
Remember me




Early diagnosis and treatment of overweight and obesity can improve overall health and quality of life as well as prevent and manage obesity-related complications [1]. However, healthcare professionals should be aware that people living with obesity may have experienced bias, stigma, and discrimination because of their weight or obesity in many settings, including healthcare settings [49]. These experiences may affect patients’ willingness to interact with healthcare professionals. Patients who have experienced weight bias and stigma may delay or avoid healthcare services for fear of being blamed and shamed for their weight. Therefore, obesity screening, assessment, diagnosis, treatment, and management need to be conducted using objective medical measures and non-judgmental, collaborative, and person-centered approaches. Collaborative conversations, based on motivational interviewing, can include strategies such as: i) asking for permission to initiate a conversation about weight and obesity (“Is it okay for us to talk about your weight?”, “What worries you about your weight?”, “How can we work together to manage your obesity?”); ii) avoiding making assumptions about patients’ lifestyles, health behaviours, interests, motivations, or stage of change; iii) listening to patients’ concerns and trying to understand patients’ points of view; iv) validating and respecting patients’ situations and experiences; v) supporting patients to make choices, adapt, and sustain evidence-based behaviors associated with obesity management; vi) exchanging ideas about alternative options to address obesity management barriers; vii) establishing an action plan together; and viii) acknowledging that behavior change is difficult while recognizing small changes [50].
Obesity is an adiposity-based chronic disease and the goal of a medical obesity assessment is to determine how excess or dysfunctional adiposity impacts a person’s health and well-being. Anthropometric measures, such as BMI or waist circumference, can be used as screening tools, but relying solely on anthropometric measures for the screening and diagnosis of obesity can lead to both underdiagnosis and overdiagnosis of obesity [13, 51]. To diagnose obesity, existing international guidelines recommend a full medical assessment to determine if and how excess adiposity or pathogenic changes in adipose tissue are impacting a person’s health and well-being [5, 8, 13, 33, 51, 52]. A medical obesity assessment can consider the impact of obesity on cardiometabolic health, physical functioning, and psychosocial outcomes [5, 8, 13]. With a more accurate diagnosis and staging of obesity and its complications, healthcare professionals can work collaboratively with patients living with obesity to develop personalized, targeted, and effective obesity treatment and management approaches [52]. Accurate diagnosis of obesity can also facilitate the allocation of healthcare resources so that patients who need treatment have access to effective and evidence-based treatments.
Cardiovascular diseases are among the most significant obesity-related impacts and the leading cause of mortality worldwide [53]. A staggering 17.7 million deaths in 2015 were due to cardiovascular diseases, accounting for 31% of global mortality. Research indicates that dysfunctional adipose tissue and abnormal fat deposits in the myocardium and epicardium lead to the release of a series of metabolic signals, reactive oxygen species, prothrombotic, pro-inflammatory, and neurohormonal factors, resulting in endothelial dysfunction [53, 54]. Conducting a cardiovascular risk assessment in patients living with obesity is critically important and can inform effective clinical decision-making. Patients who have a low cardiovascular risk assessment score can receive secondary prevention recommendations, while patients with a high cardiovascular risk score should receive evidence-based obesity and cardiovascular treatments. Several scales and predictive models are available to assess cardiovascular risk in primary healthcare. However, there is some uncertainty regarding the potential impact on health outcomes and therapeutic approaches when using cardiovascular risk scales in adults with overweight or obesity within primary care settings.
In women of reproductive age who wish to get pregnant, multidisciplinary obesity treatment before and during pregnancy have been demonstrated to have some benefit for both the mother and the offspring. There is some evidence that multidisciplinary lifestyle-based programs can also enhance certain fertility, maternal, and child health outcomes, compared to conventional treatment [55].
This guideline includes evidence-based recommendations (Table 3) and consensus-based good practice statements (Table 4) for clinical evaluation.
Table 3 Recommendations: Clinical Evaluation*Table 4 Good Practice Statements (Ungraded): Clinical Evaluation*Obesity TreatmentsEffective and evidence-based obesity treatment interventions include behavioral interventions and psychological therapy, pharmacotherapy, and bariatric surgery and endoscopic procedures in conjunction with medical nutrition therapy and physical activity interventions [8]. Unfortunately, as in many countries, Mexican adults living with obesity often lack access to effective, evidence-based treatments and long-term management support [36].
Global obesity clinical guidelines widely accept that creating individualized care plans (based on key principles of chronic disease management) that target the root causes and complications of obesity, delivered where possible by a multidisciplinary care team with expertise in each treatment approach, and working towards improvements in health and well-being (not solely weight loss) and treatment goals identified in collaboration with patients, may represent the highest standard of obesity care [13, 57].
Multidisciplinary management approaches may improve obesity outcomes (e.g., weight loss, weight loss maintenance, quality of life, etc.) and management of obesity-related complications [58].
Medical Nutrition TherapyMedical nutrition therapy is a central component of obesity treatment, along with other critical elements, such as physical activity, exercise, sleep, and stress management. The consequences of a diet high in energy (calories) can negatively affect health in various ways, including problems related to gastrointestinal function (e.g., constipation, diarrhea, reflux, acid peptic disorders, etc.) and metabolic imbalance (e.g., hypertension, metabolic dysfunction-associated steatotic liver disease, overweight, obesity, prediabetes, diabetes, dyslipidemia).
To ensure a safe, effective, culturally acceptable and sustainable approach it is critical to provide personalized nutritional recommendations for adults with overweight or obesity based on their personal characteristics, history, values, preferences, and treatment goals [59]. Medical nutrition therapy should ideally be provided by a certified nutritionist experienced in managing obesity who can provide evidence-based advice to maximize outcomes [59].
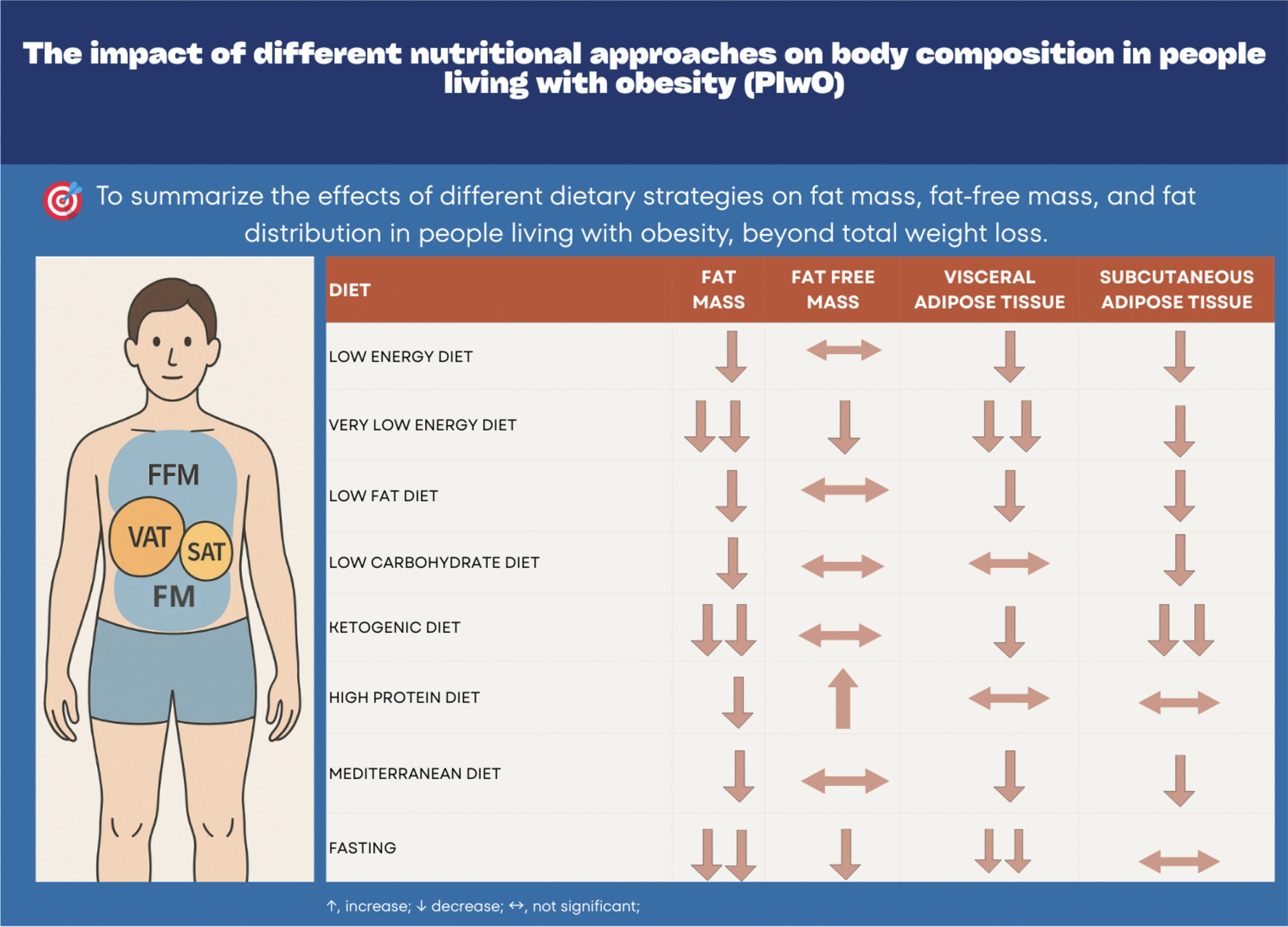
A dietary plan should be low in energy to effectively treat obesity and achieve improved weight or BMI outcomes. Numerous studies have assessed various nutritional approaches for treating obesity, examining the wide variability in the composition of fat, protein, and carbohydrates, as well as varying levels of energy restriction and time restriction, among dietary approaches. These studies demonstrate that the effectiveness of different types of diet is variable in terms of achieved weight loss and metabolic benefit [60,61,62]. However, it is difficult to compare diets due to methodological and/or analytical differences, degrees of caloric restriction, degrees of adherence, measurement errors, confounding variables, and other factors [63].
Systematic reviews and meta-analyses of clinical trials related to dietary interventions for overweight and obesity, usually show diverse results, although these differences are minor [64,65,66,67]. This leads to the conclusion that the effects of these interventions in the medium and long term do not justify the prescription of one diet over another. Currently, no single diet has been proven to be superior in treating people with obesity.
Thus, adults living with overweight or obesity can consider any of the multiple medical nutrition therapies with scientific evidence to improve health-related outcomes, choosing food-based dietary patterns that allow for best long-term adherence [59]. It is important to clarify that, once this dietary plan is identified, it will not necessarily remain optimal throughout the patient's treatment since results may vary and personal circumstances may change. Therefore, health professionals and patients must be flexible and adapt the treatment according to the results of the periodic evaluations carried out during follow-up.
Physical ActivityAccumulated time spent engaging in sedentary behaviors – defined as any activity of an awake individual, lying or reclining, that has an energy expenditure of less than 1.5 metabolic units [68]– increases the risk of morbidity and mortality due to cardiovascular and metabolic causes. It also has a negative impact on musculoskeletal and psychological health, independent of other lifestyle factors [69,70,71].
Active breaks are a simple strategy to improve cardiovascular and metabolic health and help offset the physiological effects of sedentary behaviors. Given the ease of accessibility and performance of these simple activities, they can serve as an introduction to physical activity as a treatment tool for patients with chronic diseases [69,70,71,72]. These breaks do not require specialized sports equipment or specific intensity targets, and can involve simple activities such as walking at any speed, tiptoe rising, doing squats, etc. There is no consensus on the number of active breaks needed throughout the day.
Most people do not reach the minimum exercise recommendations suggested by the WHO to maintain health [73,74,75,76,77], with a lack of time commonly reported as a primary barrier. The concept of “exercise snacks” has therefore emerged as an option for individuals with limited time and for those whose work activity is predominantly sedentary [78, 79]. This approach centers on short bursts of exercise multiple times throughout the day involving moderate to vigorous intensity with a duration of less than one minute, spaced at intervals between one to four hours [80, 81]. Exercise snacks can be done with rhythmic, repetitive exercises that involve long muscles, such as climbing stairs, jumping jacks, and cycling, among others, or with strength exercises, such as squats, rowing, planks, etc., depending on specific objectives, health status, and level of physical fitness [82,83,84,85]. Performing exercise snacks with a minimum frequency of three or more episodes during the day improves various aspects of health: cardiorespiratory capacity [86, 87], muscle strength [84, 88,89,90,91], and cardiometabolic health [82, 92,93,94]
This guideline includes evidence-based recommendations (Table 5) and consensus-based good practice statements (Table 6) for medical nutrition therapy and physical activity interventions.
Table 5 Recommendations: Medical Nutrition Therapy and Physical Activity*Table 6 Good Practice Statements (Ungraded): Medical Nutrition Therapy and Physical Activity*Behavioral and Mental Health InterventionsThere is a complex and bidirectional relationship between obesity and mental health [95, 96]. It has been documented that people living with obesity have a higher prevalence of depression, anxiety, and stress. Depressive symptoms, anxiety, and stress can also drive to alterations in eating behaviors [96], which, combined with other factors (e.g., genetic, environmental, and biological), can lead to the development of obesity. Other factors that affect both mental illness and obesity include inflammation, maladaptive coping mechanisms, and sociodemographic factors [97].
There is thus a need to consistently assess psychological and behavioral factors both at the onset and throughout the implementation of any obesity treatment. This is because psychological distress may also stem from deteriorating health, social stigma, and discrimination experienced by individuals living with obesity [98, 99].
Understanding patients’ personal history and trajectory of obesity development is crucial. This involves knowing when the weight gain began, what caused it, previous treatments, situations that led to weight changes, the impact on quality of life, and how the weight gaining pattern has evolved over time. A deeper understanding of each patient allows clinicians to create a personalized treatment plan [100].
In traditional obesity treatment paradigms, there has been an implicit assumption that obesity results from a lack of self-control (overeating), and that people can lose weight and keep it off simply by changing their eating “habits”[101]. However, we now recognize the strong genetic influences on body weight and the complex neuroendocrine regulation of energy intake and expenditure, which often hinder long-term weight management efforts.
Psychological and behavioral interventions are integrated as key pillars of obesity management [5, 8, 33]. These interventions will not only support health behavior interventions (e.g., medical nutrition therapy and physical activity) and health behavior changes (e.g., medication adherence, self-care strategies), but they will also generate a deeper understanding of the underlying reasons and conditions behind these behaviors. This includes considering thoughts, emotions, attitudes, stages of change, motivation, expectations, barriers, and potential solutions.
Behavioral and psychological interventions can be used to educate patients that weight control is neither easy nor always comfortable, and to help them develop skills to achieve behavioral change that will allow them to have a healthier life, reduce stress, have better tools to face their environment, increase psychological flexibility, promote acceptance of internal experiences, tolerate frustration, improve their quality of life, and promote sustainable self-care in the short and long term [102, 103]. Effective and collaborative conversations with patients using motivational interviewing strategies support changes toward a health behavior change, which is essential for living with and managing chronic diseases, including obesity [50].
These psychological interventions, when used in conjunction with the rest of the obesity management strategies, move from simply inducing weight loss (through caloric restriction) to facilitating patients to adopt patterns of eating and physical activity and medical adherence that promote optimal changes in body composition and overall health [102, 103].
This guideline includes evidence-based recommendations (Table 7) and consensus-based good practice statements (Table 8) for behavioral and mental health interventions.
Table 7 Recommendations: Behavioral and Mental Health Interventions*Table 8 Good Practice Statements (Ungraded): Behavioral and Mental Health Interventions*PharmacotherapyThere is a widespread belief among both patients, health professionals, and healthcare policymakers that a lack of adherence to lifestyle changes is the main barrier to managing overweight and obesity [36]. However, in many cases, medical nutrition therapy and physical activity interventions on their own do not achieve long-term sustainable improvements in overweight and obesity (which, it is important to stress, may or may not involve weight loss) given the multifactorial etiology and heterogeneity of the disease. Multiple interventions, including medical nutrition therapy, physical activity, psychotherapy, pharmacotherapy, and bariatric surgery, may be necessary to address the complex physiological mechanisms of weight gain and improve health outcomes [104]. Thus, pharmacological treatments are recommended for patients undergoing behavioral interventions who have a BMI ≥ 30 kg/m2 or for patients with a BMI ≥ 27 kg/m2 with at least one comorbidity associated with excess adiposity [105]. Despite eligibility and safety of current obesity medications, there are many access barriers to these treatments, and less than 2.0% of patients living with obesity receive pharmacological treatment [106].
Multiple pharmacological agents have emerged with potential utility for the treatment of overweight and obesity. Safe and effective long-term medications are available in Mexico that can achieve a reduction of 5%–14% of total body weight (semaglutide, liraglutide, combination of naltrexone with bupropion, and orlistat). In addition, these treatments may offer benefits in terms of improvement in obesity-related complications and comorbidities independent of weight loss [105].
Pharmacotherapy should be individualized based on patients’ specific conditions, obesity complications, and comorbidities, as well as safety considerations specified in Fig. 1. All approved medications for treating obesity are contraindicated during pregnancy. Following obesity treatment, there is an increased likelihood of pregnancy, necessitating careful monitoring and guidance for women of childbearing age.
Fig. 1
Individualization of Long-Term Pharmacotherapy Using Agents Approved in Mexico. Abbreviations: T.i.d. = three times a day, B.i.d. = two times a day, Q.d. = once a day, MAFLD = metabolic dysfunction-associated steatotic liver disease, CAD = cardiovascular arterial disease, CKD = chronic kidney disease, mild (50–79 mL/min), moderate (30–49 mL/min), RD = retinopathy-diabetic, SBP = surveillance blood pressure, UH = uncontrolled hypertension, MHR = monitor heart rate, AD = adjusted doses, APOS = avoid previous oxalate stones, MS = monitor symptoms, APD = avoid if prior disease, A = avoid, CR = controversial results, LSU = lower seizure umbral, AO = antagonize opioids, ARD = avoid if prior RD, MTAC = may trigger angle closure
It is important to note that in Mexico, some obesity medications are still prescribed despite lacking robust scientific evidence for their long-term efficacy and safety. Therefore, it is crucial for healthcare professionals who are the first point of contact for patients living with obesity and who wish to prescribe pharmacological interventions to carefully consider an agent’s effectiveness and safety.
This guideline includes evidence-based recommendations (Table 9) and consensus-based good practice statements (Table 10) for pharmacotherapy interventions.
Table 9 Recommendations: Pharmacotherapy*Table 10 Good Practice Statements (Ungraded): Pharmacotherapy*Metabolic and Bariatric SurgeryMetabolic and bariatric surgery (MBS) is one of the key pillars of obesity treatments and should be considered for individuals living with obesity, severe obesity, and obesity-related complications. MBS, encompassing procedures such as gastric bypass and sleeve gastrectomy, plays a crucial role in the treatment of severe obesity [5, 8,
Comments (0)