
Remember me



Pressure applied on the esophagus, an a priori result of encircling the distal esophagus as a mechanism of conventional anti-reflux procedures, may result in troublesome AEs (i.e., dysphagia, gas-bloating syndrome, and the inability to belch or vomit) that occur in 40–50% of patients after 5 years [13, 14]. Such post-operative manifestations are consequential from the patient perspective due to detrimental effects on quality of life. Moreover, since the introduction of PPIs in 1989, the sequelae associated with conventional anti-reflux modalities have been cited as contributing factors in the decline of surgical management of GERD in recent decades [5, 15,16,17]. However, with over one-third of patients lacking adequate relief of symptoms using PPI therapy or unwilling to continue lifelong medication, anti-reflux surgical alternatives are necessary to fulfill this substantial unmet need without significant trade-offs.
The 3-year clinical outcomes presented in this report demonstrate sustained safety and effectiveness of RefluxStop surgery, consistent with the initial successful outcomes of the published 1-year results [10]. In brief, subjects experienced substantial improvements in quality of life, symptomatology, PPI intake, and satisfaction without notable sequelae non grata, likely pertinent to the novel treatment approach employed by the RefluxStop procedure.
More specifically, clinical effectiveness showed a median 93.1% improvement in GERD-HRQL score, 100% reduction in daily PPI intake, 97.9% achievement of patient satisfaction or neutrality, and 91.5% achievement of ≥ 50% reduction in reflux symptoms (as measured by GERD-HRQL score) at 3-year follow-up of our study. Notably, three of four subjects with < 50% reduction in GERD-HRQL score and the solitary patient dissatisfied with treatment underwent 24-h pH monitoring that yielded objectively normal values, indicating that these subjective outcomes were likely unrelated to GERD. Regurgitation and gas-bloating, typical symptoms of reflux disease, were prominent at baseline in 86.0% and 84.0% of subjects, respectively. Three years after RefluxStop surgery, 97.9% of subjects experienced complete resolution of regurgitation or only occasional episodes, and gas-bloating resolved or improved in 80.9% of subjects.
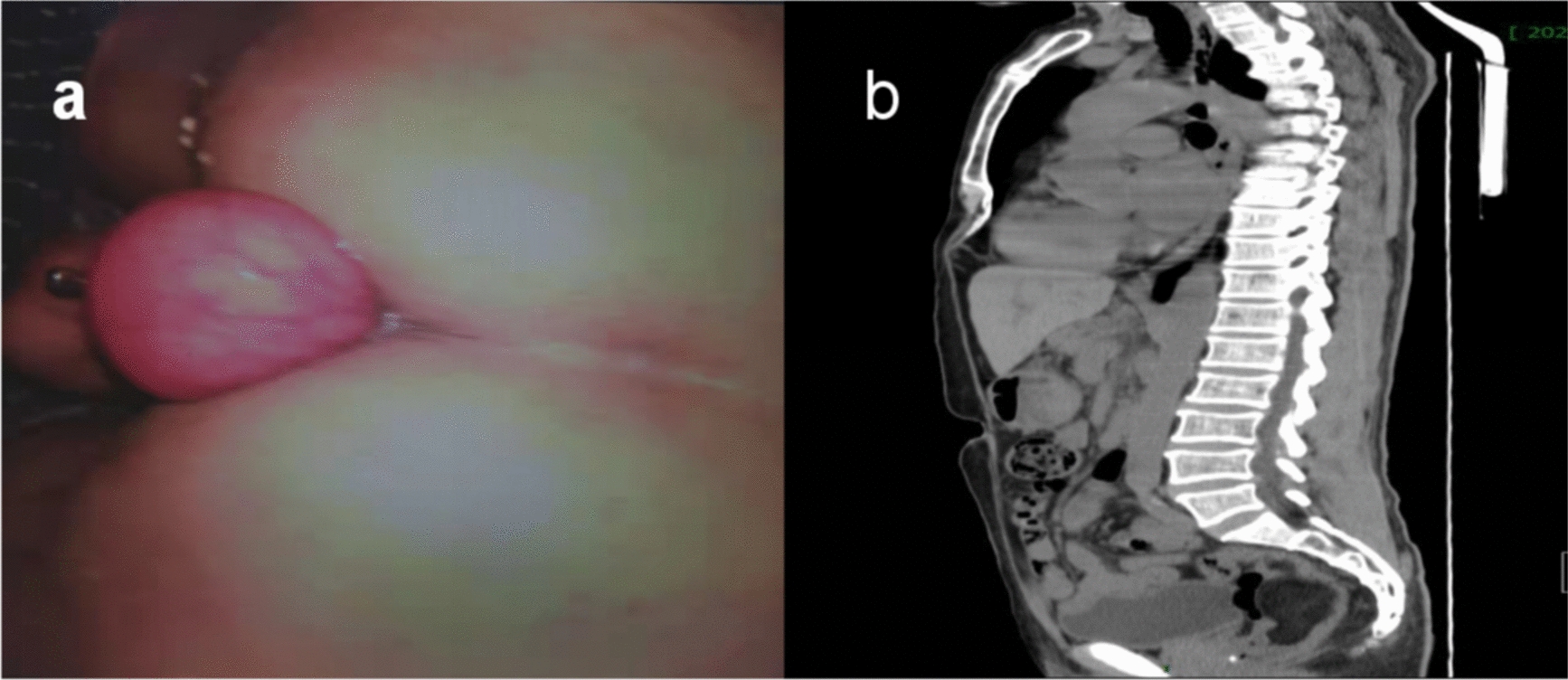
Contrast-swallow x-ray during initial post-operative hospital stay showed that the device was inadequately placed in a low position for the subject with reflux symptoms verified by pH testing, categorized as Failure Risk (see Fig. 2), which does not always preclude optimal surgical outcomes. Considering this ongoing trial included the first ever patients undergoing RefluxStop surgery, the inherent learning curve of a new surgical technique for any surgeon may explicate this observation, as with any other procedure. Device positioning is of critical importance as treatment success is contingent on the RefluxStop implant maintaining the LES sufficiently inferior in the abdomen to allow for normal LES contractility.
Fig. 2
Height categories of device positioning—device size 2.5 cm
According to these results, RefluxStop surgery provides favorable effectiveness and complication profiles, although head-to-head study against standard-of-care anti-reflux surgery is required to verify this. The RefluxStop procedure involves a loose invagination of the device in a fundal pouch, hanging in a teardrop shape when viewed from inside the stomach cavity via endoscopy. This design feature of the procedure is intended to reduce adhesions to other organs and provide stable positioning of the device. The procedure and device design are intended to limit any possible migration/erosion to enter only the stomach cavity, wherein the device is formulated in five segments that exit through the digestive tract, likely without any re-operative measures. During the entire 3-year study period, no cases of device-related AEs, mortality, deficiency, explantation, erosion and migration, SADEs, ADEs, or esophageal dilatation occurred. Only one subject experienced mild dysphagia (as determined by GERD-HRQL dysphagia subscore > 2) between 1-and 3-year follow-up.
RefluxStop surgery is postulated to offer advantages over the current standard-of-care surgical treatment due to its unique approach. Current surgical standard-of-care does not address the root cause of failure in the ARB (i.e., anatomical/physiological misalignment of the gastroesophageal junction) but instead encircles and puts pressure on the food conduit as a mechanism of action to maintain LES closure and prevent retrograde flow of gastric substance, while unintentionally impeding the naturally dynamic process of alimentation [6,7,8]. In fact, a recent (2020) study using objective intra-operative evaluation determined that diaphragmatic re-alignment and subdiaphragmatic re-positioning of the ARB constituents provided approximately four times the treatment effect of sphincter augmentation alone [18]. This indicates that it is logical that a broader attention to ARB correction with RefluxStop surgery may a priori provide superior clinical efficacy compared to techniques that solely focus on reinforcing the LES (i.e., fundoplication and MSA). Additional studies in the future can further validate this assertion.
Several published studies present clinical outcomes of conventional LARS techniques, however, incongruence in outcome measures and sample demographics constrain the ability for direct comparison. Bonatti et al. assessed PPI use for up to 3 years after conventional LARS and found that 39% of subjects required anti-reflux medication, albeit a substantial proportion was deemed inappropriate [19]. Bonavina et al. conducted a prospective multicenter observational registry study from their clinical practice performing MSA and laparoscopic fundoplication (LF), which included Nissen, Toupet, and other/unspecified fundoplication techniques, though the majority were Nissen or Toupet fundoplication. At 3 years post-surgery, they observed a mean reduction in GERD-HRQL score from a baseline of 22.0 to 4.6 (79.1%) for MSA and from 23.6 to 4.9 (79.2%) for LF; 78.2% of MSA patients and 76.5% of LF patients reported satisfaction (based on GERD-HRQL question). Also at 3 years, difficulty belching was reported by 2.4% after MSA and 8.3% after LF; difficulty vomiting was reported by 8.8% after MSA and 32% after LF. PPI usage at 3 years was prevalent in 24.2% of those with MSA and 19.5% of those with LF. Although intra-operative and procedure-related complication rates were low (≤ 2%) for both treatment options, MSA device removal was required in 11/459 (2.4%) patients. Important clinical information for context is that although the study included patients with hiatal hernia > 3 cm (48%) and Barrett’s esophagus (12.7%), these were all in the fundoplication group since the instructions for use valid at the time necessitated exclusion of such patients from MSA treatment [20]. For this reason, the two study groups cannot be considered equivalent.
Walle et al. reported results at a median of 3 years of follow-up after Nissen or partial (Toupet or Dor) fundoplication, with persistent post-operative dysphagia, defined as a GERD-HRQL score > 1 at 1 year or beyond, in one quarter of patients that underwent anti-reflux surgery (i.e., both complete and partial, without a difference between these treatments). Bloating was present in 43.5% after Nissen fundoplication and 37.9% after partial fundoplication, which was moderate/severe in 25.2% of Nissen fundoplication patients and 22.9% of partial fundoplication patients [21]. A randomized controlled trial by Spechler et al. used the same definition of treatment success as used here—a 50% improvement in total GERD-HRQL score—obtaining a 67% success rate at 1 year following LNF. Although this is considerably lower than the 91.5% obtained in the patients in the present study, it should be noted that the participants in the trial by Spechler et al. all had true PPI-refractory GERD [22].
A recent (2024) systematic literature review [13] assessing long-term outcomes of Nissen fundoplication, the current standard-of-care LARS, reported significant rates of odynophagia (16%), dysphagia (29%), gas-bloating syndrome (53%), inability to belch or vomit (40%), heartburn or epigastric/sternal pain (27%), reliance on PPI medication (12%), and re-operation (23%) at 5 years.
Although a naïve-indirect comparison, the results of the RefluxStop CE mark trial show superior outcomes at 3 years. RefluxStop surgery posits a GERD treatment alternative with promising clinical outcomes, in terms of robust and sustained safety and effectiveness results, that indicate favorability over the current standard of care. Additional studies, including real-world data, have been published recently reporting positive outcomes in line with results observed in this study [23, 24]. The data and rapidly growing experience with the RefluxStop procedure also indicate that this novel therapy may have an increasingly important role to play in the treatment of reflux disease.
Strengths and LimitationsThe lack of a control group for comparison is a limitation of this study, although its prospective character and third-party data handling are strengths. We understand that an upcoming randomized controlled trial against standard-of-care therapy (i.e., Nissen fundoplication) is underway. Another limitation of this study is exclusion of patient demographics representative of real-world settings, such as those with concomitant large hiatal hernia and morbid obesity. Duration of follow-up is mid- to long-term. Although larger sample sizes would be preferred, data pertaining to the outcomes of RefluxStop surgery in difficult-to-treat demographics have already been published [23, 24], similarly yielding favorable results. It would be desirable to repeat 24-h pH monitoring in all participants to provide objective data in support of the patient-reported outcomes; however, due the nature of the test, which can be inconvenient for patients, its use must be rationalized to a level that is considered acceptable and it shall be repeated at 5 years as standard. These outcomes will be reported in due course.
Comments (0)