
記住我

Antiviral therapy of chronic hepatitis C with direct-acting antiviral agents [DAA(s)] results in >90% sustained virologic response (SVR) rates including patients with compensated liver cirrhosis.1, 2 The development of DAA-based, interferon-alfa free antiviral therapy in patients with hepatitis C enabled treatment even in patients with (decompensated) cirrhosis or prior liver transplantation.3-5 However, there is still lack of knowledge to what extent cirrhosis including portal hypertension is reversible after HCV eradication in patients with HCV- associated cirrhosis.6-10
In a previous report on our study cohort, we demonstrated an improvement of liver stiffness values between baseline (BL) and end of treatment (EOT) as well as between BL and 24 weeks after EOT (FU 24) in patients with HCV-associated advanced liver disease and DAA-induced SVR.11 Although liver biopsy has been considered the gold standard for the assessment of fibrosis status, it is limited by its rare but potential severe complications. In addition, the accuracy of assessment of cirrhosis by liver biopsy is decreased due to sampling variations, inadequate specimen size and observer variability.12 In recent years, non-invasive methods have been evaluated for the indirect assessment of liver fibrosis and portal hypertension.13, 14 Technologies such as transient elastography or point shear wave elastography (pSWE) using acoustic radiation force impulse (ARFI) have revolutionized the monitoring of patients in daily clinical practice. Transient elastography of the liver (L-TE) and ARFI of the liver (L-ARFI) measure liver stiffness, which correlates with fibrosis.15-17 Regression of liver fibrosis was shown in patients treated with interferon up to 4 years after treatment, particularly in those who achieved SVR.18, 19 In recent years, studies analysing the effect of interferon-free DAA regimens on fibrosis regression have demonstrated short-term reduction in liver stiffness by different elastography techniques within 18 months post-treatment.20-23 However, studies with follow-up intervals beyond several years are scarce.
A number of studies have investigated spleen stiffness as a non-invasive parameter for portal hypertension.24-26 In a recent trial, elevated spleen stiffness measured by ARFI (S-ARFI) represented a reliable non-invasive tool for the prediction of oesophageal varices in HCV-infected patients.27
The aim of the present study was to assess the frequency and degree of fibrosis regression as well as reduction of portal hypertension by liver and spleen elastography in patients with HCV-associated advanced liver disease and DAA-induced SVR up to 3 years post-treatment.
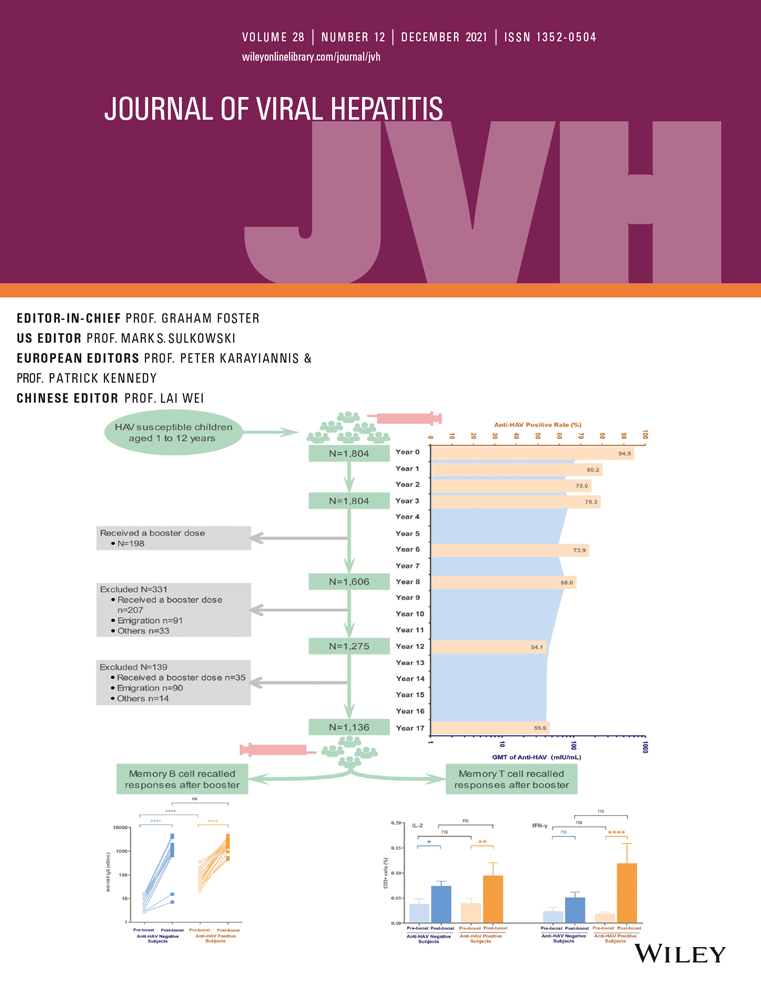
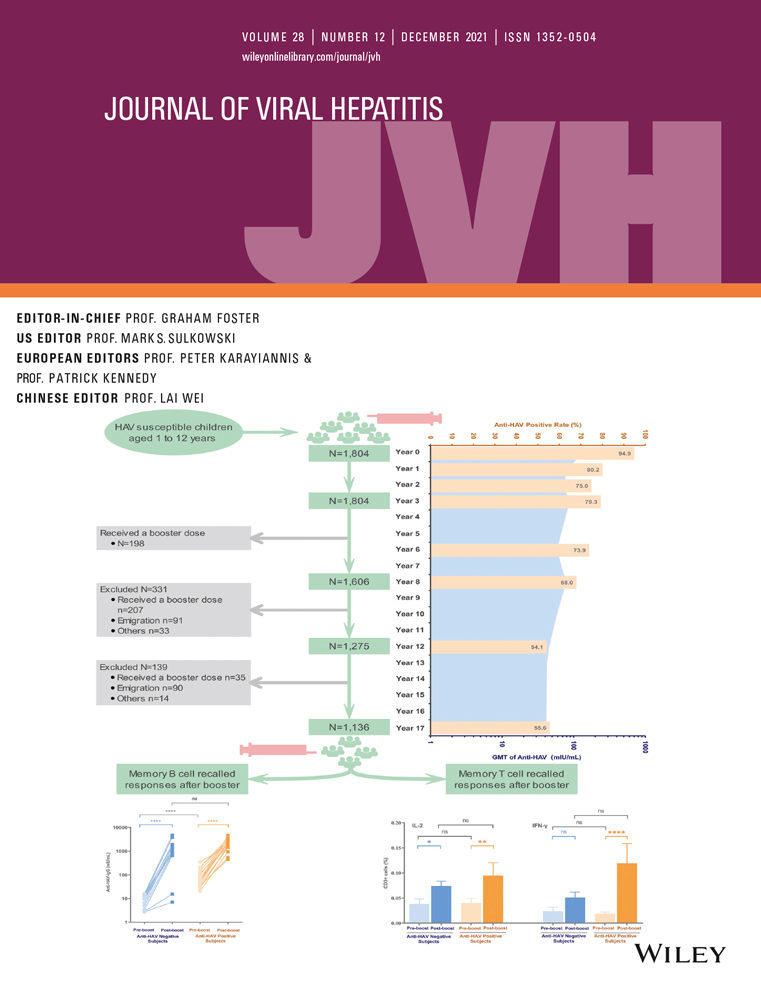
2 MATERIALS AND METHODS 2.1 Patient selection and study designTreatment of chronic hepatitis C within the present prospective study was conducted between 06/2014 and 12/2015 at a German tertiary care centre. The study was performed in accordance with the Declaration of Helsinki and the ICH/CPMP guidelines ‘Good Clinical Practice’ and was approved by the local ethics committee. Written informed consent was obtained from all participants before enrolment. Here, we report the 3 years follow-up update to the initial study report.8 Main inclusion criteria of the initial study and thus the current analysis were confirmation of HCV infection by anti-HCV (third-generation) enzyme immunoassay (Roche Diagnostics, Mannheim, Germany), quantifiable HCV-RNA by quantitative reverse transcription polymerase chain reaction assay [COBAS TaqMan HCV test 2.0 (Roche Diagnostics, Mannheim, Germany)], presence of cirrhosis determined by histology, if available, abdominal ultrasound and/or transient elastography (stiffness values ≥12.5 kPa), and timely planned DAA-based, interferon-free antiviral therapy. Patients with concomitant liver diseases, including autoimmune disorders, coinfection with hepatitis B virus, Wilson's disease, hemochromatosis, systemic infections, preexisting severe psychiatric conditions, significant alcohol consumption (≥40 g/day in women and ≥60 g/day in men) and drug abuse within the past year were excluded from the study. Details of the study design have been reported previously as well as results regarding fibrosis regression and portal hypertension of these patients at end of treatment (EOT) and again at 24 weeks after EOT (FU24).8 A synopsis of the study design including the initial and the current follow-up report is given in Figure 1.

The flow diagram illustrates selection of patients analysed in the study
Clinical and laboratory assessments including routine biochemical liver tests were obtained at baseline (BL) of antiviral therapy, EOT, FU24 as well as at 1, 2 and 3 years post-treatment. Moreover, MELD score28 and CPT score29 were calculated for each patient. APRI Score [AST level (ULN)/(platelet counts (109/l) × 100)]30 was available in a subpopulation (n = 33) at BL, EOT and 3 years post-treatment and was performed retrospectively. Measurements of liver and spleen stiffness were performed at BL, EOT and FU24 as well as at 1, 2 and 3 years post-treatment. In addition, spleen diameter and the presence or absence of ascites were evaluated by conventional B-mode ultrasound.
The choice of antiviral therapy was at the physician's discretion. In detail, all 54 patients included in the analysis received a DAA-based, interferon-free therapy regimen with or without ribavirin for 12 or 24 weeks (Table 1). Treatment details of 43/54 patients were recorded within the European compassionate use programme (Clinical Trials.gov Identifier NCT02097966). Data of those patients have in part been or will be published within reports of the respective programme.31 Moreover, clinical data of three patients were reported within a study focusing on complications before and during antiviral therapy.32
TABLE 1. Patients’ characteristics, virological data and antiviral treatment Parameter Patients (n = 54) n or median (range) Age (years) 57 (30–86) Gender male/female (n/n) 37/17 Ethnicity (n) Caucasian 48 Non caucasian 6 HIV coinfection (n) 2 Prior or current HCC (n)a 2 Prior liver transplantation (n) 5 Ascites (n) 4 Body mass index (kg/m2) 26.1 (19–44) Bilirubin (mg/dl) 1.1 (0.4–5.4) Albumin (g/dl) 3.7 (2.8–4.9) INR 1.13 (0.9–1.5) AST (U/l) 82 (17–260) ALT (U/l) 71 (17–254) Platelets (/nl) 90 (28–223) APRI Score (AST * 100/109/l) 2.5 (0.3–15) CTP Score 5 (5–9) MELD Score 9 (6–17) HCV genotype distribution 1a/1b/3/4 (n) 19/17/13/5 Baseline HCV RNA (log10 IU/ml) 6.02 (4.19–7.01) Liver FibroScan (kPa)b 32.4 (9.1–75) Liver ARFI (m/s) 2.7 (1.2–4.1) Spleen ARFI (m/s) 3.4 (2–4.3) Spleen diameter (cm) 14.7 (9–21) Treatment details Daclatasvir +Sofosbuvir ± Ribavirin (n) 36 Sofosbuvir +Ledipasvir ± Ribavirin (n) 12 Simeprevir +Sofosbuvir ± Ribavirin (n) 5 Ombitasvir/Paritaprevir/Ritonavir + Dasabuvir (n) 1 Abbreviations: ALT, alanine aminotransferase; ARFI, acoustic radiation force impulse; AST, aspartate aminotransferase; HCC, hepatocellular carcinoma. a Patients had prior radiofrequency ablation. b In 4 of 54 patients, liver FibroScan was not applicable due to ascites. 2.2 Transient elastography (TE)Patients were placed on a supine position with elevated arms above their heads. Liver transient elastography (L-TE) was carried out with the FibroScan® 502 Touch device (Echosens, Paris, France) which incorporates an ultrasound transducer probe mounted on the axis of a vibrator. The vibrator generates painless vibration with a frequency of 50 Hz, which leads to an elastic shear wave propagating through the skin and the subcutaneous tissue to the liver. Shear wave velocity (expressed in kilopascal, kPa) is directly related to the stiffness of the tissue.33 Stiffness measurements were performed with a 3.5-MHz transducer (‘M-probe’) in patients with a skin capsule distance (SCD) ≤25 mm and with a 2.5-MHz transducer (‘XL-probe’) in patients with a SCD >25 mm, respectively. The fasting interval between last food intake and measurement was assigned to at least 4 h.34 Ten measurements were taken to obtain the median number in kilopascal. Unreliable measurements were defined as an interquartile range (IQR) to median value ratio greater than 30% and a success rate (SR) less than 60%. These thresholds were chosen, because they were reported to improve inter-variability and intra-variability discrepancies.35, 36 For diagnosing liver cirrhosis, the cut-off value of 12.5 kPa was used.37
2.2.1 Point shear wave elastography (pSWE) using acoustic radiation force impulse (ARFI)Patients were placed on a supine position with elevated arms above their heads. Liver (L-ARFI) and spleen (S-ARFI) ARFI were performed with a Siemens AcusonS2000TM (Siemens AG, Erlangen, Germany) ultrasound system. The ultrasound probe produces an acoustic ‘push’ impulse that generates shear waves, which propagate into the tissue. Their speed is measured in metres per second (m/s). The propagation speed increases with fibrosis severity.16, 38, 39 Ten measurements were carried out for liver and spleen stiffness, respectively, on the right liver lobe as well as at the level of the lower pole/middle third of the spleen. The measurement box was placed 2 cm deep in projection on the hepatic and splenic parenchyma, respectively. The recommended examination standards published by Karlas et al.40 were used to minimize the overestimation of spleen stiffness values. An L-ARFI cut-off value of 1.8 m/s (or higher) was used to determine presence or absence of cirrhosis.38
2.2.2 Ascites and splenic length diameter measurementAscites and splenic length measurement, presence of ascites and splenic length diameter were obtained by use of a Siemens AcusonS2000™ (Siemens AG) ultrasound system.
2.2.3 Statistical analysesData were expressed as median and range for continuous variables in addition to both frequency and percentage for categorical variables. Box plots of liver and spleen stiffness values as well as APRI Score were provided at different time points between BL and three years post-treatment illustrating median changes of individual patient data shown as absolute values. Wilcoxon test was applied for comparison of two paired groups. Univariate and multivariate regression analyses were performed to identify baseline factors (continuous variables) as predictors of liver stiffness improvement. All tests were two-sided, and statistical significance was defined as p < .05. Data were analysed by using the statistical software package SPSS 24 for Windows.
3 RESULTS 3.1 Patient characteristicsBetween June 2014 and December 2015, a total of 54 patients who had achieved SVR to DAA-based therapy were included in the present analysis. Three-year follow-up data (FU144) were available in 41 patients (refusal of follow-up, n = 5; liver transplantation, n = 4; fatal outcome, n = 4 (Figure 1)). Main baseline characteristics are given in Table 1. A minority of patients (2 of 54) was co-infected with human immunodeficiency virus (HIV), and 2 of 54 had a history of HCC prior to antiviral therapy.
3.1.1 Changes of liver and spleen stiffness as well as APRI Score between baseline (BL) and 3 years post-treatment (FU 144)As shown in Figure 2A, asignificant decline of liver stiffness assessed by L-TE was observed between BL [median (range), 32.5 (9.1–75) kPa] and EOT [median (range), 21.3 (6.7–73.5) kPa; p < .0001], and there was continued improvement between EOT and FU144 [median (range), 16 (4.1–75) kPa; p = .006].

(A). Changes of liver stiffness assessed by L-TE between baseline (BL) and 3 years post-treatment (FU144). At BL (*), L-TE was not applicable in 4 patients due to ascites. At EOT (**), L-TE was not feasible in 1 patient due to ascites. At FU144 (***), L-TE was not applicable in 2 patients due to increased BMI. 13 patients had premature termination of the study. Whisker and box plots represent medians, first and third quartiles and range. (B) Changes of liver stiffness assessed by L-ARFI between baseline (BL) and 3 years post-treatment (FU144). At EOT (*), 1 patient refused L-ARFI. At FU144 (**), L-ARFI was not applicable in 1 patient due to increased BMI. 1 patient refused L-ARFI. 13 patients had premature termination of the study. Whisker and box plots represent medians, first and third quartiles and range. (C) Changes of spleen stiffness assessed by S-ARFI between baseline (BL) and 3 years post-treatment (FU 144). At BL (*), S-ARFI was not applicable in 1 patient due to splenectomy. At EOT (**), S-ARFI was not feasible in 1 patient due to splenectomy. 1 patient refused S-ARFI. At FU144 (***), S-ARFI was not applicable in 1 patient due to increased BMI. 2 patients had prior splenectomy. 1 patient refused S-ARFI. 13 patients had premature termination of the study. Whisker and box plots represent medians, first and third quartiles and range. (D) Changes of APRI Score between baseline (BL) and 3 years post-treatment (FU 144) in a subgroup of patients (n = 33). 13 patients had premature termination of the study. In 8 patients, we had missing values. Whisker and box plots represent medians, first and third quartiles and range
A significant reduction in liver stiffness measured by L-ARFI was observed between EOT [median (range), 2.5 (1.2–4.11) m/s] and FU144 [median (range), 1.7 (0.9–4.1) m/s; p = .001] (Figure 2B). However, no significant decrease of L-ARFI values was found between BL [median (range), 2.7 (1.2–4.1) m/s] and EOT [median (range), 2.5 (1.2–4.1) m/s; p = .278].
Spleen stiffness assessed by S-ARFI did not show any significant changes between BL [median (range), 3.4 (1.9–4.3) m/s] and EOT [median (range), 3.4 (2.3–4.3) m/s; p = .74] or FU144 [median (range), 3.3 (1.8–4.1) m/s; p = .138)] (Figure 2C).
A subanalysis of n = 33 patients revealed a significant decrease in APRI score between BL [median (range), 2.5 (0.3–15)] and EOT [median (range), 0.8 (0.2–3.6); p < .0001] with continued improvement between EOT and FU144 [median (range), 0.7 (0.1–4); p = .024] (Figure 2D).
Changes of biochemical markers, such as ALT, platelets and albumin, are shown in Supplement Figure 1.
3.1.2 Improvement of liver stiffness by TE and ARFI methods between BL and FU 144Overall, 38 of 54 patients (70.4%) achieved improvement of liver stiffness by TE at EOT and 29 of 38 (76.3%) declined further until FU144 (Figure 3A).

(A) Improvement of liver stiffness assessed by TE between BL and EOT as well as between EOT and FU144. Changes are given in absolute LSM value. (B) Improvement of liver stiffness assessed by ARFI between BL and EOT as well as between EOT and FU144. Changes are given in absolute LSM value. (C) Patients were classified to be non-cirrhotic (<12.5 kPa; <1.8 m/s) or cirrhotic (≥12.5 kPa; ≥1.8 m/s) by TE and ARFI methods at FU144
By L-ARFI, 30 of 54 patients (55.6%) presented a decrease in liver stiffness at EOT and 28 of 30 (93.3%) continued to improve until FU144 (Figure 3B).
At FU144, 16 and 20 patients were classified to be non-cirrhotic by TE (<12.5 kPa) and ARFI (<1.8 m/s) methods compared to 23 and 19 patients with estimated cirrhosis (≥12.5 kPa; ≥1.8 m/s) (Figure 3C).
3.1.3 Univariate and multivariate analysis of baseline factors for association with improvement of liver stiffness by TE and ARFI methods between BL and FU 144Univariate analysis indicated that high albumin was the only baseline parameter that predicts reduction in liver stiffness by TE between EOT and FU144 (p = .029) (Table 2).
TABLE 2. Univariate and multivariate analysis of baseline factors for association with improvement of liver stiffness by TE between BL and EOT as well as between EOT and FU144 BL->EOT EOT->FU144 Univariate analysis p Multivariate analysis p Univariate analysis p Multivariate analysis p Odds ratio (95% CI) Odds ratio (95% CI) Odds ratio (95% CI) Odds ratio (95% CI) Gender 0.985 (0.280–3.469) >.05 >.05 0.956 (0.302–3.023) >.05 >.05 Age 1.007 (0.952–1.066) >.05 >.05 0.967 (0.916–1.021) >.05 >.05 BMI 0.976 (0.874–1.089) >.05 >.05 1.024 (0.923–1.135) >.05 >.05 Bilirubin 0.615 (0.330–1.147) >.05 >.05 1.137 (0.640–2.018) >.05 >.05 Albumin (high) 1.466 (0.499–4.304) >.05 >.05 0.300 (0.102–0.883) .029 >.05 AST 1.009 (0.997–1.022) >.05 >.05 0.997 (0.987–1.006) >.05 >.05 ALT 1.007 (0.996–1.019) >.05 >.05 0.995 (0.986–1.005) >.05 >.05 INR 0.367 (0.008–17.558) >.05 >.05 22.964 (0.503–1048.047) >.05 >.05 Platelets 0.995 (0.984–1.006) >.05 >.05 0.996 (0.985–1.007) >.05 >.05 Genotype 1 0.769 (0.227–2.610) >.05 >.05 0.894 (0.287–2.787) >.05 >.05 Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BL, baseline; EOT, end of treatment; FU144, 144 weeks post-treatment; INR, international normalized ratio; TE, transient elastography.Moreover, low total bilirubin serum levels (p = .048) and low INR values (p = .048) at BL were associated with improvement of stiffness between BL and EOT measured by L-ARFI. By multivariate analysis, only bilirubin remained significantly associated with improved L-ARFI values (p = .048) (Table 3).
TABLE 3. Univariate and multivariate analysis of baseline factors for association with improvement of liver stiffness by ARFI between BL and EOT as well as between EOT and FU144 BL-> EOT EOT->FU144 Univariate analysis p Multivariate analysis p Univariate analysis p Multivariate analysis p Odds ratio (95% CI) Odds ratio (95% CI) Odds ratio (95% CI) Odds ratio (95% CI) Gender 1.244 (0.390–3.970) >.05 >.05 0.938 (0.297–2.963) >.05 >.05 Age 1.027 (0.973–1.084) >.05 >.05 1.024 (0.972–1.080) >.05 >.05 BMI 0.987 (0.890–1.095) >.05 >.05 0.998 (0.900–1.106) >.05 >.05 Bilirubin (low) 0.452 (0.206–0.994) .048 0.452 (0.206–0.994) .048 0.920 (0.519–1.630) >.05 >.05 Albumin 2.088 (0.742–5.875) >.05 >.05 2.047 (0.748–5.603) >.05 >.05 AST 1.003 (0.993–1.014) >.05 >.05 1.002 (0.992–1.011) >.05 >.05 ALT 1.006 (0.996–1.016) >.05 >.05 1.004 (0.995–1.013) >.05 >.05 INR (low) 0.019 (0.000–0.961) .048 >.05 0.750 (0.002–3.226) >.05 >.05 Platelets 1.005 (0.994–1.016) >.05 >.05 1.003 (0.993–1.014) >.05 >.05 Genotype 1 0.667 (0.212–2.095) >.05 >.05 1.250 (0.401–3.894) >.05 >.05 Abbreviations: 144 weeks post-treatment; ALT, alanine aminotransferase; ARFI, acoustic radiation force impulse; AST, aspartate aminotransferase; BL, baseline; EOT, end of treatment, FU144; INR, international normalized ratio.As shown in Table 4, high albumin (p=0.004) and high platelets at BL (p=0.029) predicted non-cirrhotic status (<12.5 kPa) by TE at FU144. By multivariate analysis, only albumin remained significantly associated with non-cirrhotic status (<12.5 kPa) 3 years post-treatment (p = .005).
TABLE 4. Univariate and multivariate analysis of baseline factors for association with non-cirrhotic status by TE (<12.5 kPa) and ARFI (<1.8 m/s) at FU144 <12.5 kPa at FU144 <1.8 m/s at FU144 Univariate analysis p Multivariate analysis p Univariate analysis p Multivariate analysis p Odds ratio (95% CI) Odds ratio (95% CI) Odds ratio (95% CI) Odds ratio (95% CI) Gender 0.625 (0.151–2.586) >.05 >.05 0.735 (0.193–2.793) >.05 >.05 Age 0.957 (0.898–1.019) >.05 >.05 1.013 (0.957–1.073) >.05 >.05 BMI 1.072 (0.939–1.244) >.05 >.05 1.104 (0.966–1.262) >.05 >.05 Bilirubin 1.361 (0.632–2.932) >.05 >.05 0.798 (0.415–1.537) >.05 >.05 Albumin (high) 0.107 (0.023–0.494) .004 0.107 (0.023–0.502) .005 0.408 (0.127–1.314) >.05 >.05 AST 1.003 (0.992–1.014) >.05 >.05 0.993 (0.982–1.005) >.05 >.05 ALT
留言 (0)