
Remember me
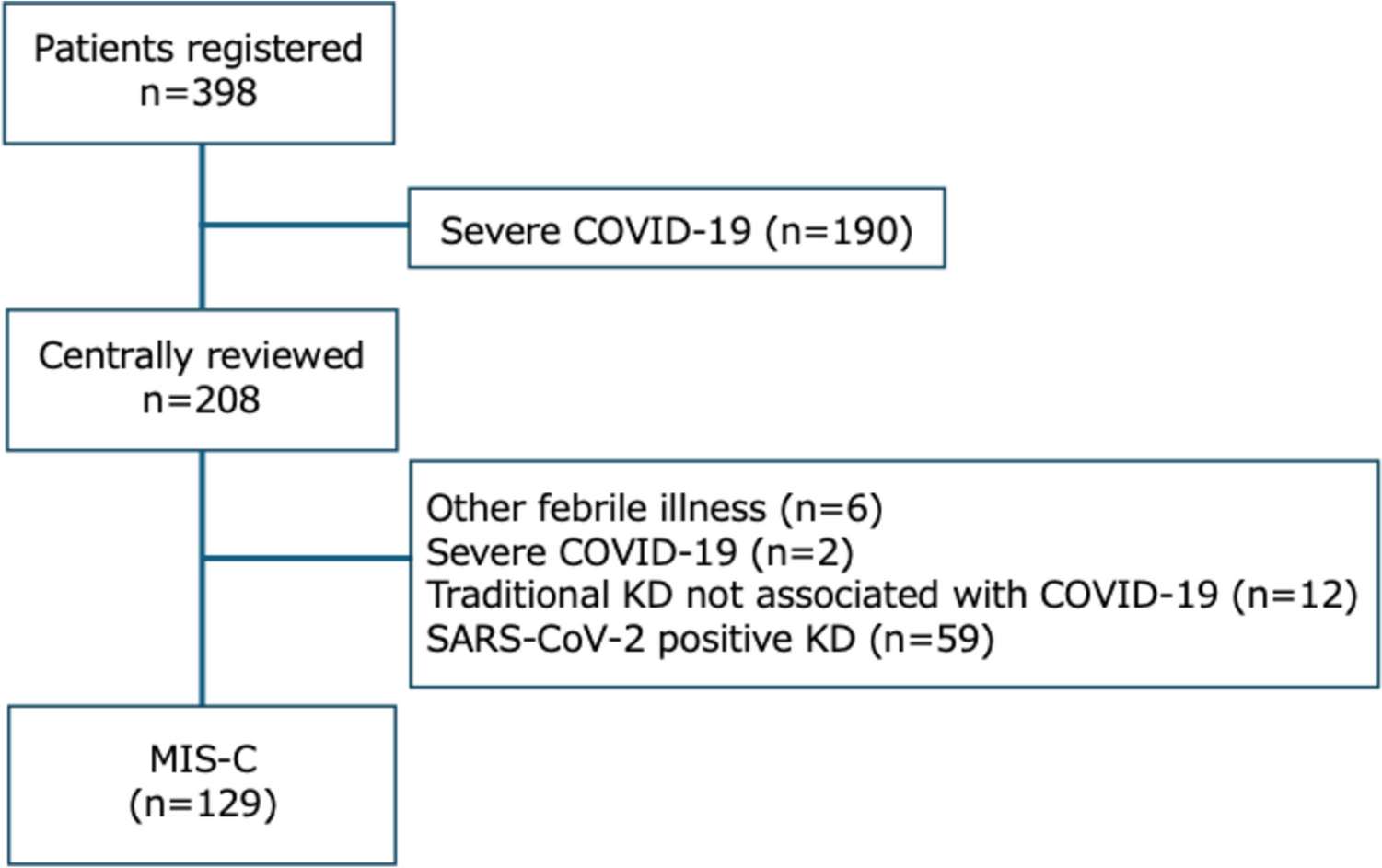

In total, 253 patients were enrolled into the study and were included in the full analysis set (Fig. 2). Two out of the 50 participants who discontinued the study during Epoch 1 withdrew consent because of AEs. One patient experienced fatigue, which was of moderate severity, probably related to treatment and later resolved/recovered. The AEs experienced by the second patient included pyrexia, headache, and myalgia, all of which were mild, possibly related to treatment, and later resolved/recovered. One of these patients was negative for binding anti-rHuPH20 antibodies and the other patient did not undergo testing. No participants discontinued the study during Epoch 2 owing to AEs. None of the enrolled patients tested positive for binding anti-rHuPH20 antibodies at any time prior to enrollment. Among 14 participants who were positive for treatment-emergent anti-rHuPH20-binding antibodies during Epoch 1, 13 entered Epoch 2 (1 patient withdrew consent). Most participants in the study had a history of Ig treatment (n = 242/253, 95.7%) and many patients had ongoing fSCIG 10% treatment at enrollment (n = 141/169, 83.4%). Participant demographics and characteristics are summarized in Table 1.
Fig. 2Patient disposition. aTwo fatal AEs (possible stress-related complication of chronic lymphocytic leukemia; cardiogenic shock) were reported, neither of which was considered to be treatment-related. bOther reasons included: unable to keep timely appointments (n = 2); switched to home infusion and would not complete diary and/or questionnaire (n = 2); switched to home infusion (n = 1); switched to another treatment (n = 1); transferred care (n = 1); did not restart fSCIG 10% (n = 1). cParticipant eligible for entry into Epoch 2 (anti-rHuPH20 antibody titer of ≥ 1:160 in Epoch 1) but withdrew consent before entry. AE adverse event, fSCIG facilitated subcutaneous immunoglobulin, rHuPH20 recombinant human hyaluronidase
Table 1 Baseline participant characteristicsTreatment CharacteristicsParticipants received fSCIG 10% treatment for a median (interquartile range [IQR]) duration of 10.0 (3.5–11.8) months. Participants who discontinued fSCIG 10% could remain in the study for anti-rHuPH20 antibody and safety assessments. Among the 37 participants who discontinued fSCIG 10% permanently at an Epoch 1 visit, 14 participants remained in the study. During Epoch 2, two participants discontinued fSCIG 10% and 21 participants discontinued fSCIG 10% at a completion/termination visit. fSCIG 10% discontinuation due to AEs occurred in four, one, and six participant(s) at Epoch 1, Epoch 2, and the completion/termination visits, respectively.
Infusion parameters for participants with available treatment data during follow-up are summarized in Table 2. The majority of infusions were administered every 4 weeks (1197/2201, 54.4%, n = 225) and at home (1395/2230, 62.6%, n = 227), with a median (IQR) number of infusion sites of 2 (2.0–2.0, n = 203). Of participants with available data (n = 227), most (n = 144, 63.4%) used two sites, 30 (13.2%) used only a single site, and 29 (12.8%) used one or two sites. The most frequently used infusion site location was the abdomen, including the left upper abdomen (22.5%), right upper abdomen (22.3%), right lower abdomen (18.1%), and left lower abdomen (17.0%).
Table 2 fSCIG 10% treatment characteristicsSafety and TolerabilityOverall, 98.5% of infusions were administered without rate reduction, interruption, or discontinuation due to AEs. Treatment-related, non-serious AEs (including infections) were experienced by 52 participants (20.6%, 284 events) (Table 3). Overall, the rate of all SAEs was 0.207 per person-year (95% confidence interval [CI]: 0.159–0.266). The incidences of serious, non-serious, and local and systemic AEs related to fSCIG 10% are shown in Table 4. Most treatment-related AEs were either mild or moderate in severity. Two participants (0.8%) each experienced one treatment-related SAE (aseptic meningitis and deep vein thrombosis). Two fatal AEs (possible stress-related complication of chronic lymphocytic leukemia, and cardiogenic shock; 0.8%) were reported, neither of which was considered to be treatment-related. The incidence of all non-serious AEs (number of events per person-year, including infections) was lower among patients previously treated with fSCIG 10% (3.068, 532 events, n = 98/141) than those naive to fSCIG 10% treatment at enrollment (5.790, 161 events, n = 21/28). There was also a marked difference in the number of events per person-year of systemic non-serious AEs between participants previously treated with fSCIG 10% (0.623, 108 events, n = 21/141) and those naive to fSCIG 10% treatment (1.690, 47 events, n = 5/28).
Table 3 Treatment-related AEs, including infectionsTable 4 Treatment-related AEs by severity and by preferred termImmunogenicityOf 196 participants enrolled, for whom at least one anti-rHuPH20 assessment was completed, 14 (7.1%) tested positive for treatment-emergent anti-rHuPH20-binding antibodies (maximum titer 1:10 240). Samples from four patients with anti-rHuPH20 antibody titers ≥ 1:10 000 did not cross-react with other human hyaluronidases (hyaluronidase-1, hyaluronidase-2, and hyaluronidase-4). The incidence of a positive anti-rHuPH20 antibody test according to the specific PID diagnosis was highest in participants with specific antibody deficiency (11.8%; 95% CI: 3.3–34.3) followed by hypogammaglobulinemia (9.1%; 95% CI: 3.1–23.6) and common variable immunodeficiency (6.6%; 95% CI: 3.5–12.0). Among 150 participants with an assessment at baseline, eight (5.3%) were positive for anti-rHuPH20 antibodies, six (75.0%) of whom were treated with fSCIG 10% prior to enrollment.
Overall, among participants with positive antibody titers, titers generally increased over Epoch 1, with varying trends over time in Epoch 2 (Fig. 3). However, the incidence of non-serious AEs related to fSCIG 10% treatment did not increase after the first positive anti-rHuPH20 titer. No participants experienced any treatment-related SAEs before or after the first positive antibody test and no neutralizing antibodies were detected.
Fig. 3Anti-rHuPH20 antibody titers over Epochs 1 and 2. rHuPH20, recombinant human hyaluronidase
Patient-Reported OutcomesMost respondents reported self-administration to be easy (22/56, 39.3%) or very easy (18/56, 32.1%) at Month 12 of Epoch 1 (Supplementary Table S1). During Epoch 1, among respondents with available treatment preference data (n = 91), almost all (98.9%) planned to continue fSCIG 10% treatment.
In general, HRQoL measurements remained stable over the study. The mean (SD) change in the EQ-5D-3L VAS score from baseline to Month 12 of Epoch 1 was 2.5 (15.88) (Supplementary Table S2). The EQ-5D-3L questionnaire results are summarized in Supplementary Table S3. The proportion of respondents who reported some anxiety/depression or problems with activities decreased over Epoch 1 (33.6% at baseline to 23.9% at Month 12 of Epoch 1) (Supplementary Table 31). By contrast, the proportion of respondents reporting some problems with pain/discomfort increased over Epoch 1 (54.1% at baseline to 62.7% at Month 12 of Epoch 1).
SF-36v2 scores were indicative of normal health and remained stable over Epoch 1 (mean [SD] changes from baseline to Month 12 of Epoch 1 were − 0.4 [5.49] and 0.5 [8.16] for physical and mental component summary scores, respectively) (Supplementary Table S4).
Healthcare Resource UtilizationAt the time of study completion/discontinuation, 56 hospitalization events (event rate [number of events per person-year]: 0.191) and 287 days in hospital (event rate: 0.980) had occurred. In total, 15 participants (event rate [number of events per person-year]: 0.051) had at least one hospitalization event owing to an infection (Supplementary Table S5). There were no abnormal total IgG levels within the 4 weeks prior to or during hospitalization.
Comments (0)