Study design and participants
This was a single-center, randomized, double-blind, sham-controlled trial conducted at Xuanwu Hospital, Capital Medical University. The trial was registered at www.clinicaltrials.gov (unique identifier: NCT03821181), approved by the Ethics Committee of Xuanwu Hospital of Capital Medical University, and conducted in compliance with the ethical principles of the Helsinki Declaration. All participants or their legally authorized representatives provided informed consent before enrollment.
The inclusion criteria were: (1) aged 4 to 14 years; (2) undergoing digital subtraction angiography (DSA) and meeting the MMD diagnostic criteria recommended by the Research Committee of the Ministry of Health and Welfare of Japan [17]; (3) patients with no history of TIA, ischemic or hemorrhagic stroke, or involuntary movements attributable to MMD, which may involve nonspecific symptoms such as headaches, dizziness, cognitive decline, and emotional changes [18, 19]; (4) cerebral vascular reserve detected by single-photon emission computed tomography showing no severe impairments; (5) no neurologic deficits on physical examination; and (6) informed consent provided by a legal representative.
The exclusion criteria were: (1) previous cerebral revascularization; (2) secondary moyamoya phenomenon caused by sickle cell disease, neurofibromatosis type 1, cranial therapeutic irradiation, Down syndrome, congenital cardiac anomaly, renal artery stenosis, giant cervicofacial hemangiomas, and hyperthyroidism; (3) mental disorders that could mimic nonspecific moyamoya symptoms, such as schizophrenia, anxiety, mood disorder, bipolar disorder, and psychoactive substance abuse; (4) unlikely to be available for follow-up over 1 year; (5) severe hepatic or renal dysfunction; and (6) any of the following cardiac diseases: mitral and/or aortic stenosis, patent foramen ovale, bacterial endocarditis, or any other cardiovascular condition interfering with participation.
Randomization and masking
Patients diagnosed with MMD by DSA were recruited, and baseline assessments were performed. Patients were then randomly assigned to the RIC or sham RIC group at a ratio of 1:1. Randomization was performed using opaque and sealed envelopes that contained the group allocation. The randomization numbers were computer-generated with a block size of six. An investigator who was not involved in the study design or data analysis opened the envelopes to the participants. All the participants, investigators, and examiners were blinded to the treatment assignments.
Interventions
All enrolled patients underwent risk factor management and lifestyle guidance, including antiplatelet therapy, appropriate blood pressure control, avoiding hot meals (noodles, soup, etc.), strenuous exercise, playing wind instruments (such as flutes), and blowing balloons [20]. In addition, all participants were asked to complete either the RIC or sham RIC treatment twice daily for one year. The RIC protocol involved five cycles of bilateral upper arms with 5-minute inflation to 50 mmHg above systolic blood pressure alternating with 5-minute deflation using an automated device, whereas the sham RIC protocol involved five cycles of bilateral upper arms with 5-minute inflation to 30 mmHg alternating with 5-minute deflation. After completing the one-year RIC or sham RIC treatment, the participants were not permitted to continue the intervention.
An electronic autocontrol device (Xuanyitong, Beijing Renqiao, China) was used for the RIC and sham RIC procedures. Electronic devices were equipped with subscriber identity module cards containing patient-specific identification numbers and RIC implementation dates, which were linked to a background monitoring platform. To ensure RIC compliance, the background monitoring platform automatically reminded the patients if treatment had become interrupted for three consecutive days. The investigators were alerted when the RIC was interrupted for four consecutive days. This information was documented on a background monitoring platform. A “grace” period of one session of RIC was assessed to be approximately four days [21]. Compliance of one month was considered substandard if a patient interrupted RIC or sham RIC treatment for four consecutive days of the month.
Follow-up
After the intervention began, clinical events were followed up for three years. All enrolled participants were required to undergo monthly follow-ups, or when necessary during the first year, and every two months, or when necessary, thereafter. During these visits, the patients were questioned about the occurrence of stroke or TIAs, revascularization surgery, RIC, current medications, management of cerebrovascular disease risk factors, and any other discomfort. The patient global impression of change (PGIC) assessment was performed both at the beginning and the end of the intervention. This information is recorded in the database.
Outcome assessmentEfficacy
The primary outcome of this study was the cumulative incidence of major adverse cerebrovascular events (MACEs). MACEs were defined as the occurrence of stroke, recurrent transient ischemic attacks (≥ 2 attacks), or need for revascularization surgery as determined by the treating team. If participants experienced a stroke, recurrent TIAs, or revascularization surgery, any of these events were considered as MACE. Ischemic stroke occurrence refers to a new cerebral infarct lesion detected by diffusion-weighted imaging (DWI) or fluid-attenuated inversion recovery (FLAIR) weighted sequencing. Hemorrhagic stroke was diagnosed when DWI- or FLAIR-weighted sequences showed new hemorrhagic or high-density lesions on computed tomography (CT). TIA events were defined as neurological symptoms and signs that resolved spontaneously within 24 hours after onset, without evidence of infarction on magnetic resonance imaging (MRI) or CT. The decision for revascularization was made by neurosurgeons with experience in vascular reconstruction techniques. This decision was based on comprehensive evaluations of the patient’s condition and the willingness of the patient’s guardian to operate.
Secondary outcomes included the rates of ischemic stroke, recurrent TIAs, hemorrhagic stroke, revascularization surgery, and improvement in PGIC scales at follow-up assessment. The PGIC scale was used to assess the occurrence or progression of nonspecific symptoms and cerebrovascular events associated with MMD. The PGIC consists of a 5-point scale (1 = significant reduction or elimination of symptoms, 2 = mild attenuation, 3 = no change, 4 = mild deterioration, and 5 = significant deterioration). A significant reduction or elimination of symptoms was regarded as clinical improvement. Changes in overall symptomatology were recorded at outpatient follow-up.
Safety
Safety measures in this study were assessed based on the presence of upper limb injury, including local edema, petechiae, ecchymosis, skin lesions, and any adverse events related to RIC. These were assessed by two independent examiners who were blinded to the treatment assignments. Any differences in these assessments were resolved by attempting to reach an agreement between the examiners. If no consensus was reached, a third examiner performed the final assessment.
Cerebral hemodynamics evaluation
Transcranial Doppler (TCD) is a useful tool for evaluating and monitoring patients, as well as detecting unstable diseases [22, 23]. It is a noninvasive, low-risk, bedside technique that enables real-time characterization of cerebral hemodynamics. However, there is no exact numerical method to judge the instability of cerebral hemodynamics, given the relative rarity of cerebrovascular disorders in children and the age-related changes in cerebral hemodynamics.
This study evaluated patients using baseline Suzuki stages on cerebral angiography and TCD parameters, based on previous TCD research findings in pediatric patients [23, 24]. A prospective study showed that the mean cerebral blood flow velocity of the middle cerebral artery (MCA) by TCD in patients with MMD ≤ 21 years old was 159 cm/s [23]. In this study, we statistically analyzed the MCA with a baseline mean velocity ≥ 159 cm/s. All tests were conducted using a Hitachi Aloka Arietta 70 (2.0 MHz transducer) ultrasound machine. Measurements were performed only once for each vessel because pediatric patients could not tolerate prolonged examinations, including peak systolic velocity (PSV), end-diastolic velocity (EDV), and mean velocity (MV).
Statistical analysis
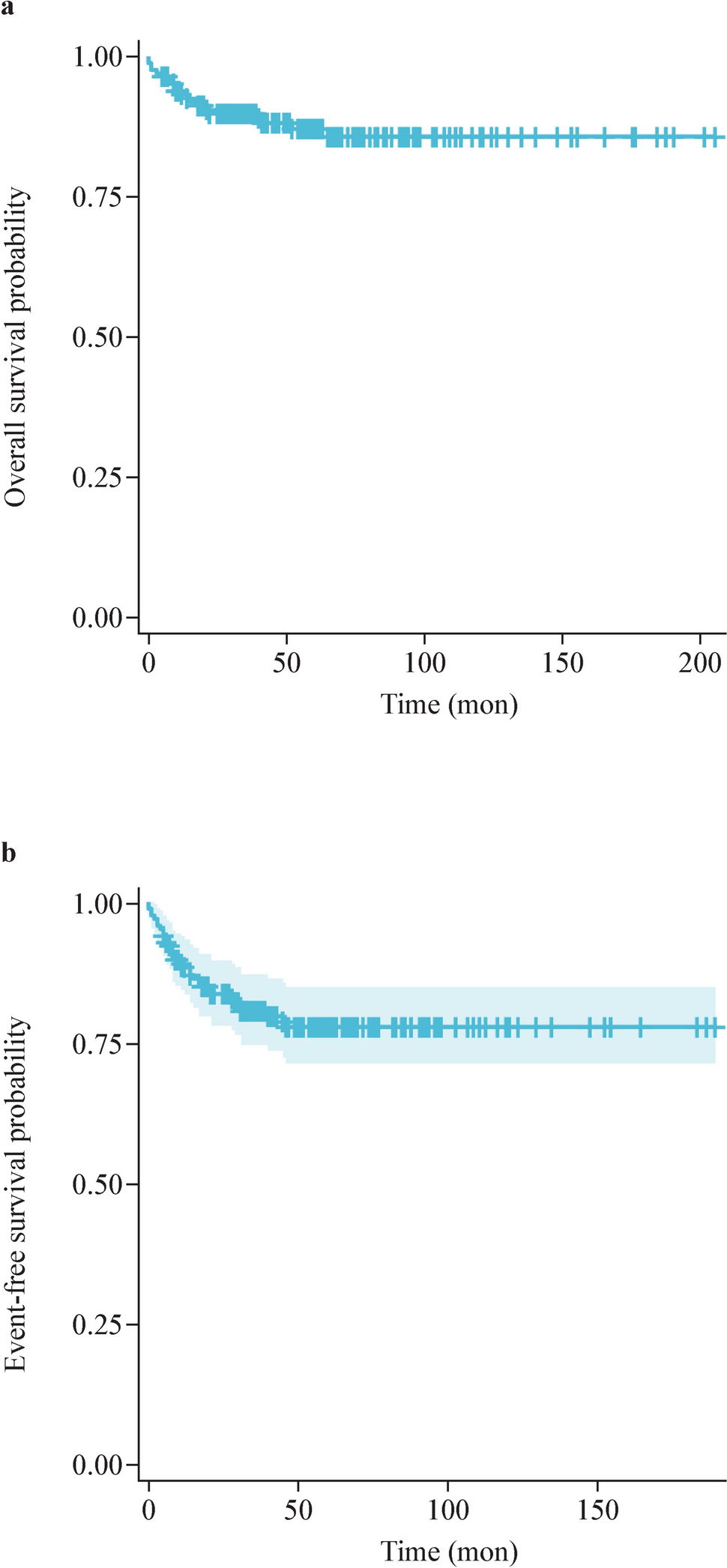
This was a pilot randomized controlled study. No parameters were used to estimate the sample size. However, in a pilot study, Hertzog et al. showed that 10–20 participants per group were adequate to assess feasibility [25]. Twenty patients per group were, therefore, planned, and 46 patients were eventually selected for this study. To compare the characteristics of the RIC group with the control group at baseline and follow-up, continuous variables were analyzed using the independent Student’s t test or the Mann–Whitney U test and expressed as mean ± standard deviation or medians [interquartile ranges (IQRs)]. Categorical variables were analyzed using the χ2 test or Fisher’s exact test and shown in proportions. The cumulative incidence of MACEs for time-to-event variables was obtained using Kaplan–Meier estimates. All data were analyzed using SPSS (version 24.0; IBM Inc.), with the significance level set at P < 0.05. Kaplan–Meier curves were constructed using Prism (version 8.02; GraphPad Software Inc.).



Comments (0)