
Remember me
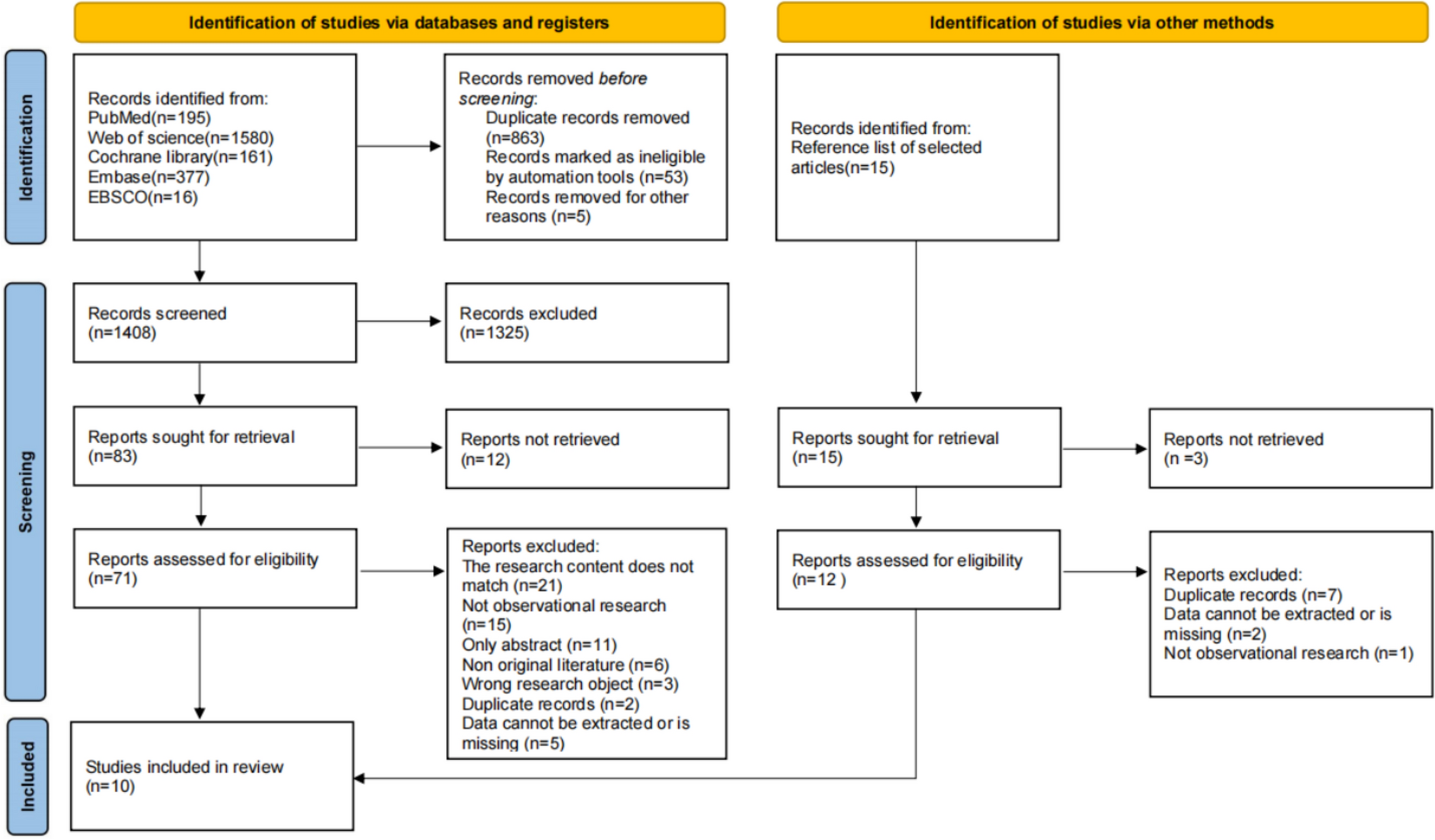

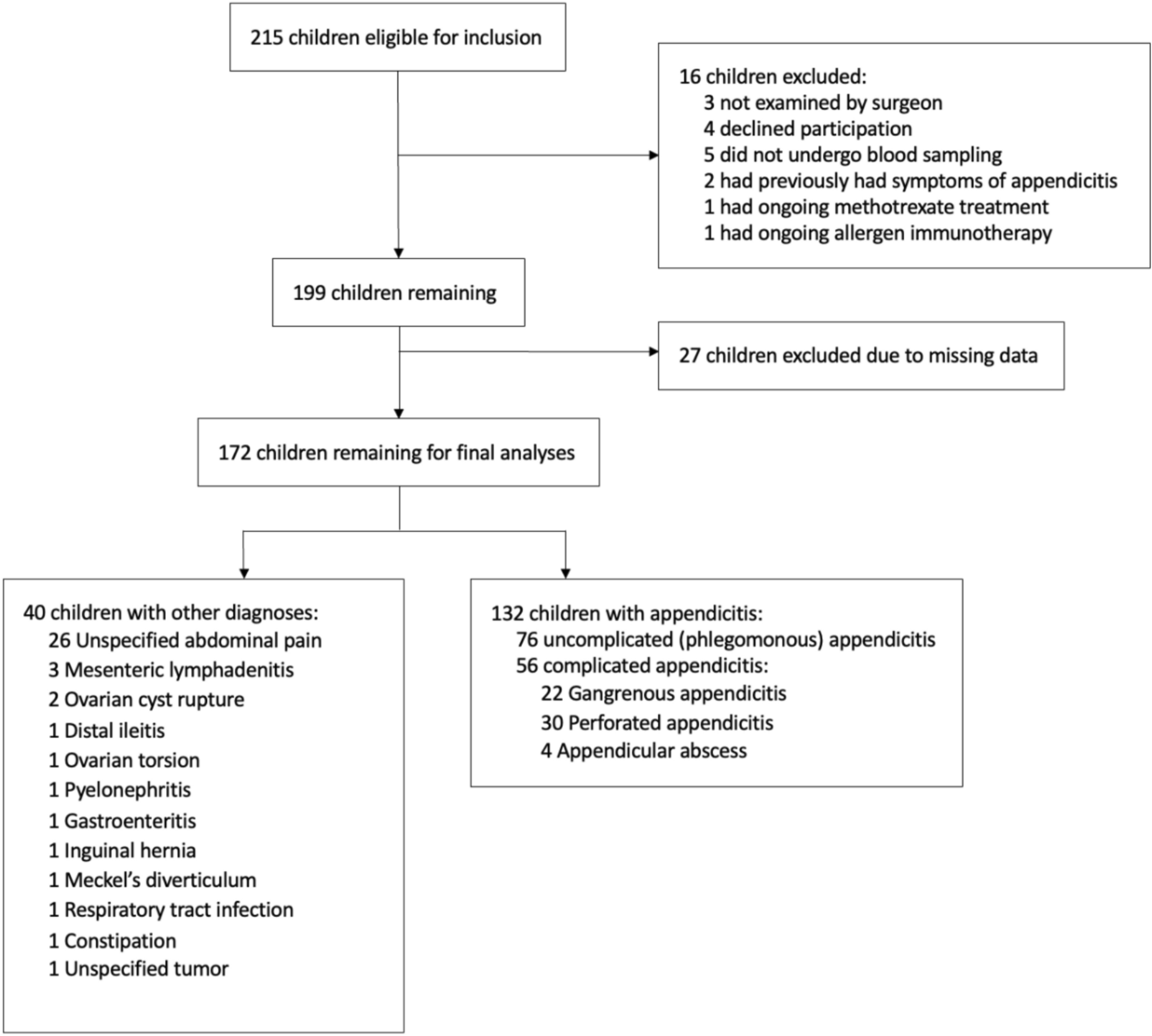


A total of 3838 records were identified from PubMed (969), Scopus (1319), Web of Science (1245), and Cochrane (305). After removing 1,305 duplicates, 2533 records were screened by title and abstract, with 2264 excluded. Full-text assessment was conducted for 269 reports, leading to the exclusion of 258 based on criteria such as review articles (42), editorial comments (16), different diseases (141), different interventions (43), non-English articles (11), and books (5). Ultimately, 11 studies met the eligibility criteria for inclusion [11,12,13, 21,22,23,24,25,26,27,28]. Figure 1
Fig. 1
Flow diagram of the study selection process
Baseline and summary of the included studiesThe included studies encompass various designs, including 6 retrospective cohorts, 3 cross-sectional studies, one prospective cohort, and one case series, conducted across multiple countries, including France, the USA, the UK, Italy, and Russia. Sample sizes range from 15 to 143 pediatric patients, covering diverse conditions such as orthopedic trauma, facial lacerations, intracranial hemorrhages, and abdominal injuries. Telemedicine tools include video conferencing, mobile applications, digital imaging transmission, and tele-ultrasound. Control groups vary, including non-telemedicine care, historical cohorts, and bedside assessments. Primary outcomes focus on diagnostic accuracy, clinical decision-making, time-to-surgery, and telemedicine effectiveness. Specialties involved include orthopedics, radiology, neurosurgery, emergency medicine, and ophthalmology, with injury locations spanning the limbs, head, spine, chest, and abdomen. Table 1
Table 1 Summary of the included studiesThe baseline characteristics of the included studies vary widely. Patient ages range from 0.39 to 13.3 years. GCS is reported in two studies, ranging from 6 to 12.8. Injury Severity Scores range from 10.4 to 31. Male predominance is common, ranging from 46.66% to 71.4%. Falls are a frequent injury mechanism, reported in up to 40.5% of cases. Table 2
Table 2 Baseline characteristics of the included studiesQuality assessmentThe four included diagnostic studies were assessed using the QUADAS-2 tool and were judged to have a low risk of bias across all domains (Fig. 2). Among the retrospective cohort studies, evaluated using the Newcastle–Ottawa Scale (NOS), five were rated as having good quality, while Jackson et al.’s [11] study was classified as poor quality (Table 3). The case series by Elkaim et al. [21], assessed using the Joanna Briggs Institute (JBI) critical appraisal checklist, was determined to be of moderate quality (Table 4).
Fig. 2
Risk of bias assessment using the ROB 2 tool
Table 3 Quality assessment of the included cohort studies using the Newcastle–Ottawa scaleTable 4 Quality assessment of case series study using the Joanna Briggs Institute checklistQualitative synthesisImproved access to careTelemedicine has significantly enhanced access to emergency surgical care for pediatric patients, particularly in rural and underserved areas. Zorin et al. [28] reported a threefold increase in telemedicine consultation requests over 3 years, indicating a growing reliance on this technology to connect patients with specialized care. The study highlighted that 3745 telemedicine requests were received, with 572 categorized as urgent or emergent. This increase reflects the potential of telemedicine to bridge the gap in healthcare access, allowing timely interventions that can prevent unnecessary transfers to distant trauma centers [28]. Similarly, Taylor et al. [25] noted that their telemedicine program prevented 16 unnecessary transfers, demonstrating how telemedicine can keep patients closer to home while still receiving appropriate care [25]. Furthermore, Elkaim et al. [21] emphasized that teleconsultation using Multimedia Messaging Service (MMS) is particularly beneficial for improving remote management of orthopedic patients, allowing for timely decisions regarding transfers and treatment plans [21]. Palombo et al. [24] highlighted the role of telemedicine in facilitating pediatric radiograph consultations, particularly in emergency settings where immediate specialist access is crucial [24]. Martino et al. [12] highlighted the role of telemedicine in providing timely interpretations of pediatric trauma CT scans, which is crucial for effective management and treatment decisions. Their study found that the mean time to interpretation (TTI) was significantly shorter for radiology residents (55.9 min) compared to attending teleradiologists (90.4 min, P < 0.001).
Diagnostic accuracy and reliabilityThe accuracy of remote consultations in pediatric trauma has been a focal point in recent studies. Zennaro et al. [27] found that point-of-care ultrasound (POC US) performed by pediatricians under remote guidance from radiologists yielded a sensitivity of 93.8% and specificity of 99.7% when compared to expert radiologists [27]. This high diagnostic accuracy highlights telemedicine's effectiveness in providing timely and precise assessments, crucial in emergency settings where every minute counts. Whitney et al. [26] reported strong interrater reliability for ultrasound interpretations between bedside and remote evaluators across various pediatric conditions. The κ values for focused assessment with sonography in trauma, intussusception, and hip effusion were 0.748, 0.816, and 0.764, respectively [26]. Percent agreement adjusted for chance was 86%, 80%, and 88%, with κ values of 0.851, 0.8, and 0.747, respectively. Further adjustments revealed agreements of 92%, 81%, and 88%. Additionally, Saleh et al. [13] demonstrated that digital camera imaging of the eye fundus for suspected abusive head injuries achieved a sensitivity of 100% and specificity of 85.7%, further supporting the reliability of telemedicine in pediatric emergency care [13]. Palombo et al. [24] found that telemedicine for pediatric radiographs had a sensitivity of 98.6% and specificity of 82.6%, indicating that telemedicine can effectively aid in diagnosing pediatric injuries [24]. Martino et al. [12] found that radiology residents had comparable discrepancy rates in interpreting pediatric trauma CT scans to attending teleradiologists, demonstrating that telemedicine can maintain diagnostic accuracy across different levels of expertise. Discrepancy (13.3% vs. 13.3%), major discrepancy (4.4% vs. 4.4%), missed findings (9.6% vs. 12.6%), and overcalls (3.7% vs. 0.7%) were similar between residents and attending teleradiologists, with no statistically significant differences (all P > 0.05) [12].
Enhanced training and educationTelemedicine serves as a valuable educational tool for healthcare providers. In the study by Taylor et al. [25], the implementation of a pediatric trauma telemedicine program led to increased comfort among emergency medicine providers in managing head-injured patients [25]. The program included regular educational sessions, which helped improve the knowledge and skills of the staff at the partnering hospital. This aspect of telemedicine is vital, as it promotes a collaborative learning environment where providers can enhance their competencies while delivering care. Similarly, Marcin et al. [23] highlighted the importance of telemedicine in providing pediatric critical care consultations, emphasizing that telemedicine can help bridge the knowledge gap for providers in rural settings, ultimately improving patient outcomes [23]. Palombo et al. [24] also noted that the use of telemedicine in interpreting pediatric radiographs can serve as a training opportunity for emergency department staff, enhancing their diagnostic skills [24]. Martino et al. [12] suggested that focused training for radiology residents in pediatric trauma imaging is essential to improve interpretation accuracy, indicating the need for ongoing education in telemedicine applications [12].
Cost-effectiveness and resource utilizationJackson et al. [11] highlighted that telemedicine in interhospital transport accelerates definitive care for pediatric intracranial hemorrhage, potentially improving outcomes, reducing hospital stays, and enhancing cost efficiency [11]. Palombo et al. [24] also suggested that the use of telemedicine could reduce the need for unnecessary transfers and consultations, ultimately saving costs for healthcare systems [24].
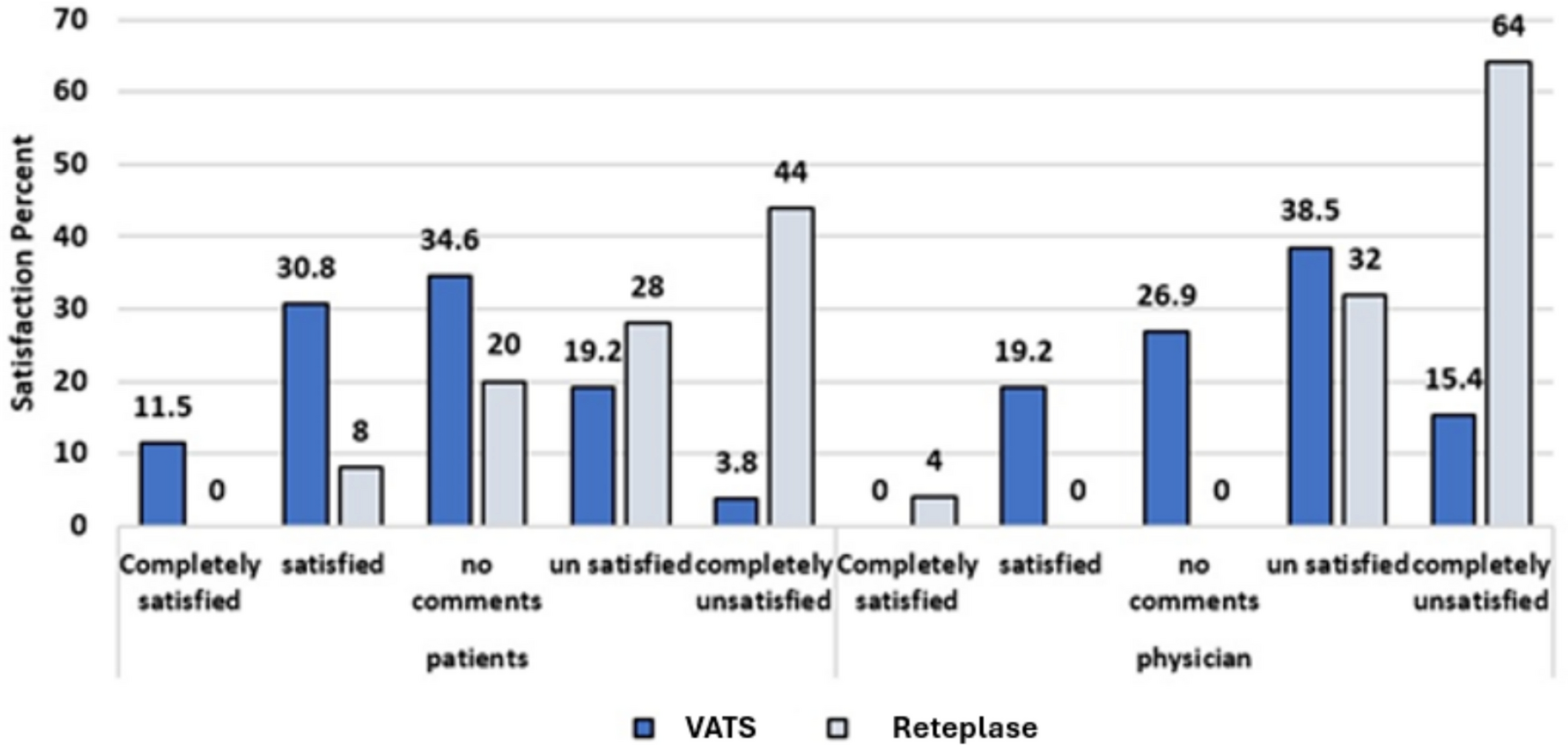
Patient and family satisfactionFarook et al. [22] reported high levels of satisfaction among families who utilized telemedicine for pediatric facial lacerations, with 86% (Vs 82% in the verbal consultation group) of patients undergoing surgery after teleconsultation. The ability to consult with specialists without the need for travel can reduce the stress and anxiety associated with emergency care, allowing families to remain close to their support systems during critical times [22]. This aspect of telemedicine is particularly important in pediatric care, where the emotional well-being of both the child and family is important. Moreover, the study by Marcin et al. [23] indicated that telemedicine consultations resulted in high satisfaction rates among parents and providers, reinforcing the positive impact of telemedicine on the overall healthcare experience [23]. Palombo et al. [24] also found that the use of telemedicine for pediatric radiographs led to high satisfaction levels among emergency department staff, as it facilitated quicker consultations and improved patient management [24].
Challenges and limitationsDespite the numerous benefits, challenges remain in the implementation of telemedicine in pediatric trauma care. Zorin et al. [28] identified issues such as mismatched urgency categories in consultation requests and delays in obtaining telemedicine consultations. These challenges can hinder the effectiveness of telemedicine, potentially leading to adverse outcomes for patients. Additionally, the reliance on technology can pose barriers in areas with limited internet access or inadequate training for healthcare providers [28]. Elkaim et al. [21] also noted that while teleconsultation using Multimedia Messaging Service (MMS) was effective, concerns about patient confidentiality and the quality of transmitted images remained significant challenges [21]. Palombo et al. [24] highlighted that while telemedicine can aid in diagnosing pediatric injuries, there is still a risk of misdiagnosis or overdiagnosis, which can lead to unnecessary treatments [24]. Martino et al. [12] further emphasized that both radiology residents and attending teleradiologists require focused training in pediatric trauma imaging to mitigate discrepancies in interpretations [12] (Fig. 3).
Fig. 3
Challenges and limitations of pediatric surgical emergency and trauma care
Integration of technology and trainingZennaro et al. [27] emphasized the need to train pediatricians in point-of-care ultrasound under remote guidance to ensure accurate diagnoses. Successful telemedicine programs depend on healthcare providers' ability to adopt new technologies effectively [27]. Similarly, Martino et al. [12] highlighted the importance of ongoing training for radiology residents and teleradiologists to improve pediatric trauma imaging accuracy, underscoring the crucial role of technology and training in enhancing pediatric care quality [12].
Comments (0)