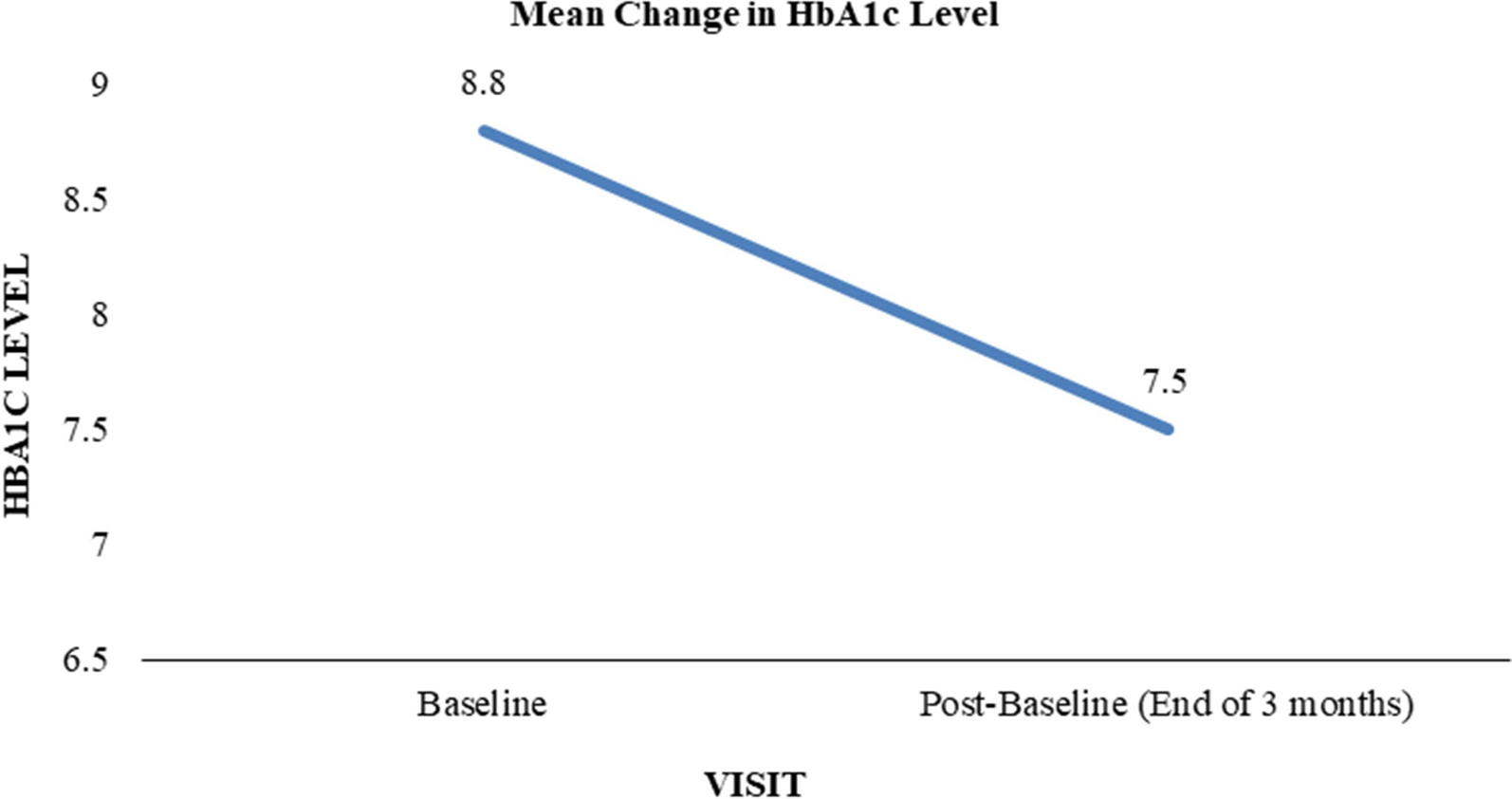
In this study, we report the following findings: (1) transition from premixed insulin to IDegAsp resulted in substantially decreased levels of HbA1c, FBG, and PBG in patients with T2DM; (2) the total daily dose of IDegAsp was significantly lower than that of premixed insulin; (3) age and disease duration did not affect IDegAsp effects on HbA1c reduction; and (4) patients with prior low-mix insulin took a significantly lower dose of insulin degludec while patients with prior mid-mix insulin took a markedly higher dose of insulin degludec than their respective intermediate-acting insulin doses.
IDegAsp is superior to premixed insulin in glycemic control [9,10,11,12,13]. We demonstrated that switching from premixed insulin (low-mix and mid-mix as well) to IDegAsp led to significantly lower HbA1c, FBG, and PBG levels, supporting previous findings [9,10,11,12,13]. In the present study, we were unable to evaluate the effect of IDegAsp on hypoglycemia due to incomplete data. Other studies have revealed that patients with type 2 diabetes have fewer hypoglycemia episodes after switching from premixed insulin to IDegAsp [9, 10, 12].
Several studies have looked into the change in total daily insulin dose after the transition to IDegAsp from premixed insulin in patients with T2DM with discordant reports [9,10,11,12,13, 17]. Kang et al. revealed no significant differences in total daily insulin dose before vs. after switching [11]. In contrast, in a real-world, prospective, non-interventional study, Fulcher et al. found that the total daily insulin dose was significantly reduced in adults with T2DM after switching to IDegAsp from premixed insulin [9]. A retrospective cohort study also showed decreased the total daily insulin dose in patients with T2DM after switching to IDegAsp from premixed insulin [10]. Such a finding has been documented by other groups [12, 13]. Taken together, the majority of literature data along with ours demonstrated that switching to IDegAsp from premixed insulin decreased total daily insulin dose. In the present study, we also observed a reduction in insulin injection frequency in a significant number of patients after switching, in agreement with the data reported in a recent study [13].
Blood glucose control in elderly patients with T2DM with long disease durations has always been a clinical challenge. In view of cognitive ability decline, comorbidities, polypharmacy, and high risk of hypoglycemia in elderly patients, the Chinese guidelines for the management of diabetes mellitus recommend the “simple treatment concept” and “de-intensified treatment strategy” for this specific group of patients [18]. In the present study, we discovered that age and disease duration did not affect IDegAsp effects on HbA1c reduction. Therefore, IDegAsp, which has a high safety profile and a low risk of hypoglycemia, appears to be more suitable for elderly patients with diabetes who are particularly prone to hypoglycemia [19].
Although IDegAsp shows advantages over other insulin formulations, there are no guidelines on IDegAsp dose to be used after transitioning from premixed insulin [14]. It is suggested that IDegAsp should usually be started at the same unit dose and injection frequency as the premixed insulin according to limited clinical experience or at a dose according to clinician discretion [20]. Data on the dose of insulin degludec used in the real world after switching are lacking. In the present study, we compared basal insulin doses in patients with T2DM after switching from premixed insulin to IDegAsp and revealed some novel findings: the total daily dose of insulin degludec at both 3 and 6 months after switching was significantly lower than that of intermediate-acting insulin taken by low-ratio premixed insulin users; conversely, the total daily dose of insulin degludec at both 3 and 6 months after switching was significantly higher than that of intermediate-acting insulin taken by mid-ratio premixed insulin users. To our knowledge, this is the first description of insulin degludec dose relevant to that of basal insulin in premixed formulations. This data provided a valuable reference for adjusting insulin degludec dose when switching from premixed insulin to IDegAsp.
This study had some limitations. First, the number of patients was small, limiting the analyses of other parameters, such as the use of other types of hypoglycemic medications. Second, as a single-arm, single-center study, there was a potential for selection bias. Last, changes in body weight and hypoglycemia risk were not analyzed due to incomplete data. Multicenter, prospective, real-world studies should be conducted in the future to validate our findings.

Comments (0)