
Remember me
Eligible patients were ≥ 18 years of age and had histologically and/or cytologically confirmed advanced solid tumors that had been previously treated with standard-of-care therapy, and either their physicians had determined that such therapy was no longer effective, or patients had declined to receive further non-investigational treatments. Other inclusion criteria were measurable disease according to the Response Evaluation Criteria in Solid Tumors version 1.1. (RECIST v1.1); Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; and adequate hepatic, renal, and hematologic function. Patients in Part B had to have a documented Globo H H-score of ≥ 100, as determined by a validated immunohistochemical assay (NeoGenomics®, San Diego, California, USA) approved by the US Food and Drug Administration (FDA) for use in clinical trials.
Exclusion criteria included a period of less than 3 weeks from prior cytotoxic chemotherapy or radiation therapy; primary immunodeficiency, systemic steroids (prednisone > 10 mg/day or equivalent) or other immunosuppressive agents within the past 14 days; or an active infection requiring systemic therapy, including known infection with human immunodeficiency virus (HIV) or active infection with hepatitis B or C virus; known untreated CNS metastases; or a history of solid organ transplantation. The complete list of eligibility criteria is provided in the Supplementary file.
The study was conducted at multiple centers in the United States and in Taiwan. The study was approved by the institutional review boards of these institutions, and all patients provided written informed consent. The study was conducted in accordance with the ethical principles of the International Council on Harmonization for Good Clinical Practice guidelines, the Declaration of Helsinki, and applicable local regulations and was registered at www.clinicaltrials.gov (NCT03573544).
Study designThis study was conducted in two parts: Part A (dose escalation) and Part B (dose expansion). The primary objectives of Part A were to establish the maximum tolerated dose (MTD) and recommended phase II dose (RP2D) of OBI-888 and of Part B (cohort expansion) to further characterize the safety and clinical activity of the RP2D dose of OBI-888 administered as monotherapy. The secondary endpoints included the characterization of the PK/PD profiles of OBI-888.
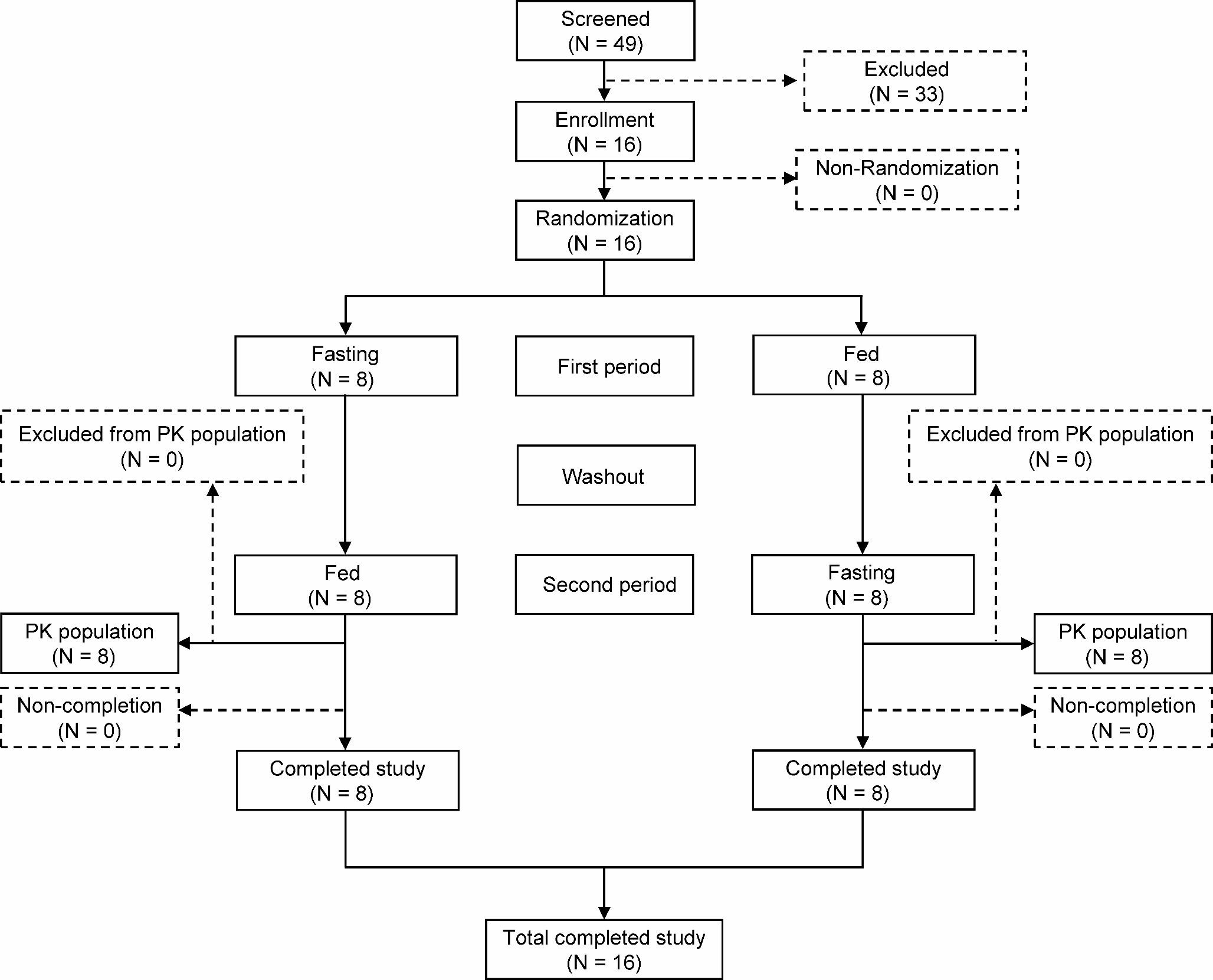
This was an open-label study with eligible patients assigned to a dose level in the order of study entry according to the 3 + 3 design in Part A or to a cohort according to tumor type in Part B (cohort 1: pancreatic adenocarcinoma; cohort 2: esophageal cancer; cohort 3: gastric cancer; cohort 4: colorectal cancer; cohort 5: basket [any solid tumor type other than those included in cohorts 1 through 4]) (Fig. 2).
Fig. 2
Study design: A. Dose escalation; B. Expansion part of the study
TreatmentOBI-888 was administered via intravenous (IV) infusion at doses of 5, 10, or 20 mg/kg in Part A (dose escalation) and at the RP2D of 20 mg/kg in Part B (cohort expansion), on days 1, 8, 15, and 22 of each 28-day cycle in both parts of the study (Fig. 2). The infusion was administered for a duration of approximately 90 min (± 10 min) for cycles 1 and 2, with the option of reducing the infusion time of cycle 3 to 60 or 30 min at the discretion of the investigator, provided that no infusion-related AEs occurred at prior dose levels. DLTs were defined as any of the following that occurred within 28 days of starting the study treatment: grade 4 neutropenia, grade ≥ 3 febrile neutropenia with or without infection, grade 4 thrombocytopenia or grade 3 thrombocytopenia with bleeding, grade ≥ 3 nausea and vomiting or diarrhea for more than 72 h despite optimal supportive care, or any other grade ≥ 3 non-hematological AE that did not resolve before the next infusion. Treatment was continued until progressive disease, unacceptable toxicity, or a decision by the investigator or patient to discontinue treatment.
Patient monitoringSafety assessments, including vital signs, physical examinations, electrocardiography recordings, AEs, and clinical laboratory tests (routine hematology, serum chemistry, coagulation, and urinalysis), were performed at protocol-specific visits (on cycle 1; days 1, 8, 15, and 22; and on day 1 of each subsequent treatment cycle).
A treatment-emergent adverse event (TEAE) was defined as an AE with an onset date on or after the start of treatment with the study drug or an AE that was present prior to the receipt of the study treatment and worsened in severity or increased in frequency, on or after the first dose. TEAEs were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE), version 4.03. AEs having both onset and end dates missing were defined as TEAEs, and events reported as “unrelated” or “unlikely related” were defined as unrelated to the study drug. Events reported as “possibly related,” “probably related,” or “definitely related,” as well as events with no reported relationship information, were defined as drug related.
Computed tomography or magnetic resonance imaging evaluations were performed during screening and every 8 weeks (± 1 week) for the first 6 months of the study, and then every 12 weeks (± 1 week) thereafter and at the termination visit. The tumor response was measured using RECIST v1.1 [11]. Stable disease lasting ≥ 4 months was considered clinical benefit [12, 13].
PharmacokineticsBlood samples for the PK analysis of OBI-888 levels were collected immediately prior to infusion, immediately following the end of the 90-min infusion, and 1, 4, and 8 h after the end of the infusion during cycle 1 on days 1, 8, 15, and 22 in Part A. Samples were collected prior to infusion during cycle 1, days 1, 8, and 15; immediately after infusion during cycle 1, days 1 and 15; and 1, 3, and 6 h after the end of infusion during cycle 1, and day 1 in Part B.
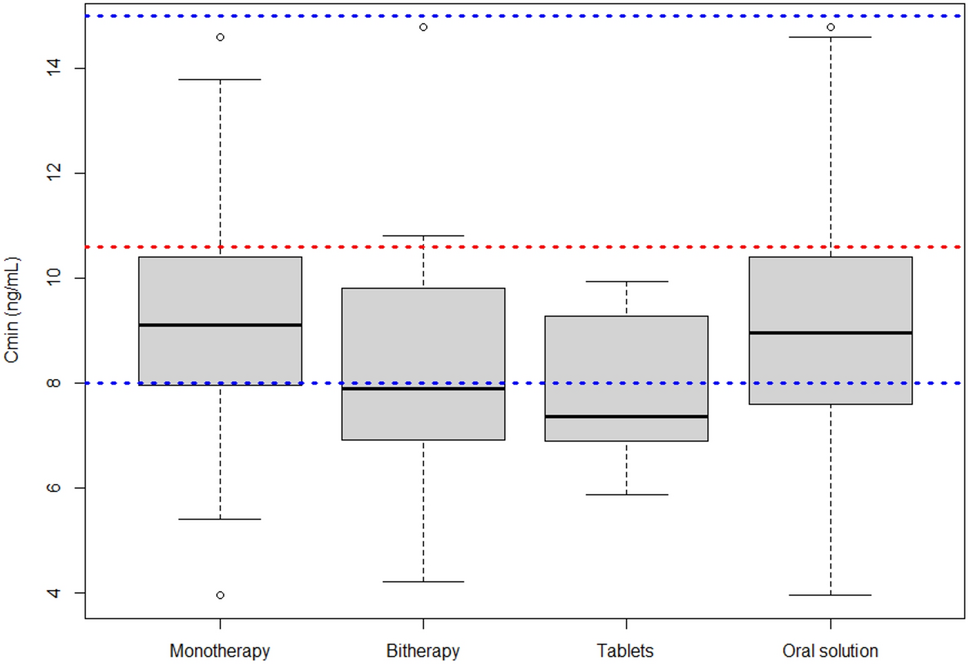
The concentration of the study drug was determined from the serum samples using a validated ELISA method. PK parameters were calculated using a non-compartmental method (Phoenix WinNonlin Software, v8.3) from blood samples collected during cycle 1, dose 1 and included Cmax, total exposure (AUC), half-life (t1/2), clearance, and volume of distribution (Vd). To assess the attainment of the steady state, trough (Cmin) concentrations and peak concentrations (end of infusion) of each dose were obtained directly from the analytical data.
Pharmacodynamics and biomarkersTumor tissue samples were collected from all the patients at the time of screening for entry in both parts of the study. While attempts were made to obtain fresh biopsy specimens, archival samples were retained along with the histology or pathology report when possible. All fresh biopsy specimens or archival samples were sent to the central laboratory (NeoGenomics, Aliso Viejo, California, USA) for Globo H expression analysis using a validated immunohistochemical assay (NeoGenomics) approved by the US FDA for use in clinical studies.
Tumor biopsy samples mandated at baseline were also used to examine the expression of immune markers, such as tumor-infiltrating lymphocytes, including natural killer cells, and immune checkpoints, such as PD-L1, using immunohistochemistry, as well as to evaluate the expression of additional tumor-associated glycans. Blood samples used for PK and antidrug antibody (ADA) assessments were pooled and used for serum glycan analysis. Blood samples were collected during cycle 1, days 1 and 15; cycle 2, day 22; and cycle 4, day 1 for ADCC analysis (serum samples were analyzed using the ADCC Reporter Bioassay [Promega, Madison, Wisconsin, USA] established on Globo H-expressing MCF-7 cells); cycle 1, days 1, 8, and 15 for CDC/ADCC analysis; and cycle 1, day 1 for KIR, HLA, and FcγR genotyping.
ImmunogenicityADAs against OBI-888 were assessed in serum samples obtained prior to infusion during cycles 1 and 2, days 1, 8, 15, and 22; every two cycles beginning with cycle 3; and at the end of the study/early termination using a series of validated ELISA-based assays (Syneos Health, Morrisville, North Carolina, USA). For patients with persistent antibodies at the end of the study, an additional ADA sample was collected four months after the end-of-study visit, if possible.
Statistical analysisA “3 + 3” design was used in the dose-escalation part of the study (Part A). The cohort-expansion phase (Part B) was designed to enroll up to 150 total patients based on Simon’s 2-stage design [14], with up to 9 patients in each cohort recruited in the first stage. If at least one objective response was observed within the first six cycles of therapy, up to 21 additional patients were enrolled in that cohort, for a total of up to 30 patients per cohort. If at least four objective responses were observed within the first six cycles of therapy in these 30 patients, then OBI-888 was considered worthy of further evaluation. This design was based on the assumption that an overall response rate of 5% or lower would result in a low level of interest in further development of the treatment, whereas an overall response rate of 25% or higher would elicit a high level of interest in the treatment. The sample size was based on a one-sided alpha of 0.05 and 90% power. The 95% confidence interval (CI) was estimated using the exact binomial distribution.
Comments (0)