
Remember me



Dementia[1-3] and depression[4] are significant causes of non-fatal disease burden globally. It is estimated that depression may be present in 27.5% of the elderly persons staying in community-dwelling[5] and in 65% of the elderly persons who are institutionalised.[6] It cannot be underestimated that quality of life (QOL) plays a paramount role in defining healthy ageing[7], and the presence of depression can compromise QOL, more so in elderly persons.[8,9] It is being emphasised that there is a need for strategies to facilitate healthy ageing, and to achieve this objective, there is a need to have preventive medicine strategies[10] that can preserve mental and physical well-being but also can reduce the social, emotional and physiological disabilities.[11] Studies have emphasised the need for alternative non-pharmacological methods to improve the overall QOL and well-being of elderly people, particularly those with cognitive impairment.[12,13] Increasingly, the role of music in its various forms and music therapy (MT) has been explored to improve the physical, psychological and physiological functioning of the ageing population.[3,8,14-19] Although many studies have shown that MT is effective, other studies have raised concerns about the overall effectiveness of MT over other modalities,[20] including modalities such as reading or other group activities to improve the features of dementia.[15] In the older population, with or without dementia, depression, and Alzheimer’s, MT helps improvement of depression, QOL and cognition in comparison with the older population not receiving MT. The present systematic review and meta-analysis try to find out the status, role and scope of MT to improve the QOL in elderly patients, particularly dementia and altered mental functions.
METHODSWe used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting the present review.[21] A systematic literature search was conducted across PubMed, SCOPUS, Central Cochrane Registry of Controlled Trials (the Cochrane Library) and ScienceDirect databases, using the search terms outlined in Table 1. In addition, the reference lists of included studies were reviewed for potentially relevant studies. Three investigators (SM, SKT and AG) independently screened abstracts, with selected articles undergoing full-text evaluation. Conflicts were resolved through consensus, resulting in a final list of studies. Only randomised controlled trials (RCTs) conducted in the older population and comparing MT were included in this review. Quasi-randomised controlled studies, prospective and retrospective observational studies, case series, case reports, letters, editorials, comments, animal studies and non-English literature studies were excluded from the study. Three investigators independently assessed studies and extracted data using a pre-designed pro forma based on inclusion criteria. The PRISMA flow chart illustrating the study selection process is presented in Figure 1. The details included were study authors, study year, country, sample size in each group, age and gender, inclusion/exclusion criteria, type of interventions, reported outcomes and details of follow-up. Authors were contacted for missing data. Discrepancies were resolved with consensus.
Table 1: Details of search strategy.
Database Search details COCHRANE 2 Cochrane reviews matching geriatric quality of life music in title abstract keyword PubMed ((‘geriatric’ [All Fields] OR ‘geriatrics’ [MeSH Terms] OR ‘geriatrics’ [All Fields]) AND (‘quality of life’ [MeSH Terms] OR (‘quality’ [All Fields] AND ‘life’ [All Fields]) OR ‘quality of life’ [All Fields]) AND (‘music’ [MeSH Terms] OR ‘music’ [All Fields] OR ‘musics’ [All Fields] OR ‘musical’ [All Fields] OR ‘musicality’ [All Fields] OR ‘musically’ [All Fields] OR ‘musicals’ [All Fields] OR ‘musics’ [All Fields])) AND ((randomisedcontrolledtrial [Filter]) AND (1000/1/1:2024/1/3 [pdat])) ScienceDirect Title, abstract, keywords: geriatric quality of life music SCOPUS TITLE-ABS-KEY (geriatric AND quality AND of AND life AND music) AND (LIMIT-TO [DOCTYPE, ‘ar’])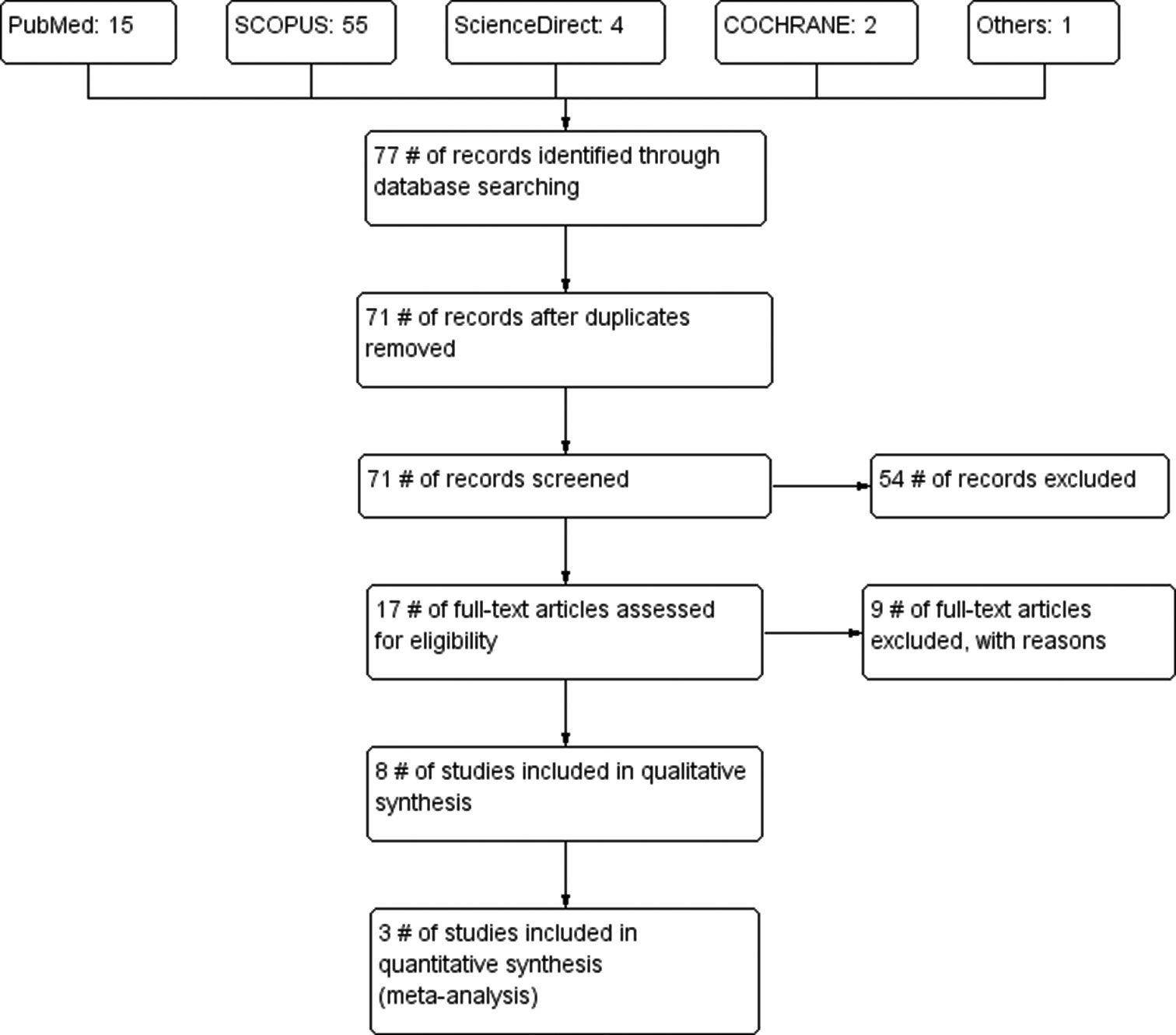
Export to PPT
Statistical analysisThe meta-analysis was conducted using Review Manager (version 5.3, Cochrane Collaboration). A random-effects model was used for the meta-analysis as there was inherent heterogeneity among studies. Forest plots were generated to represent individual study effects and heterogeneity among studies was assessed using the Cochrane Q test and I2 statistic. A significance level of P < 0.10 or I2 > 50% was considered to suggest substantial heterogeneity. The revised JBI critical appraisal tool was employed to assess the risk of bias in RCTs.[22]
RESULTSA systematic search was conducted with the predefined search criteria, as mentioned in Table 1, which yielded 76 records. Six articles were removed due to duplication. After screening the articles based on their titles, 54 records were excluded from the study. Sixteen full-text articles were studied for eligibility, resulting in eight articles included for qualitative synthesis. The excluded eight articles, along with the reasons for their exclusion, are listed in Table 2.[23-30] The characteristics of the included articles for qualitative synthesis are detailed in Table 3.
Table 2: Characteristics of excluded studies.
Study author (Year) Reason for exclusion Bro et al., 2019[23] Lymphoma, not on dementia Choi et al., 2009[3] Not a randomised controlled trial Kiper et al., 2022[24] Virtual reality box, no music Liao et al., 2018[25] Further updated analysis is available[17] Palumbo et al., 2022[26] Post-stroke, not geriatric alone Pohl et al., 2020[27] Parkinsons disease Prieto-Prieto et al., 2022[28] Exercise not on music Raglio et al., 2016[29] Language in stroke, not on dementia Villaverde Gutiérrez et al., 2012[30] Exercise not on musicTable 3: Characteristics of included studies.
Study country Age (mean) Sex M/F subjects Inclusion Exclusion intervention Outcome variables and Follow up Remarks Chan et al., 2012[18] Singapore range- 55–75 MT- 9/15; C-9/17 MT-24; C-26 Older people>55 year, able to communicate and not hospitalised No consent, inability to hear, read and write 30 min music (pre-recorded) at home per week for 8 weeks; controls- undisturbed 30 min GDS-15 at 8 weeks MT can help in reducing depression in older people Cooke et al., 2010[15] Australia range-65–95 14/33 24/23 Early to mid-stage dementia (MMSE-12–24); Alz; documented agitation and aggression Not clear 40 min sessions (musician+pre-recorded) 3 days/week for 8 weeks; control-reading DQOL, GDS, MMSE at 8 weeks Music and reading can improve self-esteem and depression in some older people with dementia. Liao et al., 2019[17] Malaysia MT-71.72±7.331;c-71.87±8.002 MT-19/38;c-24/31 MT-55; C-57 Selected communities, GDS score ofAmong these eight articles, two are from Singapore, two from Japan and one each from Australia, Malaysia, France and Italy. The article reported age ranges ranging from 55 to 95 years. The total number of subjects studied in all these articles combined is 605, with 330 receiving MT, while the remaining served as controls. Three of these studies employed crossover designs, where controls were initially given MT in the second phase. Among the control interventions, one article utilised painting, and another used reading.
The main inclusion criteria in these studies were dementia (n = 4), depression (n = 4), Alzheimer’s (n = 2) and no clear mention of dementia/depression (n = 3). The exclusion criteria used included patients who were not able to hear, read and write, those with comorbidities, individuals unable to walk, patients on palliative care and cases with no clear mention of exclusion criteria (n = 3). The interventions varied across the studies, encompassing differences in the duration of intervention, the number of sessions per week, the nature of the music (prerecorded or live) and the setting (at home or in an MT centre). Two studies employed 1-h sessions, three studies utilised 30-min sessions, two studies implemented 40– 50-min sessions and one study mentioned 2-h/week sessions. In addition, one study incorporated some form of physical exercise along with MT. Regarding the type of music used, three studies employed prerecorded music, while three studies involved a music therapist and two studies involved musicians.
Results of individual studiesThe various outcomes were measured using different scales across these studies: Geriatric depression scale (GDS) (n = 4), Dementia QOL (DQOL), Mini-mental state exam (MMSE); in French: Evaluation Instantanée du Bien-Être (EVIBE); Numeric rating scale (NRS), Philadelphia geriatric centre; European quality of life dimensions; Pittsburgh sleep quality index and Lubben social network scale (LSNS). MT was found to be helpful in five studies. One study showed no significant effect on depression scales, while another study demonstrated improvement in oral, immunological and physical health but not in functional mobility. Yet, another study indicated no improvement in QOL. Due to the common outcome measure of GDS across four studies, a meta-analysis was feasible and conducted as follows.
Risk of bias and quality assessmentAccording to the JBI tool employed for quality assessment, five studies demonstrated a low risk of bias[15-17,19,20], while three studies exhibited a moderate risk of bias.[8,13,18] Detailed information is provided in Table 4.
Table 4: JBI critical appraisal checklist for RCT studies.
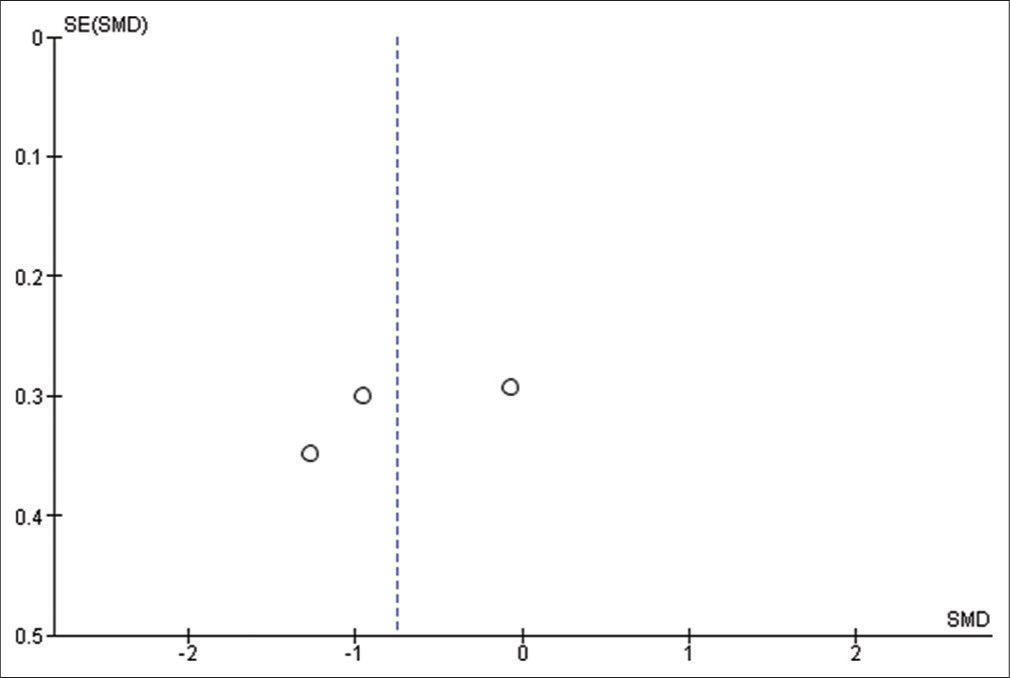
Study ID Item 1 Item 2 Item 3 Item 4 Item 5 Item 6 Item 7 Item 8 Item 9 Item 10 Item 11 Item 12 Item 13 Chan et al., 2012[18] Yes Unclear Yes No No Yes No Yes Yes Yes Yes Yes Yes Cooke et al., 2010[15] Yes Yes Yes No No Yes Yes Yes Yes Yes Yes Yes Yes Liao et al., 2019[17] Yes Yes Yes No No Yes Yes Yes Yes Yes Yes Yes Yes Murabayashi et al., 2019[19] Yes Yes Yes No No Yes Yes Yes Yes Yes Yes Yes Yes Pongan et al., 2020[13] Unclear Yes Yes No No Yes Yes Yes Yes Unclear Yes Yes Yes Raglio et al., 2015[20] Yes Yes Yes No No Yes Yes Yes Yes Yes Yes Yes Yes Shimizu et al., 2013[8] Unclear Unclear Yes No No Yes Yes Yes Yes Unclear Yes Yes Unclear Yap et al., 2017[16] Yes Yes Yes No No Yes Yes Yes Yes No Yes Yes Yes Meta-analysisIn the meta-analysis using a random-effects model with an inverse variance method for continuous data, we compared the GDS scores at follow-up between MT and non-MT groups for three studies.[15,16,18] The overall effect estimate was 0.75, standard error of 1.46 and a confidence interval (CI) -1.46–-0.04), suggesting a positive effect in favour of MT. However, in view of the wide CI, the results need to be interpreted with caution [Figure 2]. The Z statistic was found to be 0.3 (P = 0.04), suggesting that the overall effect is different from zero; however, the modest Z statistic highlights the need for further studies to confirm the positive role of MT. There was significant heterogeneity among the studies on the Q statistic, and the I2 value of 75% further highlights potential differences in the included studies [Figure 3].

Export to PPT
Export to PPT
DISCUSSIONThere are numerous cultures and traditions worldwide; some lack a written language, but none are without music or dance. Music and dance serve as a universal language of expression. It is plausible that our ancestors recognised the significance of MT for well-being, self-esteem and the prevention of depression. In our review, at least two studies emphasise traditional methods of music and dance. While there is limited evidence for the efficacy of MT in relieving pain in conditions such as chronic obstructive pulmonary disorders, Alzheimer’s, multiple sclerosis and Parkinson’s disease, the exact mechanism for how MT improves depression in the elderly remains unclear. Some studies suggest a physiological response through mood alteration, thereby enhancing overall health. The emotional response may be attributed to the involvement of the limbic system.[18]
Yap et al.[16] conducted a crossover RCT involving elderly participants without dementia. The MT intervention included the use of musical instruments under the guidance of experienced instructors, with each session lasting 1 h. A total of over ten sessions were conducted across 11 weeks. The study observed a non-significant reduction in the GDS score by 0.479 (95% CI: −0.329, 1.287) and an improvement in the LSNS by 1.125 (95% CI: −1.134, 3.384). Despite the lack of statistical significance in the scores, the authors noted that the intervention was well-received by the participants. Chan et al.[18] utilised a 30-minute pre-recorded music at home for older individuals, the majority of whom were women (62% not habitually listening to music [LtM]). Many participants had chronic illnesses such as hypertension and diabetes. The variation in depression levels, assessed by GDS scores, was notably different, mainly from the 4th to the 8th week, with a significant P = 0.0016 observed in the 8th week. The significant reduction in depression over the 8 weeks was confirmed by an F-value of 7.05 with P = 0.016.
Liao et al., in 2019[17] utilised traditional Tai Chi with music in 50-minute sessions. The study included individuals with mild-to-moderate depression, characterised by GDS scores of 11–25. The attendance rates were notably high at 98%. The music group exhibited substantial improvements in QOL at 3 months, evident in the physical, psychological, social and environmental domains (F-values of 50.66, 32.97, 56.85 and 27.75, respectively, with P < 0.001). Cooke et al.[15] employed MT in patients with early to mid-stage dementia, as indicated by MMSE scores ranging from 12 to 24, in a crossover study. The sessions, lasting 40 min each, involved collaboration with a musician and utilised pre-recorded music. The study predominantly featured women (70%), many of whom were widowed. Among these participants, 30% had depression. Significant differences in midpoint QOL scores were observed between the music and control (reading) groups (F = 6.672, P < 0.05). Initially, the control group reported higher feelings of belonging (3.61) compared to the MT group (3.17). However, after crossover, the control group’s scores decreased from 3.61 to 3.46, while the music group showed increased scores from 3.17 to 3.57. Regarding depression scores from the GDS, a significant decrease over time was noted (F [2, 22] = 8.129, P < 0.01).
Murabayashi et al.[19] conducted a crossover RCT in 2019 involving older individuals with dementia, depression and frailty. The sessions, lasting 45–50 min, were conducted by a music therapist. Out of the 94 participants, the majority were female (93%). The study found that the MT-first group exhibited significant improvements compared to the waiting-first group in terms of timed up and go (TUG), GDS-15 and general health questionnaire (GHQ-12) scores, with effect magnitudes of −0.64, −0.75 and −0.95, respectively. Following the crossover, the clinical global impressions of improvement responder rate were significantly better in the MT group than the waiting group, with P < 0.05. The study acknowledged limitations, including a small sample size and the exclusion of at least 20 participants due to poor attendance. The female dominance in the study raised concerns about generalizability. Despite the observed improvements in TUG, GDS-15 and GHQ-12 scores with MT, the study noted that cognitive function did not show any significant effects. The authors emphasised the necessity for further research involving specific types of musical activities to better understand the potential benefits of MT in this population.
Raglio et al.[20] conducted a study using MT in older patients with dementia (MMS <18 and neuropsychiatric inventory [NPIS] <18) and depression (Cornell scale for depression in dementia [CSDD] score 1–4). The intervention consisted of 30-minute sessions twice a week for 10 weeks, facilitated by a music therapist using a prerecorded playlist. The study involved three groups: MT, LtM and controls. Results demonstrated significant improvements in behavioural symptoms and depression (assessed by the CSDD score) and QOL (Cornell-brown scale - score) over time. However, these improvements were not specifically attributed to any particular intervention. The reduction in neuropsychiatric inventory (NPI) global score was statistically significant (P = 0.001) with a decrease of 28% in MT, 12% in LtM and 21% in the control group. Post hoc analysis revealed reductions in specific NPI subclasses, including delusion (LtM: 37%, MT: 35% and Controls: 11%) and disinhibition (LtM: −40%, MT: −44%, Controls: −61%). In the MT group, a positive trend, although not statistically significant, was observed for behaviour-related scores. The study acknowledged significant dropout rates and highlighted that the control group received standard care, potentially impacting the results.
Pongan et al.[13] explored the effectiveness of MT in patients with mild Alzheimer’s (MMSE >20) and chronic pain, comparing it to a control group engaging in painting sessions with professional assistance. Both MT and painting groups showed non-significant changes in NRS scores (MT: 2.68–2.39, F = 1.37, P = 0.25; Painting: 3.54–2.88, F = 2.27, P = 0.14). Significant improvements in EVIBE scores were observed in both groups (MT: 3.17–4.30, Painting: 3.44– 3.90), with MT achieving significance (F = 4.10, P = 0.05). The study acknowledges limitations, including variability in pain scores which led to non-significant results in NRS scores and the absence of a proper control group, impacting the assessment of MT and painting effectiveness.
Shimizu et al.[8] conducted a study employing MT in elderly individuals who were not habitual exercisers. The intervention utilised the Naruko clapper, a traditional musical instrument in the community, to create rhythmic movements accompanied by music. The participants attended 1-h sessions of MT per week. Results indicated that MT had positive effects on both psychological and physical function aspects, especially in younger elderly patients whom they considered as <75 years old. Notably, the intervention demonstrated a positive influence on the secretion of SIgA, indicating an immunological function (REL-IAFT: P = 0.004, r2 = 0.181; REL-BEF: P = 0.008, r2 = 0.200). However, no significant differences were observed in physiological indices. The study highlighted the significant impact of age on physiological functioning. It is important to note that the study primarily included women, which represents a limitation.
LimitationsThere is a limitation of the studies, which was the inclusion of some form of physical exercise alongside music, making it challenging to isolate the impact of music alone on the observed results. This factor complicates the interpretation of the findings specifically attributed to the music component.[17] Chan et al.[18] demonstrated a positive aspect with 100% participant retention. However, it is constrained by sample selection bias through snowballing using social networks. No participant was blinded, and there was no control over the frequency of at-home music listening. There is a need for further RCTs with consistent treatment across groups, except for MT and exploration of different timing for sessions[18,20] focusing on grouping participants based on physical function rather than age for a more comprehensive understanding of the intervention’s effects[8] including collaboration between a psychologist and a research nurse.[18] The studies lack a proper control group without any intervention, as the control group in this study consisted of readers, and the reading group also showed significant improvement in depression scores.[15] Yap et al.[16] had that the primary limitation of the study is the small sample size, consisting of only 31 participants; also, the authors underscored the need for further RCTs without a crossover design, citing potential challenges in assessing a washout period due to the possibility of a learned effect from the therapy, unlike in drug studies.
CONCLUSIONThe results of the studies in our review exhibit diversity, with studies employing different assessment scores such as GDS, DQOL and MMSE. A meta-analysis of GDS scores from three studies suggests a positive effect in favour of MT, although caution is warranted due to the wide CI. While MT appears promising in alleviating depression and enhancing physical well-being in the elderly, the heterogeneity and limitations across the studies necessitate further well-designed research to establish its efficacy and understand the specific mechanisms underlying its positive effects. Future studies should address issues such as sample size, control group selection and potential confounding factors to provide more robust evidence for the therapeutic benefits of music in this population.
Comments (0)