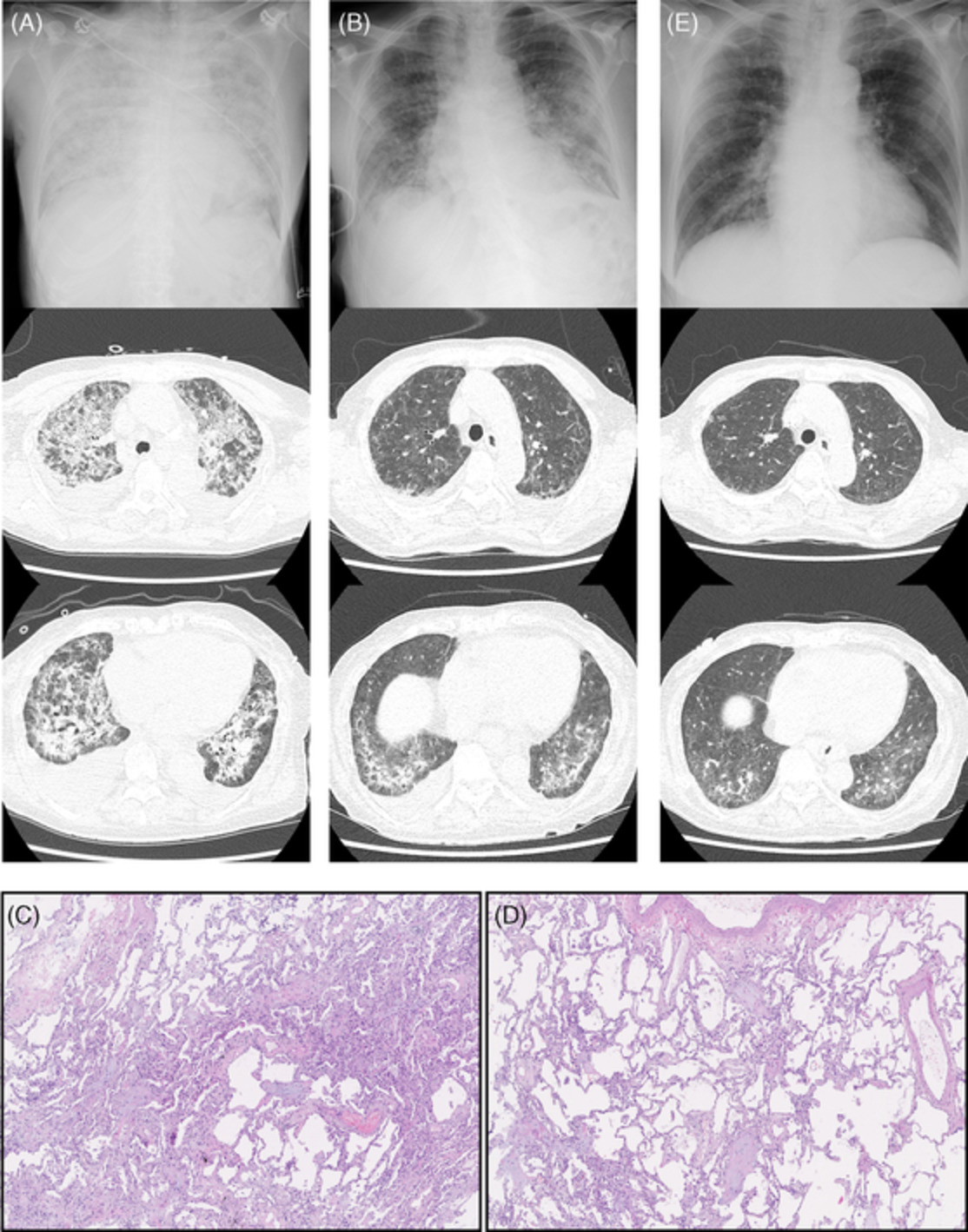
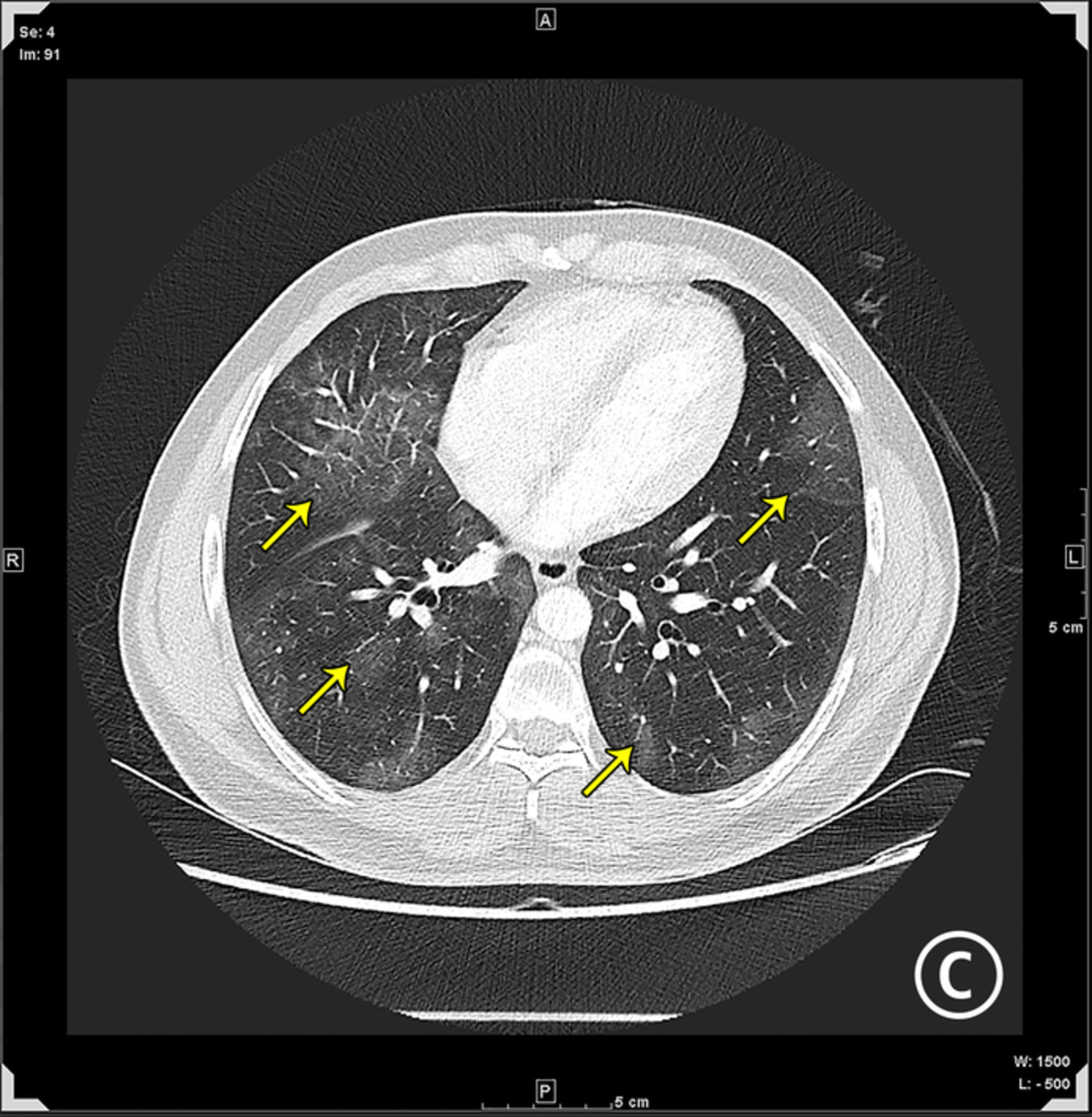
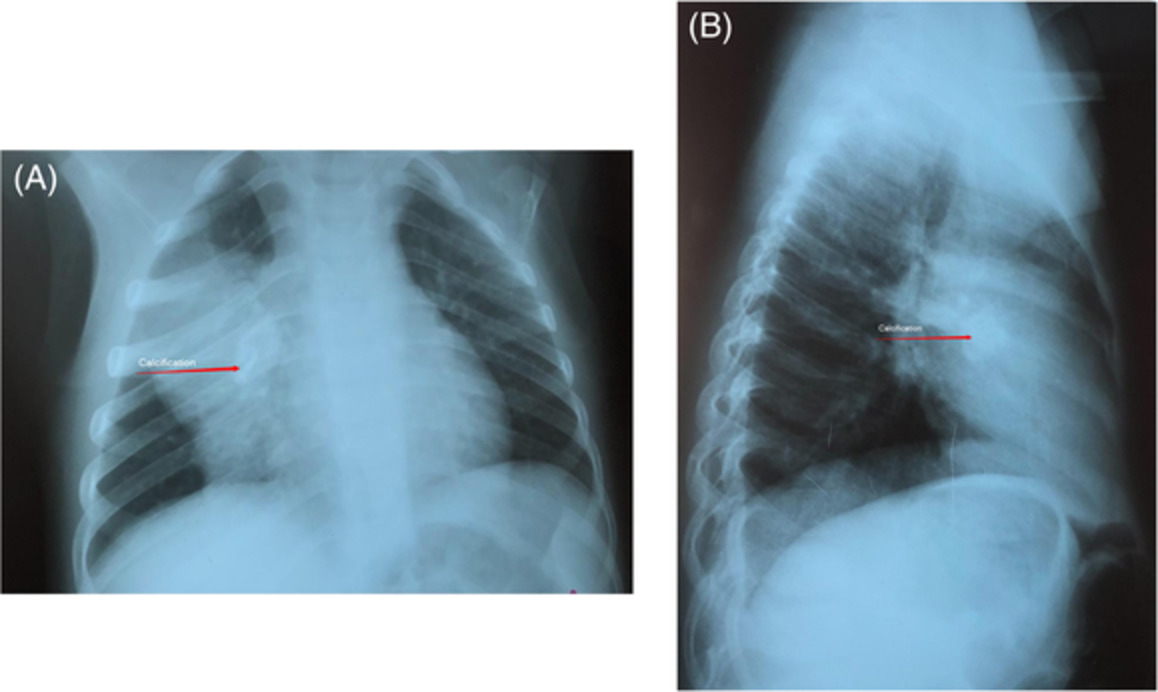
Case 2A 54-year-old Japanese woman with a 40-year history of bronchial asthma was previously diagnosed with severe COVID-19 infection, associated with ARDS, hypoxaemic respiratory failure and required invasive mechanical ventilation at a previous hospital (Figure 2A,B). She received methylprednisolone (80 mg/day) for 3 days, favipiravir for 14 days, remdesivir for 10 days and intravenous immunoglobulin for 3 days. Immunotherapy with tocilizumab (8 mg/kg) was also administered. During the first month after these treatments began, the patient's general condition gradually improved. A percutaneous tracheostomy was inserted for ventilatory weaning. Two months later, she was referred to our hospital; her oxygen saturation was 99% on positive end-expiratory pressure at 4 cm H2O and her fraction of inspired oxygen was 30% via a tracheostomy tube. She was extremely obese (body mass index, 38.2 kg/m2). Laboratory data showed high serum levels of lactate dehydrogenase (270 IU/L), KL-6 value of 1222 U/ml and a surfactant protein-D (SP-D) value of 447 ng/ml. Arterial blood gas analysis revealed a pH of 7.59, partial pressure of carbon dioxide of 30.5 mmHg and partial pressure of oxygen of 54.2 mmHg in room air. Diffuse reticular and GGOs accompanying interlobular septal thickening and architectural distortion in the bilateral lung lobes were evident on the chest HRCT (Figure 2C,D). We initiated combination therapy of prednisolone (30 mg/day) and tacrolimus (3 mg/day) when the patient was admitted. We chose tacrolimus but cyclosporine because she has received rosuvastatin for hyperlipidaemia. One month later, her clinical condition had gradually improved. However, she demonstrated respiratory failure, with incomplete response to corticosteroids, and reticulation associated with traction bronchiectasis was detected on follow-up HRCT (Figure 2E,F). As a result, we performed VATS to decide whether to add antifibrotic treatment such as nintedanib. The lung biopsy specimens of the right upper lobe and lower lobe revealed extensive intra-alveolar granulation tissue, mural organization with fibrosis and alveolitis with infiltration of a small number of lymphocytes, but no findings of DAD (Figure 2I,J). SARS-CoV-2 detection using reverse transcription polymerase chain reaction on formalin-fixed paraffin-embedded sections of the lung biopsy resulted negative. Nintedanib was added to the regimen of prednisolone plus tacrolimus. Most lung abnormalities on HRCT had resolved 6 months later, but some interlobular septal thickening and residual reticulation were observed (Figure 2G,H). Although her DLCO remained unchanged (6.46 ⇒ 6.94 ml/min/mmHg), FVC increased from 1.18 to 1.63 L. Serum KL-6 and SP-D also decreased from 1222 to 505 U/ml, and from 447 to 153 ng/ml, respectively. She has since experienced no serious adverse effects.

Serial changes in high-resolution computed tomography (HRCT) of the chest in case 2. (A, B) At the previous hospital, HRCT revealed diffuse ground-glass opacities (GGOs) in both lungs. (C, D) At admission, HRCT imaging revealed diffuse reticular and GGOs accompanying interlobular septal thickening and architectural distortion in the bilateral lung lobes. (E, F) One month after we initiated combination therapy with corticosteroid and calcineurin inhibitors, reticulation in association with traction bronchiectasis, suggestive of pulmonary fibrosis, was observed. (G, H) Six months after the start of therapy, chest HRCT showed interlobular septal thickening and GGOs over a slightly smaller area. (I) Histopathological findings of the lung biopsy specimens obtained by video-assisted thoracoscopic surgery. Low-magnification microscopy showed extensive intra-alveolar granulation tissue and mural organization with fibrosis (Elastica van Gieson stain; bar represents 250 μm). (J) High-magnification microscopy showed alveolitis with a small number of inflammatory cells infiltration and loose intra-alveolar and mural organization with fibrosis (haematoxylin–eosin stain; bar represents 100 μm)
DISCUSSIONTo the best of our knowledge, these are the first reported cases of lung sequelae post-COVID-19 confirmed histopathologically as diagnosis of organizing pneumonia (OP) without DAD on VATS.
Wang et al. reported that 94% of patients with COVID-19 who were discharged from their hospital had mild to substantial residual lung abnormalities on their last CT scans (median of 24 days after symptom onset).1 According to a prospective longitudinal cohort study reported by Han et al., 40 (35%) of 114 patients who recovered from severe COVID-19 pneumonia developed lung fibrosis-like changes within 6 months.2 Our patients also had severe hypoxaemia and residual CT abnormalities 1 month after the treatment for severe COVID-19 pneumonia.
Whether the pathophysiological features of severe COVID-19 pneumonia constitute a typical form of ARDS or a distinct form of lung injury is unclear. Several autopsy studies demonstrated that DAD was the primary histopathological finding in patients with fatal COVID-19 pneumonia. In contrast, Vadász et al.3 recently reported that COVID-19-associated ARDS developed severe OP and corticosteroid therapy might be more beneficial. OP is a distinct clinicopathological entity that may occur as a pulmonary reaction to various injuries, including ARDS or lung injury due to prolonged mechanical ventilation. Although cryptogenic OP (COP) or viral-induced secondary OP such as severe acute respiratory syndrome, Middle East respiratory syndrome and the 2009 H1N1 pandemic have been well described, COVID-19-induced secondary OP is poorly recognized.4 In addition, we believe that it is difficult to distinguish COP from secondary OP with regard to clinical and radiological features and response to corticosteroid therapy.
In our two patients, histopathological findings proved the features of OP without DAD. Thus, our findings suggest that immunosuppressive therapy may be highly effective for patients who have recovered from severe COVID-19 pneumonia but later developed severe OP following COVID-19. Corticosteroid therapy for patients with persistent post-COVID-19 interstitial lung disease has previously been described as a potential treatment for preventing irreversible impairment.5 Although case 2 was treated with immunosuppressive agents for 1 month, she had severe respiratory failure and reticulation associated with traction bronchiectasis on chest HRCT, which was suggestive of pulmonary fibrosis. Moreover, lung biopsies showed extensive well-recognized OP pattern, mural organization with fibrosis and interstitial infiltration of a small number of chronic inflammatory cells. We speculate that severe or fatal COVID-19 infection, driven by immune dysregulation, might have provoked pathogenetic profibrotic pathways. Given the clinical course (disease behaviour), HRCT findings suggestive of pulmonary fibrosis and histopathological findings, we decided to administer antifibrotic agents. Therefore, a combination of immunosuppressive and antifibrotic treatments may have greater efficacy against lung sequelae post-COVID-19 with pulmonary fibrosis. In fact, case 2 responded well when nintedanib was administered along with immunosuppressive agents than immunosuppressive agents alone. In conclusion, immunosuppressive or antifibrotic drugs may provide clinical, functional and radiographic improvement in patients with lung sequelae post-COVID-19 associated with OP.
ACKNOWLEDGMENTSThe authors thank Dr A. Kurosaki (Department of Diagnostic Radiology, Fukujuji Hospital, Japan Anti-Tuberculosis Association, Kiyose, Japan) for radiological investigations. The authors also thank Dr Tadaki Suzuki and Dr Minoru Tobiume (Department of Pathology, National Institute of Infectious Diseases, Tokyo, Japan) for detecting SARS-CoV-2 by using reverse transcription polymerase chain reaction on formalin-fixed paraffin-embedded sections of the lung biopsy specimens.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this case report and accompanying images.
Comments (0)