
Remember me




There is research support for IBHC across diverse conditions including anxiety and depression,57,58,59 PTSD,60 substance use,61 chronic pain and opioid use disorders,62,63 and psychotic and bipolar disorders.64,65,66,67 However, the current findings suggest the typical condition-based referral models within IBHC research studies may not represent the complexity of referral decision-making in primary care settings that differ from those frequently represented in IBHC research. The existing guidance that some IBHC models provide may be sufficient for settings that mirror those IBHC research studies or existing standardized IBHC models, like the primary care behavioral health (PCBH) model.27,68,69,70,71 However, in clinical care settings newly developing and implementing IBHC to serve diverse and complex patient populations, the findings indicate that PCPs and behavioral health clinicians would benefit from additional support in making clinical decisions about whether a patient is best served in IBHC or specialty care.
Providers in the GIM and FM clinics at Boston Medical Center had an overwhelmingly positive response to IBHC and believe that IBHC helps better serve patients.40 However, there were notable discrepancies between the patient characteristics described as currently managed versus those described as appropriate for management in IBHC. The present analysis also elucidated the heterogeneity between providers the factors that influenced whether a patient or behavioral health condition was appropriate for management in IBHC. This suggests that IBHC providers could benefit from adaptation and specification of the IBHC model to support clinical decision-making.
Participants identified multiple behavioral health conditions or symptoms and patient characteristics that influence whether a patient is adequately managed in IBHC versus specialty care. This included condition or symptom type, case complexity, duration of care needs, chronicity or acuity, stability, severity, provider comfort-level with managing the condition or symptoms, likelihood of patient engagement, sociodemographic characteristics, and patient preference. A number of these characteristics are consistent with existing literature, both in IBHC and more broadly. For instance, previous research on collaboration between primary and specialty behavioral health care suggests that PCP decisions on whether to manage depression themselves or refer to specialty care depends on severity, complexity, and their own comfort-level with management.72 IBHC research also indicates that the severity of depression symptoms impacts the setting in which a patient demonstrates long-term clinical improvement.73
In addition, some participants reported that IBHC would not be able to provide the necessary support to adequately serve patients struggling with substance use or limited resources. Individuals diagnosed with substance use disorders, unmarried people, and people of color demonstrate lower engagement in IBHC compared to those not diagnosed with substance use, married people, and white people.74 Bias, discrimination, and other structural barriers experienced by patients who use substances, are unmarried, and are not white may drive lower engagement across settings. Findings on IBHC engagement for individuals struggling with housing instability75,76 suggest the feasibility of IBHC for similarly minoritized populations, although more information on its effectiveness is needed.
Given IBHC’s ability to increase engagement in behavioral health services,2,8,9,10,11 patients managing substance use or limited resources (e.g., low-income) would likely benefit from referral to IBHC over specialty care. The contradictory intersection between patient needs and provider ability to manage patients with substance use or limited resources suggests a particular need for standardization and interventions to ensure that the patients who would benefit most from IBHC are not instead referred to specialty care. Because previous training experiences and implicit biases may inhibit provider ability to assess and treat patients in IBHC, standardization of clinical decision-making and training in behavioral health assessment and interventions may support equitable and effective IBHC implementation.
There were inconsistencies in the conditions participants deemed appropriate versus inappropriate for IBHC, and in the characteristics that influenced their referral decision-making. Given the overlap between patient characteristics reported as currently managed and inappropriate for management in IBHC, these inconsistencies likely exist in real-time referral decisions. Without clear guidance about referrals appropriate and inappropriate for IBHC, referral decisions may be based on clinic-specific characteristics rather than existing empirical evidence on the referral decision that will best meet a patient’s unique needs. Thus, heterogeneity in referral decision-making could explain discrepancies between positive IBHC research outcomes and inconsistent findings in real-world implementation.8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31 Standardization of referral decision-making may clarify which patients and what conditions are best managed in IBHC.
Furthermore, the current findings suggest that standardization of referral decision-making should be tailored to dimensional, rather than diagnostic, approaches to referral decision-making. It seems that the more confident providers are in their ability to manage patients within IBHC programs (based on skill, time, clinic resources), the more likely they are to manage them within IBHC. Provider confidence seems to relate more consistently to a provider’s perceived ability to manage the complexity of the case in front of them, rather than the diagnosis. Despite the high frequency of responses related to behavioral health condition or symptom type, high variability in whether providers deemed specific conditions or symptom types appropriate or inappropriate for management in IBHC suggests that condition-based referral decision-making in IBHC may be primarily driven by the interaction between condition complexity and provider confidence in their ability to manage the condition in IBHC, given the extent of patient and setting resources.
Participant responses often demonstrated how interactions between patient and provider characteristics impact referral decisions. For example, some respondents reported that patients with limited resources may be less likely to engage in specialty care and are thus indicated for IBHC, while those with sufficient resources are less indicated for IBHC because they are more likely to engage in specialty care. However, other responses indicate that patients with limited resources need more support than IBHC can provide, while those with sufficient resources may be suitably managed in IBHC.
This split in perspectives emphasizes the competing needs of patients and providers. Patients who providers may feel most confident managing within IBHC (i.e., mild/moderate depression, no comorbidity, high functioning, secure access to resources) may also be those most likely to engage in specialty behavioral health care. However, this may not be the best utilization of specialty care within settings with limited behavioral health resources. Conversely, patients whom providers are least confident they can manage in IBHC (due to acuity, crisis, multiple comorbidities, less access to resources) may be the most in need of IBHC services because of difficulty accessing and engaging in specialty care.
Without guidance about referrals appropriate and inappropriate for IBHC, providers display heterogeneous perspectives about appropriate referrals, suggesting the need for a heuristic to inform guidance specific to local settings so that referrals to IBHC and specialty behavioral health care may best serve patient and provider needs. Based on the complex interrelationships between provider and patient needs (i.e., ability to manage or engage, respectively), Fig. 1 presents an example model heuristic that could guide standardization and implementation of interventions to support more nuanced decision-making for local, real-world settings moving toward integration of behavioral health care. In the model heuristic, the interaction between patient ability and provider ability guides provider decisions. The model heuristic represents how providers approach referral decision-making in primary care clinics at Boston Medical Center, and its dimensional approach may accommodate the unique needs of various local settings in its conceptualization of patient and provider ability. As such, the model heuristic in Fig. 1 may guide provider training and clinical pathway standardization, in which providers receive specific guidance regarding when to refer patients to IBHC or specialty behavioral health care.77,78,79,80
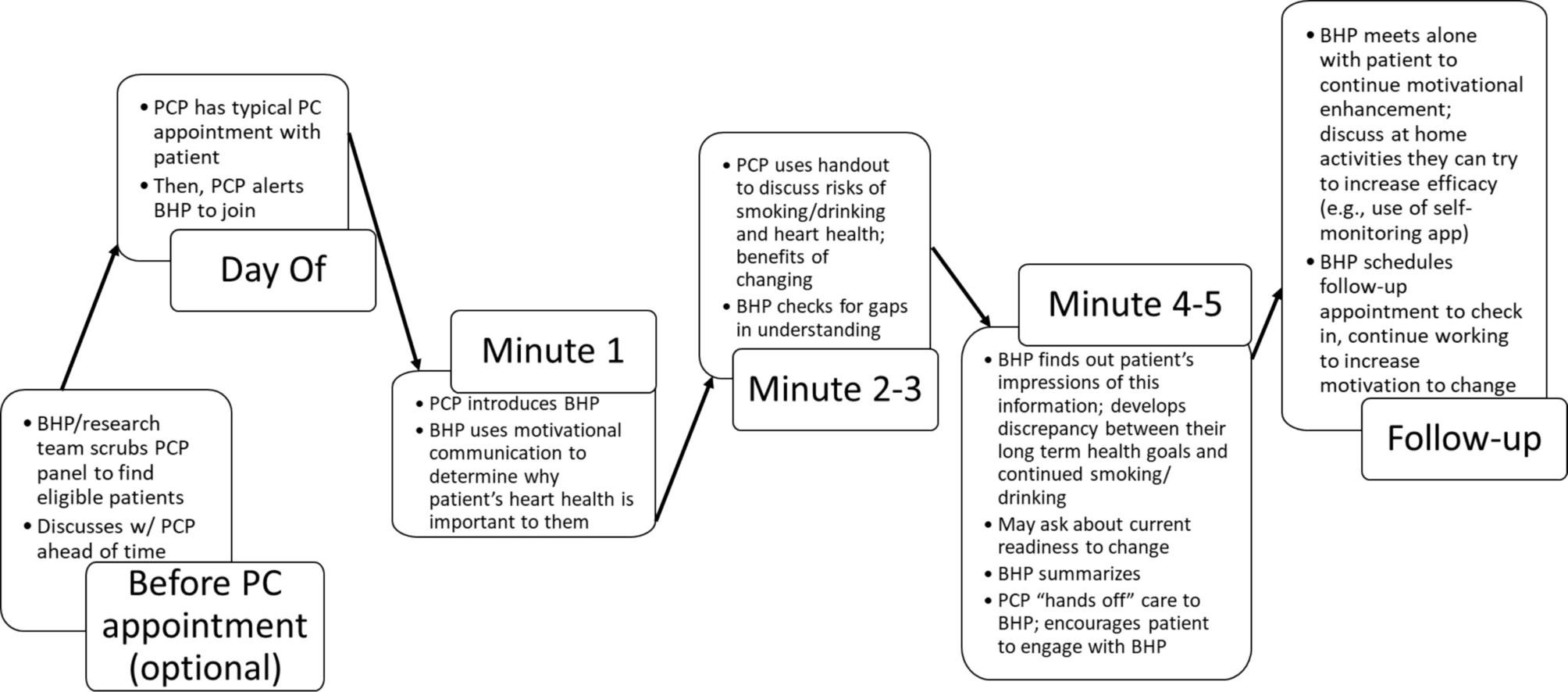
Fig. 1
Model heuristic for clinical decision-making: the interaction of patient and provider ability in determining referral to IBHC or specialty behavioral health care.
Notes. IBHC, integrated behavioral health care; BH, behavioral health. aPatient ability to engage based on resources, history of engagement, preference, condition, or symptom characteristics. bProvider ability to manage patient based on comfort-level managing condition, clinic resources, condition, or symptom characteristics
For example, patients who demonstrate high ability to engage in care who are evaluated by a provider with limited ability to treat their behavioral health condition (e.g., due to lack of training, limited capacity or resources, lack of training in the appropriate intervention) would likely be referred to specialty care. Patients who demonstrate low ability to engage in care who are evaluated by a provider with high ability to treat them would be indicated for IBHC referral. Patient preference or other clinic specific factors could guide referral decision-making for patients with high ability to engage in care who are evaluated by a provider with high ability to treat them. Finally, cases in which patients with low ability to engage in care are evaluated by a provider with limited ability to provide appropriate behavioral health care may require increased provider training or additional case coordination. Training interventions to increase provider ability to manage conditions associated with high patient need (e.g., serious mental illness, substance use) would improve the ability of IBHC to serve patients who would benefit most.
Future DirectionsTo specify how condition characteristics impact a patient's ability to engage and benefit from IBHC, further research on IBHC management of diverse behavioral health conditions with varying levels of acuity and complexity is warranted, focusing on how these variables may moderate IBHC effectiveness. Moreover, future research should leverage mixed method investigation across the condition, patient, and provider characteristics presented here, in both IBHC and specialty care settings, to evaluate IBHC’s effectiveness across the diversity of conditions and symptoms managed in real-world settings.
Future research should also include collaboration with providers in local IBHC settings to further develop tools for referral decision-making standardization that incorporate characteristics most relevant to provider perspectives and patient needs (e.g., Fig. 1). Findings from the present analysis also suggest that increasing provider comfort-level in addressing behavioral health needs could increase the ability of IBHC to manage patients with more challenging and complex behavioral health, if only to help patients get to, and engage in, specialty care. Thus, offering comprehensive and ongoing behavioral health training is essential for expanding the breadth of behavioral health conditions or symptoms managed in IBHC settings.
Moreover, providers and administrator interviews did not speak to the appropriateness of chronic disease and physical health management for referral to IBHC. Some models of IBHC have demonstrated effectiveness in improving indicators of health conditions, like heart disease, diabetes, and chronic pain.15,17,18,19,23 IBHC implementation at Boston Medical Center was limited by a lack of training in health psychology among both primary care and specialty behavioral health providers.48 As more clinics implement IBHC models, there are increasing opportunities for managing chronic health conditions. Future research should focus on training needs for provision of behavioral health care for managing physical health concerns.
IBHC settings in which providers have limited training or comfort-level in managing behavioral health are best positioned to address the high patient ability–high provider ability scenario, which limits access to IBHC and could undermine its intended purpose. Thus, clinical and research efforts should focus on implementing and documenting the impact of increased provider training in IBHC across a variety of behavioral health conditions. It is also important to note that current findings highlight the paradox of stepped-care IBHC models: patients who would benefit the most from IBHC’s potential to improve access and engagement are more likely referred to specialty care due to high care needs, while patients with high ability to access specialty behavioral health care may be considered a better fit for IBHC based on level of care needs. The difference in how patient and provider ability are managed in real-world implementation of IBHC versus the stepped-care model championed by some IBHC researchers further supports the need for more nuanced models in real-world and research settings. These models could encourage, for example, the integration of low-intensity interventions into specialty care and high-intensity interventions into IBHC.
LimitationsDespite the broad implications discussed above, interpretation of these findings is limited by a small sample size, participant self-selection bias, and the uneven distribution of the sample across clinics and participant roles, limiting this study’s ability to compare perspectives between provider types or clinic setting. Nonetheless, sample size was partially determined through theoretical saturation, and sample distribution across roles and clinics is similar to provider and administrator distribution in the local setting.
In addition, the qualitative nature of the present analysis limits the findings to narrative perspectives, which is in line with the researchers’ goal to gain a deep and broad understanding of provider referral. Although the findings include frequency of each subtheme, these should be interpreted with the knowledge that the interviews did not systematically prompt for factors that influenced referral decision-making. Moreover, the present analysis did not aim to assess whether cases were effectively managed in IBHC or in specialty care. Quantitative referral outcome measures could allow future researchers to evaluate real-time referral decision-making and outcomes and inform how standardization may support improved patient outcomes.
The use of “appropriate for IBHC” and “inappropriate for IBHC” represent another limitation. Participants likely used these categories based on the wording of interview questions which used the terms “appropriate” and “inappropriate.” This language is potentially stigmatizing and may not reflect the flexible and interactive nature of referral decisions as described by participants in the present analysis. More inclusive and less rigid language would benefit future research on referral decision-making in IBHC.
Since the collection of these data and in response to researchers’ analyses, several changes have been implemented within the IBHC program of study with the goal of improving the overall success of implementation. Notably, additional stepped-care model-based features have been incorporated to improve referral and engagement in specialty care when needed. In addition, like many institutions, due to COVID-19 there has been massive shifts to telehealth, which has had yet unclear impacts on both IBHC burden and referral practices. Despite limiting generalizability, these changes demonstrate the importance of continual empirical assessment of IBHC implementation to improve adaptation in real-world settings.
Comments (0)