
Remember me


A total of 399 patients with complete medical records were included in this study, including 162 (40.6%) males and 237 (59.4%) females, with a median age at diagnosis of 18.1 months (range: 9.5–31.8 months). In our study, 311 patients (77.9%) were < 3 years old, and 11 (2.8%) were > 7 years old. About half of the patients (200 cases, 50.1%) had an AFP level between 100,000 and 999,999 ng/mL at diagnosis (Table 1).
Table 1 Characteristics of 399 patients with hepatoblastomaStage, pathology, and metastasisPatients were classified by PRETEXT staging at diagnosis, POSTTEXT staging after neoadjuvant chemotherapy, and COG (Evans Surgical) staging after surgery. At diagnosis, 38 patients (9.5%) were in PRETEXT stage I, 139 (34.8%) in stage II, 144 (36.1%) in stage III, and 78 (19.6%) in stage IV. Among all the patients, 327 (82.0%) were positive for one of the PRETEXT annotation factors, including portal vein involvement (P +) (17.0%), inferior vena cava or hepatic vein involvement (V +) (19.0%), extrahepatic tumor extension (E +) (8.5%), and multifocal tumor (F +) (19.8%). After neoadjuvant chemotherapy, 47 patients (47/78, 60.2%) in PRETEXT stage IV were classified as POSTTEXT II (n = 27) and III (n = 21). Two hundred fifty patients (62.7%) were in COG stage I, 24 (6.0%) in stage II, 49 (12.3%) in stage III, and 76 (19.0%) in stage IV.
Half of the patients (227/399, 56.9%) were defined as epithelial subtype, the primary pathological subtypes in the study, which included 4 (1.0%) small cell undifferentiated (SCU) and 98 (24.6%) pure fetal type. One hundred forty-eight patients (37.1%) were defined as mixed epithelial and mesenchymal types, and 18 had no pathological subtypes. Six patients were diagnosed clinically and did not receive delayed operations.
Among the 399 patients, 62 (15.5%) had pulmonary metastasis, 8 (2.0%) had bone metastasis, and 11 (2.8%) had metastasis to the lymph nodes. Two patients (0.5%) had both lung and bone metastasis, and six patients (1.5%) had both lung and lymph-node metastasis.
Treatment path and outcomeThe treatment path and outcome of the 399 HB patients are presented in Fig. 1. A total of 283 (70.9%) received neoadjuvant chemotherapy compared with 116 (29.1%) who underwent primary surgery. Among the 283 patients, 251 patients (88.7%) underwent delayed surgery after chemotherapy, and the remaining 32 (11.3%) did not undergo additional surgical resection. In total, 364 patients received postoperative chemotherapy. One hundred eleven patients suffered from at least one adverse event following chemotherapy, and the most common adverse event was septicemia (41 patients; 10.4%).
Fig. 1
The treatment path and outcome of 399 HB patients. HB hepatoblastoma, PD progressive disease
A total of 367 (367/399, 91.7%) patients underwent surgery, and complete tumor resection was performed in 333 (90.7%) patients. Of the patients who did not undergo surgery, 9 died, 16 had PD, and 7 were lost to follow-up. Among the 367 cases, the resection sites of 105 patients (28.6%) were in the right liver lobe, 57 (15.5%) in the left liver lobe, and 4 (1.1%) in both right and left. The resection site of 67 patients (18.3%) was irregular, and the remaining cases were unknown. After surgery, adverse events occurred in 10 patients, with ascites (6 patients; 1.6%) being the most prevalent side effect (Supplementary Table 2). Twelve patients (3.0%) underwent a second surgery, including one for postoperative complications, four for pulmonary metastasectomy, and seven for recurrent intrahepatic tumor resection.
Thirty-nine patients who did not achieve complete remission after first-line treatment (chemotherapy combined with surgery) were treated with a “second-line therapy,” which consisted of transarterial chemoembolization (TACE) (n = 31), radiofrequency ablation (RFA) (n = 3), and high-intensity focused ultrasound (HIFU) (n = 5).
At the end of the follow-up, 299 (299/399, 74.9%) patients had complete remission, 24 (6.0%) patients died, 17 for primary disease, 5 for relapse, and 2 for adverse effects. Twenty patients had relapses, 4 for pulmonary relapse, and 17 for liver relapse. Sixteen (4.0%) patients had PD, and 25 patients (6.27%) were lost to follow-up.
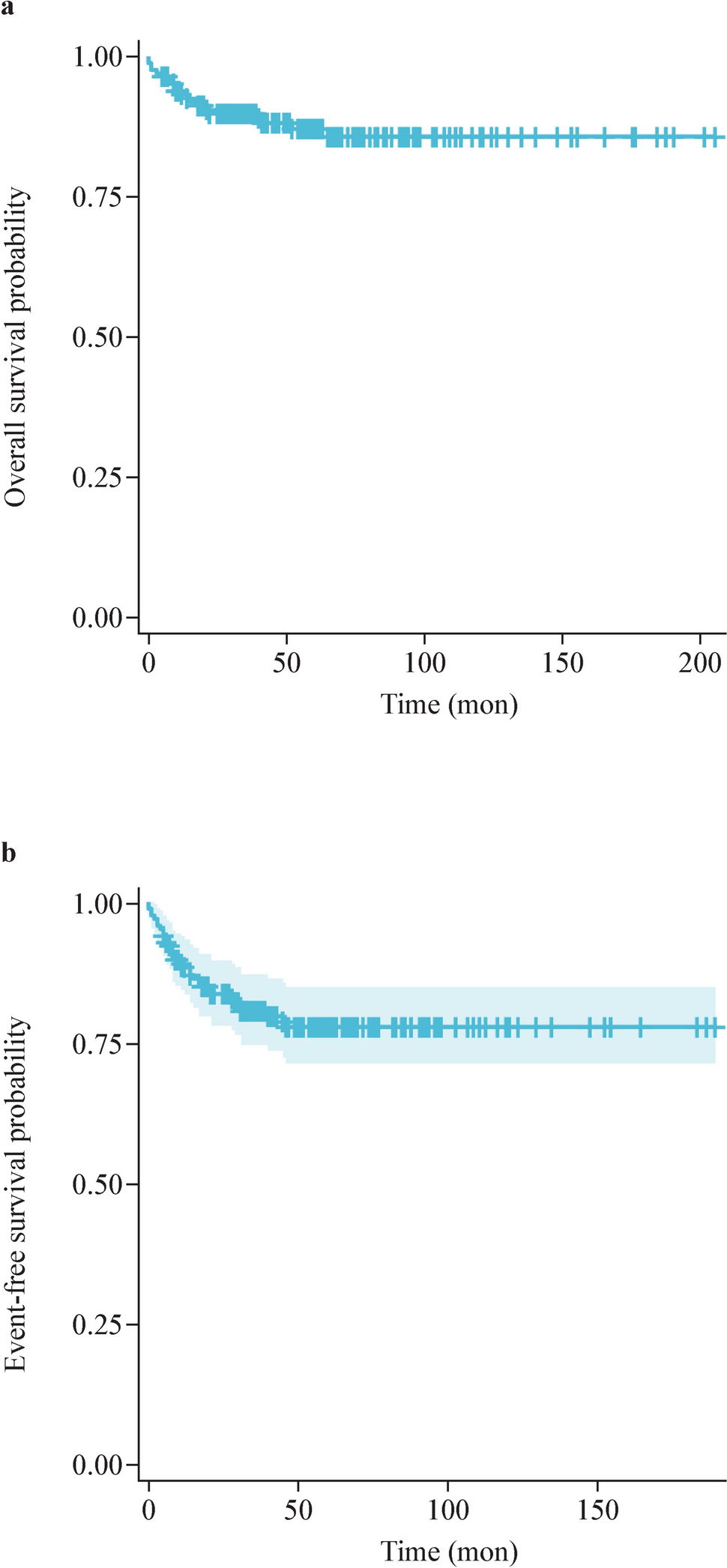
Survival and prognostic factorsThe 4-year EFS was 76.9% [95% confidence interval (CI) 72.8–81.2%], and the 4-year OS was 93.5% (95% CI 91.0–96.1%). The 4-year EFS for patients in the very-low-risk group, low-risk group, intermediate-risk group, and high-risk group was 100.0%, 91.6% (87.3–96.1%), 81.7% (75.0–89.1%), and 51.0% (42.6–61.1%), respectively. The 4-year OS for the corresponding risk groups were 100.0%, 97.3% (94.7–100.0%), 94.4% (90.1–98.9%), and 86.8% (80.6–93.5%), respectively. The survival rates for PRETEXT, COG stage, and CHIC and risk group are detailed in Fig. 2 and Table 2.
Fig. 2
The event-free survival (EFS) and overall survival (OS) of 399 HB patients treated with CCCG-HB-2016 protocol under different risk stratification system. a The EFS and OS for all the 399 HB patients. b, c The OS and EFS of 399 HB patients with different PRETEXT stages. d, e The OS and EFS of 399 HB patients with different COG Evans stages. f, g The OS and EFS of 399 HB patients with different CCCG-HB-2016 risk stratification. h, i The OS and EFS of 399 HB patients with different CHIC risk stratification. CCCG Chinese Children’s Cancer Group, HB hepatoblastoma, PRETEXT pre-treatment extent of tumor, COG Children's Oncology Group, CHIC Children’s Hepatic Tumors International Collaboration
Table 2 Comparison of the EFS and OS in patients with hepatoblastoma based on different stratificationThe prognostic factors, including age, AFP level at diagnosis, pathological subtypes, PRETEXT stage, PRETEXT annotation factors (VPEFR), POSTTEXT stage, COG stage, and metastasis at onset, were analyzed in our study. The survival rates and hazard ratios are shown in Table 2.
Multivariable cox regression analysis revealed that compared with age [3–7 years vs. < 3 years, hazard ratio (HR): 5.428, 95% CI 1.523–19.345; P = 0.009], E + (HR: 3.975, 95% CI 1.033–15.286; P = 0.045) and tumor rupture (R +) (HR: 7.044, 95% CI 1.784–27.806; P = 0.005) were independent risk factors for OS (Supplementary Table 3).
Second-line treatment for patients (hepatoblastoma)The propensity score matching (PSM) method was used to explore the impact of second-line therapies on survival. This was calculated by a logistic regression model with the following covariates: age, sex, and CCCG-HB 2016 risk stratification. The matching was performed using a 1:4 nearest-neighbor matching protocol with a caliper width of 0.2. The results showed that the 4-year EFS and OS of patients (n = 34) with second-line therapy were lower than those of patients who did not receive additional treatment (n = 129). However, this difference was not statistically significant (4-year EFS, P = 0.072; 4-year OS, P = 0.255) (Supplementary Fig. 2).
Correlation between declining alpha-fetoprotein with event-free survival and overall survival rateThis study found that the AFP level of HB patients continued to decline with the progression of treatment (Supplementary Fig. 3). By analyzing the relationship between the declining AFP during different treatment periods and patient prognosis, we found that the declining percentage of AFP after the first two cycles of neoadjuvant chemotherapy was positively correlated with EFS. Therefore, we further explored the relationship between AFP and EFS and established that AFP decline > 75% was statistically associated with EFS (Table 3). In addition, a stratified analysis with a 75% decrease in AFP as the cut-off value showed that patients with an AFP decline > 75% after the first two cycles of neoadjuvant chemotherapy had better EFS and OS than those with ≤ 75% (Fig. 3).
Table 3 Stratification analysis of the association between AFP decline percentage after two cycles of neoadjuvant chemotherapy and EFSFig. 3
Correlation of AFP decline percentage with EFS and OS (n = 197). AFP alpha-fetoprotein, EFS event-free survival, OS overall survival, CT chemotherapy
Comments (0)