
Remember me
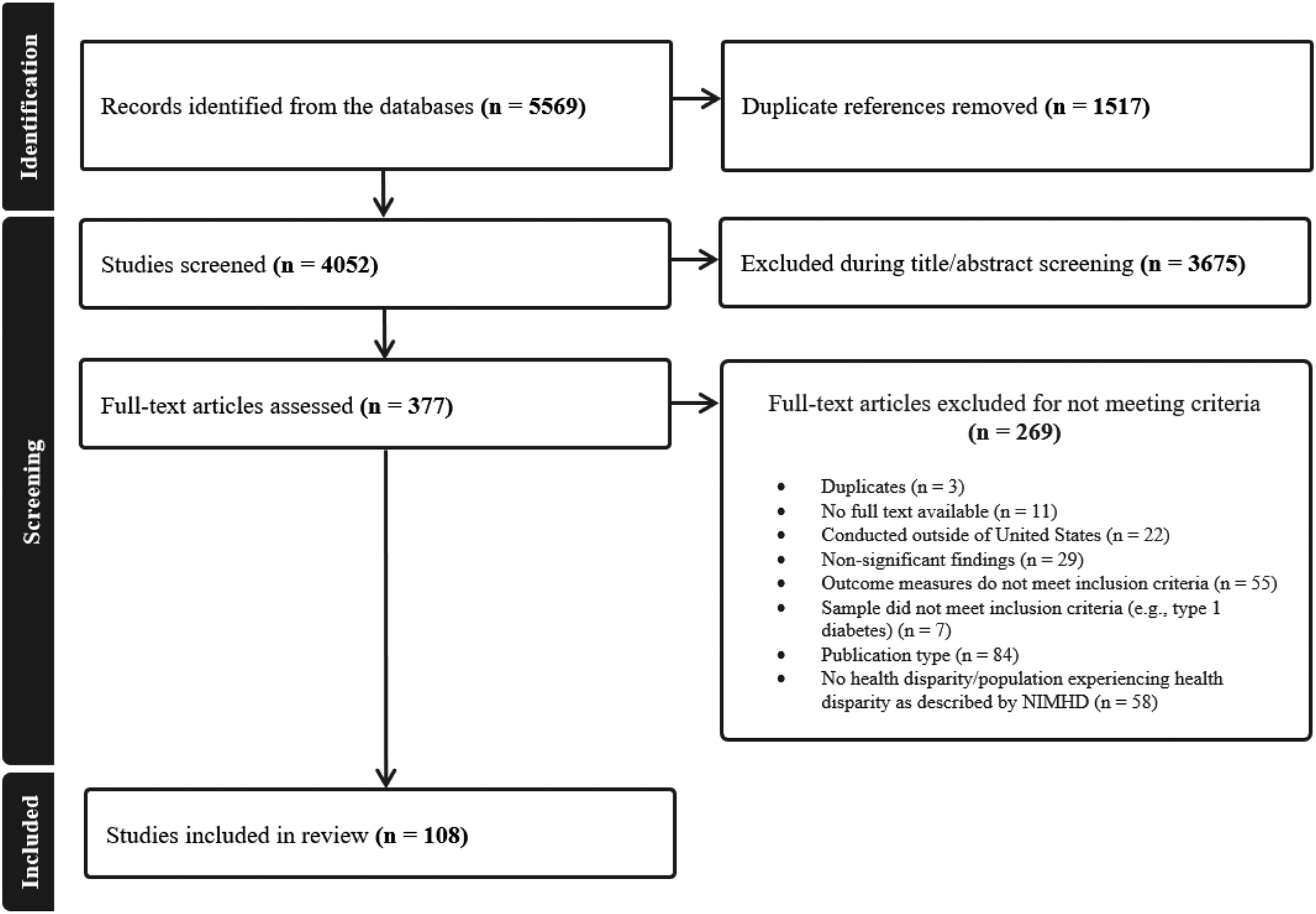
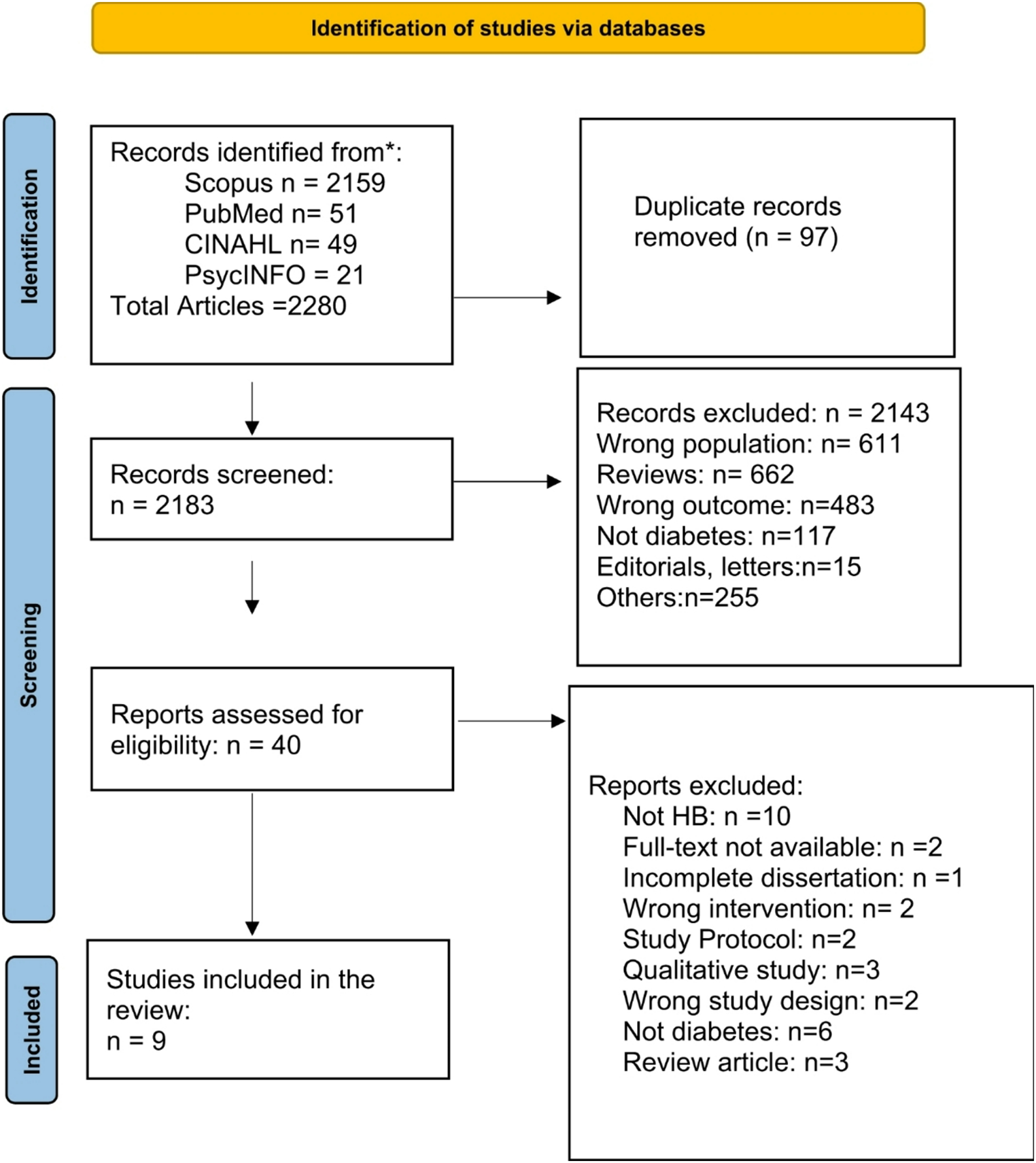
Following removal of duplicate papers, 156 studies were identified in the initial search, 62 reached full-text review, and 23 were included in analyses (see Fig. 1). Of the 23 included papers, 19 (82.6%) were published between 2017 and 2023 and 21 (91.3%) focused on T1D. Many of the studies were conducted in the United States (n = 10) or the United Kingdom (n = 3) or were conducted using the international SWEET registry (n = 3). Fifteen studies reported extramural funding, with the most common funding sources being the National Institutes of Health (n = 5), the National Institute for Health and Care Research (n = 3), and SWEET (n = 3).
Most studies involved medical EBPs (n = 12; see Table 1), whereas fewer focused on psychosocial (n = 7; see Table 2) and diabetes education (n = 2; see Table 1) EBPs [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. Two studies considered interventions to support the transition from pediatric to adult diabetes care (see Table 2). Most studies (n = 11) identified barriers and facilitators of implementing an EBP or were implementation trials (n = 11); fewer studies documented gaps in the use of an EBP in standard clinical practice (n = 7). Only one paper detailed the development of an implementation strategy. Five papers employed implementation science theories/models/frameworks. While 13 of the 23 papers mentioned equity, most did so as part of a discussion of their data or next steps for research (n = 11), whereas few papers reported aims to improve equitable access to care or health outcomes (n = 2).
Fig. 1 Table 1 Medical care and diabetes education implementation studies in pediatric diabetesTable 2 Implementation papers on psychosocial care for pediatric diabetes and transition to adult careMedical Care for Pediatric DiabetesEvidence-Based Practices
Table 1 Medical care and diabetes education implementation studies in pediatric diabetesTable 2 Implementation papers on psychosocial care for pediatric diabetes and transition to adult careMedical Care for Pediatric DiabetesEvidence-Based PracticesAmong medical care studies, there was a relatively even split across screening or assessment (n = 6) and treatment (n = 7) EBPs. Screening studies included screening for diabetes complications (including microalbuminuria and ophthalmic issues), monogenic diabetes, T2D, and implementation of ISPAD medical care guidelines. Studies examining implementation of EBPs for pediatric diabetes treatment included in-hospital management of diabetes ketoacidosis (DKA), group-based medical care, and guidance on physical activity. Two studies examined school-based diabetes medical care, one of which examined use of advanced diabetes technologies (i.e., insulin pumps, continuous glucose monitors, hybrid-closed loop insulin infusion systems) in schools.
Areas of Implementation ResearchOnly 3 studies documented research-to-practice gaps, two of which employed the Better Control in Pediatric and Adolescent Diabetes: Working to Create Centers of Reference (SWEET) international registry. First, one SWEET registry study examined use of diabetes technology (insulin pumps, continuous glucose monitors) across 101 SWEET centers, showing that > 60% of the 25,654 pediatric T1D patients used at least one technological component for diabetes management [33]. Second, in a survey study of 105 SWEET diabetes centers, 79 clinics reported on access to antibodies testing (84%), C-peptide determination (73%), and genetic testing (57%). In addition, inequities in access to antibody testing across higher and lower income countries were related to clinical outcomes [37]. Third, in an online survey study of 77 pediatric diabetes units in England and Wales (2019–2020), healthcare providers (N = 114) reported that their role includes supporting (94%) and promoting (88%) physical activity in their patients, consistent with NICE guidance [35].
Four studies identified barriers and facilitators of implementing an EBP. Results from a survey study in England and Wales (described above) indicated that barriers to implementing an EBP around physical activity guidance largely focused on provider factors, such as lack of time, minimal knowledge about the EBP, and limited training opportunities [35]. Two qualitative school-based studies identified barriers of implementing diabetes care and use of advanced technology in that setting [27, 39]. Both studies included small samples of public school nurses (11 to 40) who either identified as White or served largely White students. Multilevel barriers included parental expectations, inconsistent training on use of technologies, interpersonal communication and cooperation, school organizational factors, and local and school policies. A fourth study employed qualitative interviews with medical staff to identify barriers to screening for T2D in a remote town in the Kimberley region of Australia [38]. Barriers included the complexity of the screening guideline, provider apprehension about screening in young adolescents, and organizational issues (e.g., use of automated recall system to achieve patient follow-up, limited time, high use of locum staff).
Only one study described the development process for an implementation strategy, specifically a group-based delivery method for evidence-based pediatric diabetes care [44]. These authors did not identify this delivery method as an implementation strategy. This mixed methods study involved development and refinement of the group-based medical care model at two implementation sites in the United Kingdom serving 78–80% adolescent and young adult patients who identify as ethnic minorities.
Seven studies involved implementation trials. Nearly half of the implementation trials occurred at single clinics (n = 3) and half were multisite trials (n = 4) that ranged from 2 to 25 sites (one study not specifying the number of sites). Although no study used the term implementation strategy, three examined locally developed clinical practice guidelines or screening algorithms as strategies to increase use of an EBP [27, 38, 42]. Two studies described testing technology-based implementation strategies, such as a point-of-care decision aid (iSCREEN) and an artificial intelligence-based approach to ophthalmic exams [48, 49]. In one trial aimed at increasing delivery of evidence-based pediatric diabetes care, an implementation strategy of anonymous comparison on quality indicators among a nationwide system of 25 treatments centers was evaluated [40]. While no studies employed Proctor’s implementation outcomes explicitly, six studies described adoption as the primary or sole implementation outcome and one study did not report an implementation outcome. For example, in a prospective study evaluating the use of artificial intelligence to ophthalmic exams at one clinic (310 pediatric patients, 57% White, 32% Black, 47% male) led to a pre-post increase from 49 to 95% in exam completion and adherence to guidelines [48]. Two studies measured both effectiveness and implementation outcomes (i.e., hybrid studies) [40, 48]. None of the trials included a comparison implementation strategy or set of strategies and the descriptions of implementation strategies being tested were minimal. Rather, pre- and post-implementation data were typically compared (n = 6).
Models/Theories/Frameworks and TerminologyTaken together, most studies did not employ implementation science terminology, reporting standards, or models, theories, and frameworks. No studies employed the terminology “implementation strategies” and only 3 studies used implementation science models/theories/frameworks, namely complexity theory, ADAPTE, and the Capability, Opportunity, and Motivation Model for Behavior (COM-B) [27, 35, 44, 50,51,52].
Consideration of EquityOf the 12 medical studies, 7 at least noted issues of equity related to the EBP of interest in the discussion of findings or areas for future research. Only 2 studies aimed to improve equity. One of these studies focused on a group-based implementation strategy to increase the reach of evidence-based medical care among young people with diabetes in “ethnically diverse, and socio-economically deprived settings” [44]. The second study involved a trial to improve screening for T2D among underserved Aboriginal and/or Torres Strait Islander youth [38].
Psychosocial Care for Pediatric DiabetesEvidence-Based PracticesAll seven psychosocial EBP studies included screening or assessment EBPs and some also considered consultation, intervention, or treatment (n = 4) [30,31,32, 34, 36, 41, 45]. Three studies examined implementation of the International Society of Pediatric and Adolescent Diabetes (ISPAD) Clinical Consensus Guidelines for Psychological Care [34, 36, 45]. Only three studies reported specific screening tools used. Two independent groups examined implementation of the Patient Health Questionnaire (PHQ-9), an evidence-based screening tool for depression [30, 31, 41]. One group examined the same screening protocol in two papers, which included the General Anxiety Disorder-7 (GAD-7) for anxiety, Diabetes Stress Questionnaire for Youth (DSQY), Diabetes Self-Management Profile self-report (DSMP-SR), Diabetes Family Conflict Scale, and the Brief Multidimensional Student Life Satisfaction Scale -PTPB version [30, 31]. None of the included studies reported on implementation of a specific evidence-based psychosocial treatment or intervention for youth with diabetes or their families.
Areas of Implementation ResearchOf the 7 studies, 3 documented research-to-practice gaps using provider-reports on surveys [34, 36, 45]. One survey study of 76 (68% response rate) SWEET network clinics found that 89% offer psychological services [34]. Two other survey studies examined implementation of the ISPAD Psychological Care Guidelines among ISPAD listserv members (21.1% response rate, 155 participants) and among pediatric diabetes clinics across the United States (85% response rate; 95 medical and 86 psychosocial providers from 98 clinics) [36, 45]. Results indicate that psychosocial care is often available at pediatric diabetes clinics, particularly larger clinics [36, 45]. However, consistent implementation of ISPAD Psychological Care Guidelines is limited, including delivery of evidence-based screening and intervention (< 55% of clinics in the United States) [45].
Four studies identified barriers and facilitators of implementing a psychosocial EBP [32, 34, 36, 45]. Results from 3 provider-survey studies and 1 qualitative study of providers (n = 7) indicate that common barriers to implementation of psychosocial care include funding for psychosocial services and inadequate staffing of qualified mental health professionals [32,34,36,45. For example, in U.S. pediatric diabetes clinics, a psychosocial provider has an average of four hours per week to care for 100 patients [45]. Medical providers identified some challenges to implementing psychological screening and consultations in clinic, such as logistical barriers (e.g., family leaves clinic before seeing psychology after a positive screen), lack of caregiver awareness of problem (e.g., parent doesn’t know child has anxiety), family negative reactions to this care (e.g., stigma of meeting with psychology), and challenges with referring to mental health providers outside of the diabetes clinic (e.g., lack of qualified professionals, family resistance to this care) [32].
All three psychosocial implementation trials focused on increasing screening and consultation [30, 31, 41]. All studies were single site, pre-post trials reporting adoption as the primary outcome. Variable information regarding strategies tested were provided. In a two-year quality improvement initiative across 4 pediatric endocrinology clinics (> 2150 patients with T1D), depression screening (PHQ-2 and PHQ-9) increased from 0 to 75% on average [41]. Strategies used to increase adoption of depression screening included electronic screening forms with automated scoring, automated alerts to providers for positive screens, electronic health record template, weekly data pulls to measure progress, minimal burden on patients (brief screening measure, involvement of family representative in study design), and availability of in-person follow-up with a mental health professional. The two remaining trials occurred at the same single institution. One trial showed increases of in-person psychosocial screening (N = 232 adolescents; 83% of eligible patients completed the screening protocol) and referrals to psychology (up 25%), although limited information regarding the strategies tested were noted [30]. The second study was a quality improvement project that occurred at the height of the COVID-19 pandemic and resulted in a return to pre-COVID-19 pandemic levels of screening (up to 56% of eligible patients by study end) and consultation (peaking at 31% in final cycle) [31]. Strategies to increase screening during the pandemic included remote access to psychosocial screeners for families (email to caregivers with link to online screeners), increasing awareness about these screeners among families and medical colleagues (e.g., daily list of patients screened to medical colleagues to start the day, calls to caregivers to confirm receipt of email with link), allowing adequate time for families to complete screeners, and access to technology for remote visits, remote consenting, and warm-hand-offs for psychology consultations.
Models/Theories/Frameworks and TerminologySimilar to pediatric diabetes medical care implementation trials, these psychosocial trials largely involved pre-post designs and did not explicitly describe implementation strategies consistent with reporting guidelines, or measure implementation outcomes. Taken together, these 7 psychosocial pediatric diabetes studies were not described as implementation science research and thus did not employ implementation terminology, models, theories, or frameworks, or reporting standards for implementation science studies.
Consideration of EquityFive out of seven studies mentioned equity and offered data regarding differences in access to care and outcomes across youth race, ethnicity, and rurality. For example, one study reported lower rates of depression screening in clinics serving patients with minority race/ethnicity compared to clinics serving predominantly White patients [41]. Differences in access to trained mental health professionals across higher compared to lower income continents and larger compared to smaller clinics were also documented [36]. While no studies aimed to shift care to be more equitable, all three trials were completely or partially conducted in clinics serving racially and ethnically diverse populations.
Pediatric Diabetes EducationEvidence-Based PracticesThe two included education studies focused on two models of diabetes education, one as an adaptation to an existing evidence-based curriculum for adults and the other focused on education for families when a child is newly diagnosed with T1D (i.e., Hospital-Based Home Care; HBHC).
Areas of Implementation ResearchOne paper noted gaps in evidence-based diabetes education standard practice. Using surveys of members of the United Kingdom Diabetes register for specialist nurses, 49.5% of specialty nurses (N = 96, 74% response rate; 79.2% pediatric diabetes specialty nurses) reported that their program offered formal education, 36.8% reported education about counting carbohydrates, and 32.6% educated about counting portions [47].
Both papers describe single-institution studies aimed at identifying barriers and facilitators of diabetes education. Provider (medical, psychosocial, educators) feedback was the primary method for understanding barriers and facilitators. In the UK specialty nurse survey study described above, barriers to implementing a structured Dose Adjustment for Normal Eating (DAFNE)-type pediatric diabetes education course included concerns for youth understanding complex regimens, provider staffing, and provider time [47]. In a qualitative study guided by the Promoting Action on Research Implementation in Health Services (PARIHS) framework, investigators used ethnographic observations of team meetings at a single diabetes center to identify implicit facilitators and barriers based on the culture of the clinic and providers (N = 24; pediatricians, pediatric nurses, dietitians, social workers) [43]. Barriers to implementing an at-home new onset diabetes education programs included resistance to both shifting existing practice (specifically providing structured, age-dependent information) allowing early discharge, as well as provider anxiety for patient safety [43].
Models/Theories/Frameworks and TerminologyWhile one of these two studies employed an implementation science framework, findings are limited by the narrow data collection approaches, limited description of the clinic context, and inclusion of only direct care professionals at one site as research participants.
Consideration of EquityNeither paper examining diabetes education and implementation noted issues around equity.
Transition from Pediatric to Adult Diabetes CareEvidence-Based PracticesTwo studies considered implementation of support tools around the transition from pediatric to adult diabetes care, namely Transition Readiness Assessment Tool (TRAQ) and Got Transition, an evidence-based framework for transition from pediatric to adult care.
Areas of Implementation ResearchOne paper is a protocol for a quasi-experimental pre-post trial with a control group across five health centers in the Ontario Pediatric Diabetes Network (Got Transition) [46]. This trial will evaluate audit and feedback approaches, or strategies, (which compare results to standards or peer performance and providing feedback to providers) for implementing Got Transition to support transition to adult care among 3 cohorts (n = 225 each) of young adults with T1D.
The second study involves a single institution quality improvement project to identify barriers of implementing TRAQ as well as to conduct a pre-post intervention evaluation to increase
Comments (0)