Study population
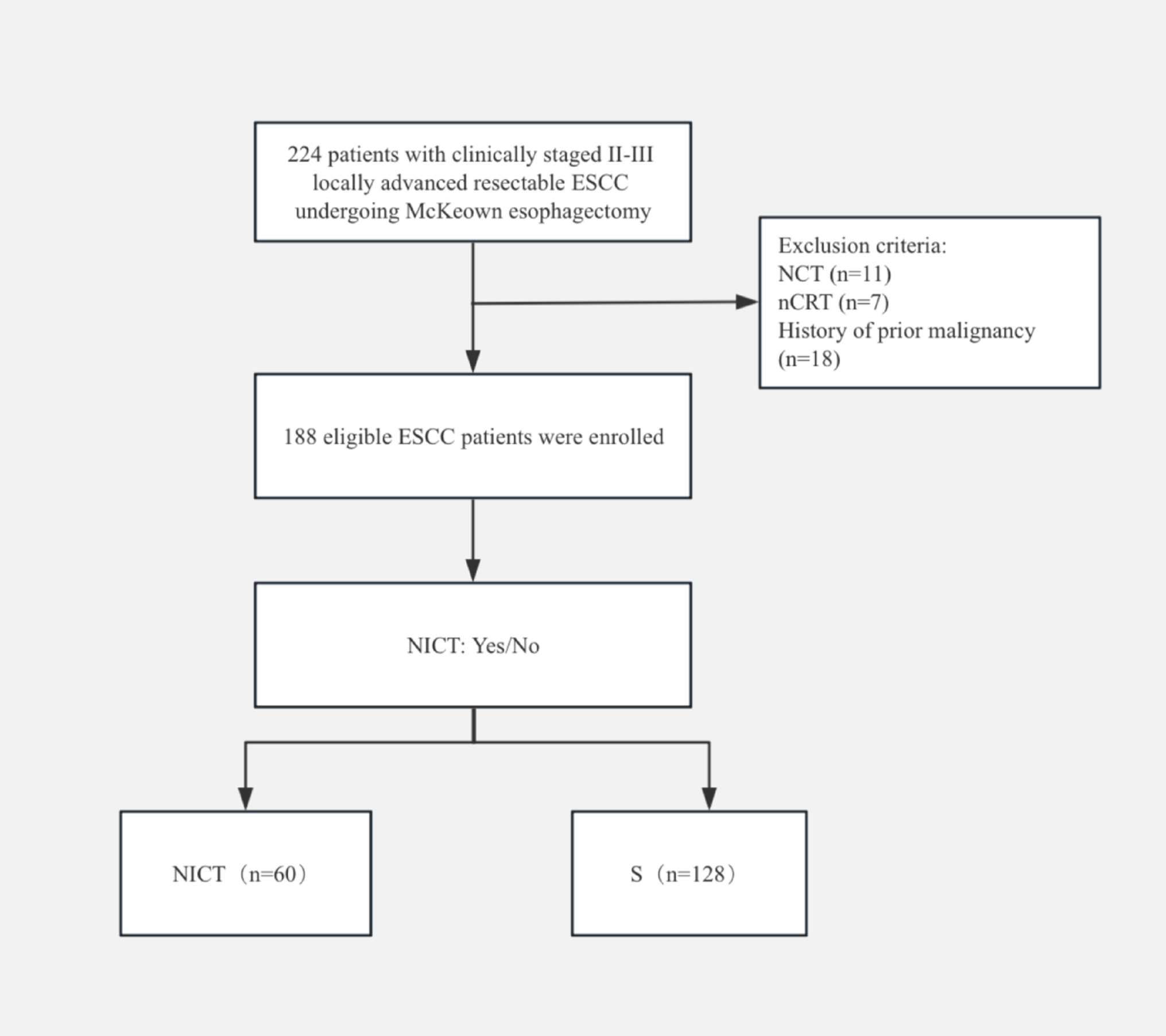
This retrospective study included consecutive patients with histologically confirmed early-stage EC who underwent 192-Ir high-dose-rate (HDR) 3D CT-guided VBT with single-channel cylinders at our institution from January 2019 to January 2024. This study was approved by the institutional review board. All of the patients had received TH/BSO procedures with pelvic ± para-aortic lymph node dissections or pelvic sentinel lymph node biopsies. Patients were staged according to the FIGO-2009 classification and were considered for VBT based on risk factors such as myometrial invasion ≥ 50%, histological grade (G) 2–3, lymphovascular space invasion (LVSI), tumor size > 2 cm, and age > 60 years. The exclusion criteria consisted of patients with positive margins, uterine carcinosarcoma, treated with other applicator types, or loss during follow-up.
Patients were instructed to empty their rectum prior to treatment and the bladder was then filled with 80 ml of saline to decrease the dose to bowels. No bowel or bladder contrast agents were used. CT simulations were performed with a slice thickness of 3 mm or 5 mm. Single-channel cylinder applicators in various diameters (2.0 cm, 2.3 cm, 2.5 cm, 2.6 cm, 3.0 cm, and 3.5 cm) were chosen based on gynecological examinations to ensure the largest tolerable size for the patient. For this analysis, d ≤ 2.6 cm and d ≥ 3.0 cm were defined as the small size and the large size, respectively.
Delineation and 3D planning
The CT-guided 3D volume-based planning was performed in a brachytherapy treatment planning system (B-TPS, Varian Medical Systems, Palo Alto/CA, USA) and delivered using the Varian GammaMed Plus iX HDR afterloader (Varian Medical Systems, Palo Alto, CA, USA). There is no consensus on contouring the vagina as an organ, optimal dose, fractionation schedule, vaginal treatment length, or dose depth for HDR VBT (Small et al. 2012). At our institution, the clinical target volume (CTV) was delineated by uniformly extending 3 mm from the applicator surface (containing the cylinder) for simplicity. This expansion is capable of including 95% of the vaginal lymphatic channels (Choo et al. 2005). The treatment length ranged from 3 to 5 cm from the vaginal apex and did not exceed two-thirds of the total vaginal length in a shortened postoperative vagina. The bladder, rectum, sigmoid, and small intestine were delineated as OARs. The outer borders of hollow organs and bowel loops were contoured. The rectal contour extended from the anal sphincter to the recto-sigmoid flexure. The sigmoid and small intestine were contoured to either the top of the scan or at least 2 cm superior to the vaginal vault. The prescription dose was 5 Gy × 6 fractions, two fractions weekly. After the delineation, the physicist selected the corresponding cylinder models from the TPS applicator library that included all available solid applicator models, followed by applicator reconstruction and dwell position setup. Graphical optimization and manual adjustment were then used to adjust the dwell times to optimize dose distribution. The goal of plan optimization was that 90% of the CTV received the prescribed dose while the minimum dose in the most irradiated 2 cc of the OARs did not exceed 60% of the prescription dose. For larger cylinders, which featured an increased distance between the CTV and the single central axis channel, longer dwell times were required.
A vaginal_CTV structure was retrospectively delineated as a substitute for the vaginal target to assess the dose received by the vaginal wall. The vaginal_CTV was a uniform 3-mm expansion around the applicator surface (excluding the cylinder volume) with a length corresponding to CTV. (Noorian et al. 2023; Carrara et al. 2017).
Dosimetric parameters
The dosimetric parameters were obtained from the dose-volume histogram (DVH) in the B-TPS. The DVH parameters for the vaginal_CTV included: (1) D2, D5, D90, D95, D98, and D100: the minimum doses covering 2%, 5%, 90%, 95%, 98% and 100% of the volume, respectively; (2) D0.1 cc, D1cc, D2cc, and D5cc: the minimum dose in the most irradiated 0.1 cc, 1 cc, 2 cc and 5 cc, respectively; and (3) V100: the volume receiving 100% of the prescribed dose.
Moreover, two quality indices of the vaginal_CTV including conformity index (CI) and homogeneity index (HI) were calculated. The CI is defined as follows (Paddick 2000):
$$\beginc} } \right)^ /(TV \times V_ )} \\ \end$$
(1)
where TV90% is the volume of vaginal_CTV receiving at least 90% of the prescribed dose; TV is the total volume of vaginal_CTV; V90% is the volume receiving at least 90% of the prescribed dose. CI = 1 is the ideal value, indicating better conformal coverage. The HI was calculated using the equation (Prescribing and Therapy 2010):
$$\beginc} - D_ } \right)/D_ } \\ \end$$
(2)
where D50 is the median dose of the volume. Lower HI values represent a more homogeneous dose distribution and HI = 0 is the ideal value.
The D0.1 cc, D1cc, D2cc, and D5cc were evaluated for the OARs. All of the cumulative DVH parameters were calculated by linear equivalent dose in 2 Gy (EQD2) summation from each VBT fraction, and α/β = 3 Gy was assumed for both the vagina and OARs. (Noorian et al. 2023; Rovirosa et al. 2015).
Radiobiological parameters
The equivalent uniform dose (EUD) was assessed to better describe the biological effects of a nonuniform dose distribution (Niemierko 1997) The EUD is defined as the single uniform absorbed dose that produces the same biological effect as an inhomogeneous dose distribution, based on the linear quadratic (LQ) cell survival model for tumors. Later, the concept was extended to normal tissues, and the phenomenological model, known as the generalized equivalent uniform dose (gEUD), was proposed (Niemierko 1999) The gEUD can be calculated as follows: (Gay and Niemierko 2007)
$$\beginc} \left( D_^ } \right)} \right)^ } \\ \end$$
(3)
where vi represents the i’th partial volume receiving dose Di; and a is a unitless model parameter specific to the normal tissue or tumor of interest. EUD integrates voxel-level doses and volume effect, thereby effectively quantifying the biological effects of inhomogeneous dose distribution (Chen et al. 2024). In this study, the EUD was used to correlate doses with clinical outcomes through radiobiological modeling. The aim of this approach was to evaluate whether variations in the dose distribution would have potential clinically significant effects on treatment outcomes.
The selection of the parameter a mimics the dose–response behavior of the volume of interest and determines the behavior of the model (Gay and Niemierko 2007; Oinam et al. 2011). For tumors, the a takes on a large negative value, making the gEUD approach the minimal dose because the tumor control depends on the minimum dose it received. For normal tissue, a is a large positive value for small volume effects (as in serial architectures) and a small positive value for large volume effects (as in parallel architectures). In most current studies, EUD generally refers to gEUD. The parameter a for OAR is from the Lyman model parameter n, which uses the formula a = 1/n (Oinam et al. 2011; Gay and Niemierko 2007; Wu et al. 2002). For the current study, a = 2 for bladder, a = 8.33 for rectum, and a = 3 for vaginal_CTV (Guy et al. 2019).
The imaging, structure, and dose data were exported from the TPS in Digital Imaging and Communication in Medicine files and then processed with the open-source Computational Environment for Radiological Research (CERR) software (The Mathworks, Natwick, MA). EUDs for vaginal_CTV, rectum, and bladder were calculated from DVH, and the cumulative EUD was the sum of each fraction (Nenoff et al. 2021).
Follow-up
All patients were followed for one month after treatment, then every three months for the first two years, every six months for the next three years, and annually thereafter. A physical examination, blood tests, gynecological ultrasound, pelvic CT or MRI, and abdominal CT were performed at each visit for the presence of recurrence and complications. Urinary, gastrointestinal, and vaginal toxicities were assessed using the Common Terminology Criteria for Adverse Events v5.0. Acute toxicity was defined as that appearing within three months after the treatment.
Statistical analysis
Propensity score matching (PSM) was performed to reduce selection bias. Matching covariates included age, height, BMI, treatment length, stage (FIGO 2009), histological grade, hypertension, diabetes, hyperlipidemia, and adjuvant chemotherapy. Missing data were imputed using the k-nearest neighbor method with k = 10. Genetic matching was performed using the MatchIt package in R with a 1:2 ratio of small-size to large-size groups and a caliper width of 0.1 times the standard deviation of the propensity score.
The normality of the continuous variable distributions was tested using the Shapiro–Wilk test. Categorical variables were evaluated using Pearson’s chi-square test or Fisher’s exact test, and continuous variables were assessed using Student’s t-test or Mann Whitney test. A two-sided p-value < 0.05 was considered statistically significant. All the analyses were conducted using R version 4.3.2 (R Foundation).





Comments (0)