The incidence of MRONJ in osteoporotic patients remains relatively low, ranging from 0.001 to 0.4% [5,6,7, 23]. However, tooth extractions elevate MRONJ risk to 3.4% [8,9,10, 23, 24]. Nonetheless, avoiding extractions solely due to MRONJ concerns is unwarranted, as infection may be the primary cause of osteonecrosis [19]. Identifying risk factors for MRONJ in osteoporotic patients poses challenges due to the limited cases and restricted use of diagnostic images [25]. Thus, we aimed to describe the effects of ARDs on the maxilla and mandible and risk factors for the development of MRONJ using clinical data and CBCT in osteoporotic patients undergoing tooth extractions. Our findings indicate that patients under low doses of ARDs present thicker lamina dura and extended post-operative healing times and have a higher risk of MRONJ if under corticosteroid treatment or undergoing extractions of multi-rooted teeth. Moreover, sequestrum formation serves as a radiographic indicator for MRONJ.
Concurrent clinical risk factors for MRONJ during tooth extractions have been recognized, including osteoporotic patients older than 65 years [10, 11], females [26], prolonged ARD therapy [10, 11, 23], rheumatoid arthritis [23], corticosteroid use [9], and mandibular extraction sites [10, 11]. While Jeong et al. identified the mandible as a predisposing arch, no differences were found in dental arch location [10]. Although, the present results did not find a mandibular predilection, a preference for multi-rooted sites over single-rooted teeth was observed. This propensity can be attributed to alveolar socket size. In the absence of severe bone resorption, as seen in our MRONJ + teeth, the wound area can be twice as large in molars compared to canines or incisors [27].
Diverse tooth extraction protocols are reported, which may impact MRONJ development. Like ours, some employ prophylactic antibiotics [19, 26] and discourage discontinuation of ARD treatment [19, 20]. Lesclous et al. agreed that discontinuing ARD is not recommended due to increased fracture risk in the cessation period, especially with denosumab [20]. Our results support the finding that continued ARD treatment does not increase the risk of MRONJ. Besides, while some studies omit primary closure [19, 26], others compare the use of L-PRF and mucoperiosteal flaps [28]. Poxleitner et al. found no significant differences in healing outcomes between L-PRF and mucoperiosteal flap use, suggesting L-PRF as a minimally invasive, efficient, and cost-effective alternative, countering drawbacks of mucoperiosteal flaps such as invasiveness and reduced vestibular depth affecting dental rehabilitation [28]. Complementarily, a meta-analysis involving 2098 subjects found no significant differences in the effectiveness of L-PRF and alveolectomy for MRONJ prevention [25]. Likewise, our study did not demonstrate a significant protective effect of L-PRF use for MRONJ.
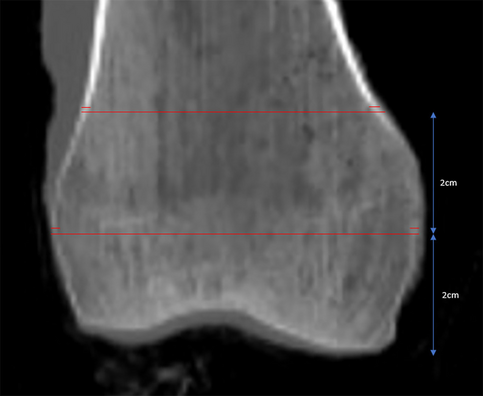
Few radiographic studies exist in osteoporotic patients investigating the local effects of ARDs on jawbones and their relationship with MRONJ. In this context, one of the most researched structures is the mandibular cortical width [14,15,16]. Three-dimensional examinations have revealed a notably thicker MCW in ARD-treated patients compared to controls [15, 16], averaging 4.3 mm and 3.4 mm, respectively [15]. Although, these differences are not evident in panoramic radiographs [14]. Similarly, our findings showed no significant contrasts between ARD-treated patients and the control group, nor was there a correlation between the duration of ARD treatment and the thickness of the MCW. This lack of association might arise from a treatment duration of less than 1 year with ARD in about 20% of the study patients, and from the fact that 25% of the study group and 20% of the control group lacked MCW measurements, as this structure was not visible on their CBCT scans.
One of the novel aspects of the present investigation is the comprehensive assessment of bony changes seen on CBCT images, which has been studied in oncologic patients treated with high doses of ARDs [21, 29] but to a lesser extent in patients treated with low doses. In osteoporotic patients under ARDs, no significant differences in the trabecular bone pattern have been demonstrated in two- [12] or three-dimensional examinations [16] when compared to a control group. Nevertheless, even low doses of ARD demonstrated significantly more thickening of the lamina dura in panoramic radiographs [12]. All findings are corroborated by our current results. In contrast, imaging outcomes related to oncologic ARD doses revealed not only a higher incidence of thickening of the lamina dura but also of osteosclerotic and osteolytic regions [30], which have been identified as local risk factors for MRONJ [30,31,32]. Lesser changes in the radiodensity of the bone trabeculae are consistent with a lower incidence of MRONJ observed in low-dose ARD treatment.
Among the examined radiographic features, only the presence of bone sequesters demonstrated an association with MRONJ development. Notably, all instances of radiographic sequestrum formation in our sample corresponded to sites with osteonecrosis. Two cases exhibited post-operative exposed bone, exceeding eight weeks, while the remaining case displayed histological osteonecrosis. In the latter case, tooth extraction and sequestrum removal within a single surgical procedure were curative, as post-operative bone exposure was absent. Shudo et al. advocated for biopsy during tooth extraction in suspected latent MRONJ cases [19]. Tooth extraction is not the trigger for MRONJ but rather the unveiling factor in these cases. Thus, combining perioperative biopsy and radiographic assessment could promptly identify a latent pathology.
While some studies observed no exposed bone postoperatively, they noted a longer healing period in osteoporotic patients on bisphosphonates [19, 20]. Shudo et al. linked longer bisphosphonate treatment to delayed mucosal healing, particularly beyond 5 years [19]. Similarly, Lesclous et al. found that ARD-treated patients experienced delayed healing, contrasting control healing within 4 weeks [20]. Our results showed controls achieved mucosal healing in an average of 2.6 weeks, whereas ARD-treated patients, whether under bisphosphonates or denosumab, needed 4.4 weeks. Yet, no correlation was found between ARD treatment duration and healing time. Consistently, other studies also found no significant impact of ARD type or treatment duration [28], corticosteroids [19, 20], diabetes [19, 20], smoking [20], number or type of tooth extracted [28], or systemic diseases [28] on socket healing.
This retrospective design inherently holds limitations compared to prospective studies. While efforts were made to match controls, ideally, they would have been drug-naïve osteoporosis or osteopenia patients, which was unattainable. Furthermore, the study’s limited sample size precluded comprehensive exploration of the effects of diverse bisphosphonate types. Additionally, different surgeons with varied experience levels performed the tooth extractions, despite surgeries taking place in the same center under similar protocols and materials. Lastly, due to the lack of histopathological reports, the incidence of MRONJ may be higher in this sample owing to dental infections rather than tooth extractions per se.
In conclusion, osteoporotic patients under low-dose ARDs showed a noticeable thickening of the lamina dura. Corticosteroid intake and the extraction of multi-rooted teeth were identified as risk factors for MRONJ. Sequestrum formation observed on CBCT scans can serve as a strong radiographic indicator of osteonecrosis. In addition, a prolonged post-operative healing period is expected in patients taking antiresorptive drugs, even when there is no development of exposed bone. These results contribute to understanding the effects of ARDs and osteonecrosis in osteoporotic patients undergoing tooth extractions.


Comments (0)