
Remember me
In the present study, data from the Dresden Burnout Study (DBS) were used. Study design, recruitment strategy, and data collection have been described in more detail elsewhere [25]. In brief, the DBS was a prospective study investigating biopsychosocial determinants of burnout. The study was approved by the local ethics committee and conducted in accordance with the Declaration of Helsinki. Registration and data collection started in January 2015. In addition to self-evaluated questionnaires, information on sociodemographic factors was obtained. One essential questionnaire for our study was included only at the third follow-up assessment point (FU3). Therefore, for our longitudinal analysis, three consecutive assessment timepoints of the participants were included in the data analysis. Thus, for the present paper, data collected from August 2019 (starting point of FU3) to August 2023 were included. For participants who entered the study from the third timepoint (FU3), timepoints FU3, FU4, and FU5 were included. For participants who only entered the study from the fourth timepoint (FU4), timepoints FU4, FU5, and FU6 were included. This procedure ensures that a consistent number of three timepoints is available for all participants at the end of the analysis. For simplicity, the terms time 1 (T1), time 2 (T2), and time 3 (T3) are used instead in the following manuscript. Participants of the DBS were recruited via the Internet (www.dresdner-burnout-studie.de) and via the population registry mainly of the Dresden area. Initial inclusion criteria for this substudy were age between 18 and 68 years and full- or parttime employment. A sample of N = 846 for T1, N = 857 for T2, and N = 606 for T3 was obtained according to these inclusion criteria. Only individuals for whom the time intervals between T1 and T2 (mean [Mdays] = 428.52; standard deviation [SDdays] = 48.88: M + 1.5 × SD = 501.84 days ≙ 1.38 years) and between T2 and T3 (Mdays = 380.07; SDdays = 13.57: M + 1.5 × SD = 400.42 days ≙ 1.10 years) were at least 1 year and at most 3 years were included. In total, the sample consisted of 1381 individuals.
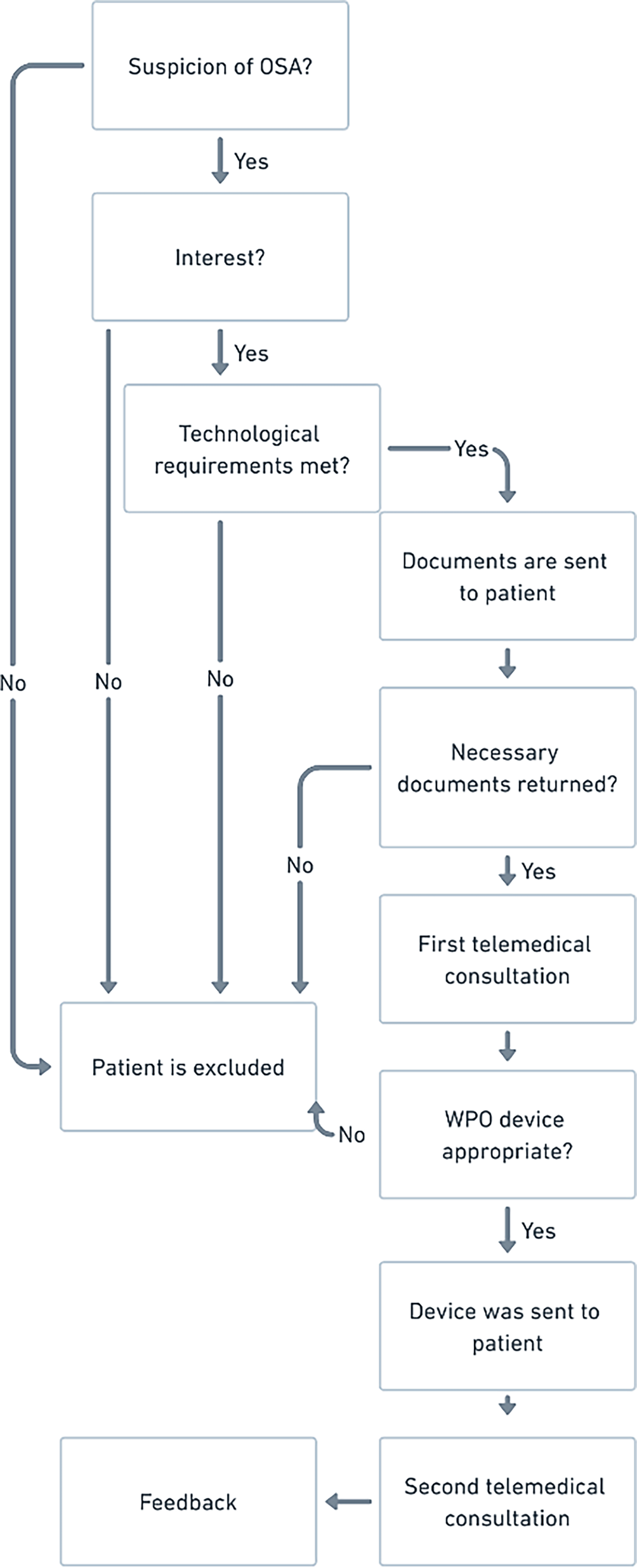
Out of the total of 1381 individuals, 368 were participants at all three timepoints. In total, 73.35% dropped out or did not participate at all three timepoints. After excluding 8 individuals due to incomplete questionnaire responses, we included 360 individuals (nfemale = 227) in the analysis of reduced sleep quality (SQ) and ERI. A detailed description of the exclusion process is presented in Fig. 1, and a descriptive summary of the sample is presented in Table 1.
Fig. 1
Participation rate, including study inclusion criteria, illustrated with a flowchart
Table 1 Sociodemographic and descriptive statistics of the sample including rumination, sleep quality, and effort–reward imbalance variables at time 1, time 2, and time 3Self-reported measuresEffort–reward imbalanceFor evaluation of work-related stress, the standardized 16-item short version of the effort–reward imbalance questionnaire was used [34], assessing the three dimensions “effort” (three items), “reward” (seven items), and “over-commitment” (six items). Items of all dimensions are answered on a four-point Likert scale (1 = strongly agree, 2 = agree, 3 = disagree, 4 = strongly disagree). Sum scores can be created for each dimension , whereby the higher the sum score, the higher the deviation in the respective dimension. Furthermore, to address the research questions of this study, an effort–reward ratio can be used, representing the imbalance between the two constructs [33]. Internal consistency (ERI: α = 0.82; effort: α = 0.74; reward: α = 0.81) was acceptable.
Sleep qualityThe German version of the Pittsburgh Sleep Quality Index (PSQI; [4]) was used to assess SQ at the three assessment timepoints. The PSQI questionnaire consists of a self-evaluating part (19 items) and a part evaluated by the partner or roommate (5 items). Seven different dimensions of sleep (subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, sleep medication, and daytime dysfunction) are examined, which can be converted into an overall score between 0 and 21. A high overall score (values >5) indicates low SQ, so the higher the value, the worse the SQ [4]. Test–retest reliability reported by a previous study was good, r = 0.89 [1]. The test–retest reliability (r = 0.70) in our study was acceptable.
Work-related rumination questionnaireFor evaluation of work-related rumination at the three assessment timepoints, the work-related rumination questionnaire (WRRQ) was used [6]. This self-evaluating questionnaire evaluates three dimensions of rumination: affective rumination (five items; e.g., “Do you become tense when you think about work-related issues in your free time?”), problem-solving pondering (five items; e.g. “In my free time I find myself re-evaluating something I have done at work”), and detachment (five items; e.g. “Do you find it easy to unwind after work?”). Items are answered on a five-point Likert scale (1 = very seldom/never, 2 = seldom, 3 = sometimes, 4 = often, 5 = very often/always). Item 6 (detachment scale) was reverse coded. The higher the rumination dimension scores, the more the person ruminates. The reliability investigated by a previous study was α = 0.84 for affective rumination, α = 0.84 for detachment, and α = 0.83 für problem-solving pondering [24].
Internal consistency in the current study was acceptable (WRRQ: α = 0.91; affective rumination: α = 0.85; detachment: α = 0.89; and problem solving: α = 0.76).
ConfoundersIn addition to the described psychometric measures—PSQI and ERI—several variables were used as potential confounders in adjusted analyses. Because of their potential systematic influence on either SQ or ERI, age, sex, body mass index (BMI), and depressive symptoms (PHQ-9) were included as covariates in adjusted analyses. Longitudinal and cross-sectional analyses were additionally adjusted for baseline levels of the independent variable and differences in days between T1 and T2.
Data analysisAll analyses were conducted using R Studio version 4.3.2 [28]. Sociodemographic variables were examined using descriptive statistics. Means, standard deviations (SD), ranges, and Pearson correlations were calculated for continuous variables. Correlation coefficients were interpreted according to Cohen’s [5] guidelines. Based on an outlier criterion of 2.5 times the interquartile range, 42 participants were excluded from the mediation analysis. The PROCESS macro for R Studio was used for mediation analysis [14, 15]. Inference on the statistics is based on bootstrapping methods, as many of these statistics have irregular sampling distributions, making inference problematic using conventional methods [14].
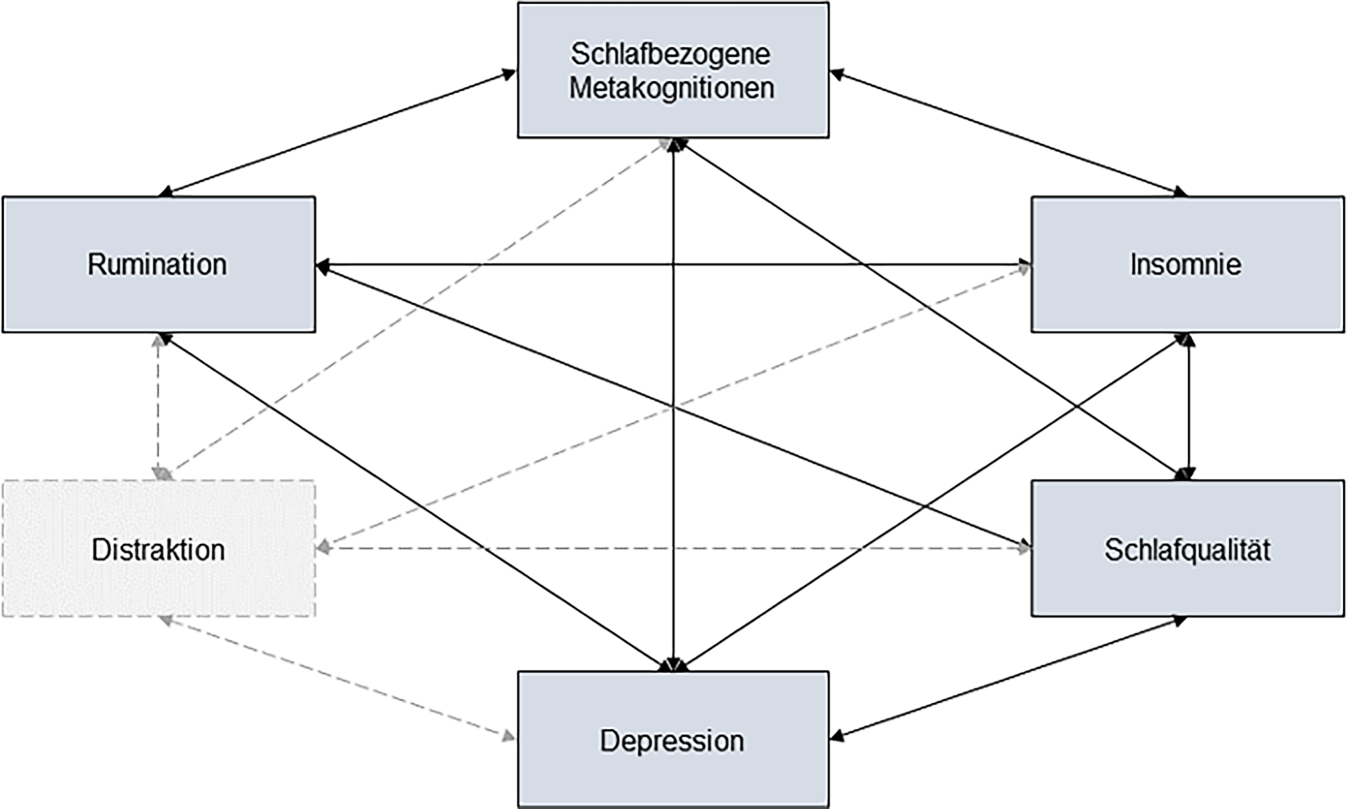
In a first step for cross-sectional mediation analysis, the model included a predictor (ERI at T1), potential mediators (work-related rumination [affective rumination, problem-solving rumination, and detachment at T1]), and an outcome variable (SQ at T1). In a second step, age, sex, and BMI (at T1) were controlled, and in a third step, depressive symptoms (at T1) were also controlled. The a‑path shows the relationship between ERI (predictor assessed at T1) and work-related rumination subscales (potential mediators assessed at T1). The b‑path shows the relationship between each work-related rumination subscale and SQ (Fig. 2a, c, e).
Fig. 2
Proposed cross-sectional and longitudinal mediation models. a Cross-sectional mediation model. b Longitudinal mediation model. a independent variable to mediator path, b mediator to dependent variable path, c total effects of independent variable on dependent variable, c’ direct effects of independent variable on dependent variable. T1 time 1, T2 time 2, T3 time 3
In the longitudinal analysis, all three steps are conducted analogously to the cross-sectional analysis. The predictor (ERI at T1), mediator (affective rumination, problem solving, and detachment at T2), and outcome variable (SQ at T3) remain the same, but they describe the data at different timepoints (Fig. 2b, d, f). The covariates age, sex, BMI, and depressive symptoms also describe the data from T2.
Bootstrap tests (10,000 replicates and 95% confidence interval) were used to compute confidence intervals and inferential statistics and to test the significance of the mediating effect where the 95% CI does not include zero, indicating significant effects. The total effects of the mediation models were interpreted to answer the first three hypotheses. For the fourth hypothesis, the entire mediation model was used.
Comments (0)