Our pooled analysis of seven country-specific RWE studies assessing the use of oral semaglutide in adults with T2D shows that clinically relevant reductions in HbA1C and body weight are seen regardless of baseline HbA1C, body weight, age, or T2D duration. Moreover, outcomes are similar for participants treated by either primary care physicians or specialists. Even though treatment satisfaction among participants was high at study start, it significantly increased during the study.
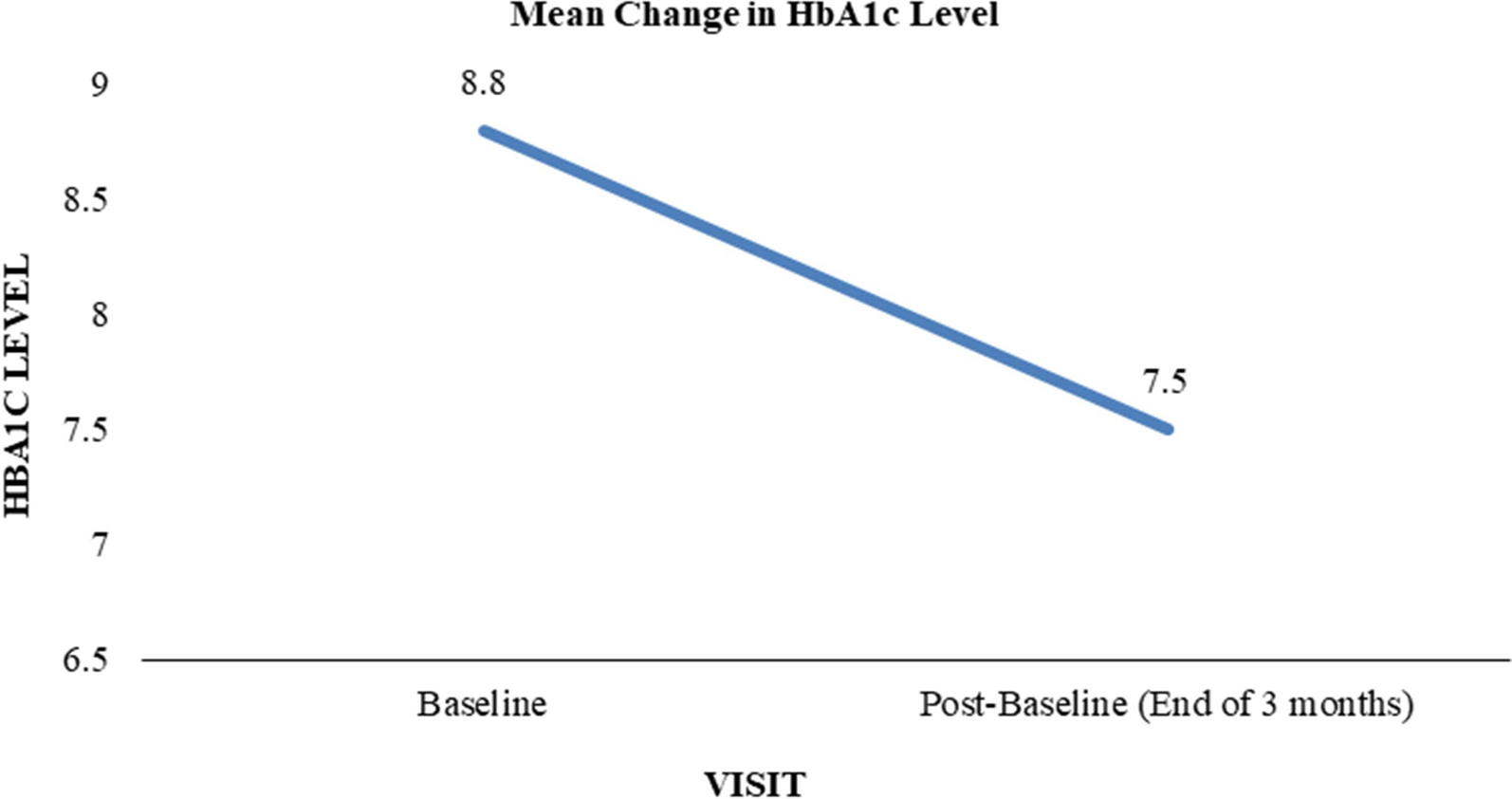
Generally, glycemic control in participants receiving oral semaglutide treatment was similar across the seven country-specific studies, estimated mean HbA1C change ranging from − 0.9%-point in Sweden (− 9.6 mmol/mol) [20], Denmark (unpublished) (− 9.9 mmol/mol), Switzerland (− 9.9 mmol/mol) [21], and Italy (− 10.0 mmol/mol) to − 1.2%-point (− 12.7 mmol/mol) in the Netherlands [19]. The pooled estimated change in HbA1C from baseline to week 38 was − 1.0%-point (− 11.2 mmol/mol). The estimated change in body weight of − 4.9 kg (− 5.0%) reflects the corresponding results in individual countries, except for Canada, where the estimated body weight change was − 7.19 kg (− 7.17%) [18]. A USA-based retrospective observational cohort study (IGNITE) has also studied oral semaglutide use in adults with T2D in clinical practice [28]. In the IGNITE population, a 0.9%-point (approximately 10 mmol/mol) reduction in HbA1C was observed for the full study cohort after 5.7 months of treatment while the reduction was 1.0%-point (approximately 11 mmol/mol) in GLP-1RA-naïve individuals.
We also explored the relationship between improvement in glycemic control and body weight changes during oral semaglutide treatment. Similar investigations have been performed for subcutaneous treatment with tirzepatide, a combined glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 receptor agonist [29], as well as for the GLP-1RAs liraglutide, exenatide, dulaglutide, and semaglutide [30,31,32,33,34]. These analyses generally showed that greater HbA1C reductions correlated with greater weight loss, albeit weakly. In this PIONEER REAL pooled study, a similar correlation between HbA1C change and body weight change was observed.
Comparing results between country-specific PIONEER REAL studies should be done with caution, as results are based on real-world settings that vary in characteristics (e.g., different baseline HbA1C or T2D duration). Combining results from the seven individual studies into a statistically powerful dataset, on the other hand, allows an attempt to extract information that is both highly relevant and widely applicable. That is what we have sought to take advantage of in this pooled analysis. Our results show that participants receiving oral semaglutide treatment experience improved HbA1C levels across age groups from under 50-year-old to over 75-year-old in a real-world setting. This is in line with other studies where other GLP-1RAs, liraglutide and dulaglutide, have proven to be effective in the treatment of T2D across various age groups [32, 35,36,37]. Clinical studies, such as the PIONEER program for oral semaglutide, have demonstrated robust glucose-lowering and weight reduction effects in diverse age demographics [6].
When changes in HbA1C levels were stratified by baseline diabetes duration, pooled results showed a reduction across all intervals, in line with the clinical PIONEER program [38]. Reduction in HbA1C levels in the current study was more than twice as high in participants having lived with diabetes for less than a year compared to participants with a diabetes duration of more than 5 years. A similar albeit weaker trend was seen when stratifying body weight change by baseline diabetes duration; participants with a shorter duration of T2D often experienced more substantial reductions in body weight compared to those with a longer disease duration. These findings suggest that improvements seen in glycemic control and weight management may be more pronounced in participants with a shorter T2D duration, which may help in motivating affected individuals to an early and adequate intervention. It is important to note that participants receiving oral semaglutide treatment experienced improvements in glycemic control and weight management regardless of T2D duration.
A major objective for the PIONEER REAL pooled study was to investigate if the participants’ physician setting (specialist or primary care) played a role in the estimated HbA1C change from baseline to EOS. No difference in HbA1C reduction was observed, regardless of the physician being a specialist or a primary care practitioner. The numbers of participants prescribed oral semaglutide by a primary care practitioner or specialist were very similar in this dataset (876 and 739, respectively). This distribution is unusual for a relatively newly available antidiabetic drug, which would typically be favored by specialists. A partial explanation for this could be that primary care practitioners are less hesitant to prescribe oral semaglutide owing to ease of administration and, in some cases, higher adherence to an oral option compared to injections [13]. It should be noted that the selected study sites for the individual PIONEER REAL studies may limit interpretability of this result.
Treatment satisfaction among individuals with T2D is a multifaceted concept that encompasses various dimensions such as glycemic control, weight management, ease of use, side effects, and overall quality of life. Treatment satisfaction among participants, as assessed by both DTSQs and DTSQc [23, 24], was generally high at baseline across the seven pooled countries, but treatment with oral semaglutide significantly increased both DTSQs and DTSQc scores at the EOS: estimated mean DTSQs increased by 3.5 points and the estimated mean DTSQc score was 12.2. This indicates that participants highly valued the treatment with oral semaglutide, even if their level of satisfaction was already good at baseline. The observed improvement in treatment satisfaction is important as it may enhance participants’ self-efficacy and adherence to therapy, leading to long-term stable glycemic control and reduced risk of complications [39]. No new safety concerns were observed in the seven completed studies of the PIONEER REAL program.
Typical limitations for a real-world study also apply for the individual PIONEER REAL studies, where limitations are described in more detail [18,19,20,21,22]. Briefly, the studies were purely observational and designed without a comparator arm. As data were collected as part of routine clinical practice, the robustness and completeness of the data and conclusions may be affected. Finally, the studies were conducted during the COVID-19 pandemic, leading to several participants not completing their EOS assessment in the predefined timeframe.

Comments (0)