
Remember me




This study analyzed cross-sectional data collected as part of a randomized controlled trial that compared the Fittle Senior System (FSS), a digital physical activity intervention with social support features drawing on social cognitive theory [9, 18], with a digital educational control. The study protocol is summarized briefly below.
ProtocolParticipants were enrolled at two academic medical centers in the United States. Following telephone pre-screening and informed consent, participants were assigned randomly in blocks of 3–6 individuals to receive either the FSS or an educational control. FSS arm participants received a tablet delivering pictorial and written instructions on physical exercises over a 12-week period, with team-based social support features in the form of 1-to-1 and group chat functions. Participants randomized to the educational control received a tablet preloaded with widely available content on physical exercise and safety tips.
SampleEligible participants were ≥ 60 years of age and able to speak English, read at the sixth-grade level, and pass the Telephone Interview for Cognitive Status [19]. Individuals with cognitive (defined by score < 26 on the Mini Mental Status Exam [20]) or visual (corrected or uncorrected visual acuity < 20/40) impairment, active participation in a structured physical exercise regimen, or health conditions that could affect their ability to participate were excluded. Recruitment was conducted through classified advertisements, virtual flyers, community newsletters distributed at senior centers and in geriatric clinics, virtual presentations, and social media advertisements.
MeasuresMultiple measures were collected as part of the parent randomized controlled trial. Measures relevant to the current study are described below.
General healthGeneral health was measured using the first question of the 36-Item Short-Form Survey (SF-36): “In general would you say your health is…?” Scores range from 1 (“excellent”) to 5 (“poor”) [21]. Due to use of a single measure, Cronbach’s alpha for general health could not be calculated.
Social supportSocial support was measured using the 12-Item Interpersonal Support Evaluation List [22]. According to this scale, social support is measured across 3 subscales: appraisal, belonging, and tangible. Each item is scored on a 1 (“definitely false”) to 4 (“definitely true”) scale, including reverse coding for some prespecified items. We have reported the mean score, with a higher mean corresponding with more social support. In our sample, Cronbach’s alpha for social support was 0.87.
Physical activityPhysical activity was measured using the Global Physical Activity Questionnaire [23]. This 16-item scale assesses physical activity across multiple domains, including activity performed at work, during travel to and from places, and recreational activities, as well as sedentary behavior. Physical activities are clustered into moderate and vigorous physical activities, and physical activity levels are expressed as the total number of metabolic equivalent (met)-minutes per week. Attainment of ≥ 150 minutes of moderate-intensity or 75 min of vigorous-intensity physical activity per week or ≥ 600 metabolic equivalent-minutes per week of moderate and vigorous physical activity is consistent with adherence to United States Centers for Disease Control and the World Health Organization physical activity guidelines [2, 3]. Sedentary behavior based on the Global Physical Activity Questionnaire is expressed in terms of minutes per week [23]. World Health Organization physical activity guideline recommendations advise limiting sedentary activities without defining a specific goal threshold [3]. In a recent systematic review, reliability and validity of the Global Physical Activity Questionnaire were found to vary based on study population [24]. In our sample, Cronbach’s alpha for physical activity was 0.51.
Sociodemographic characteristicsSociodemographic and related features, including age, gender, race, ethnicity, and comorbid conditions, were collected by self-report.
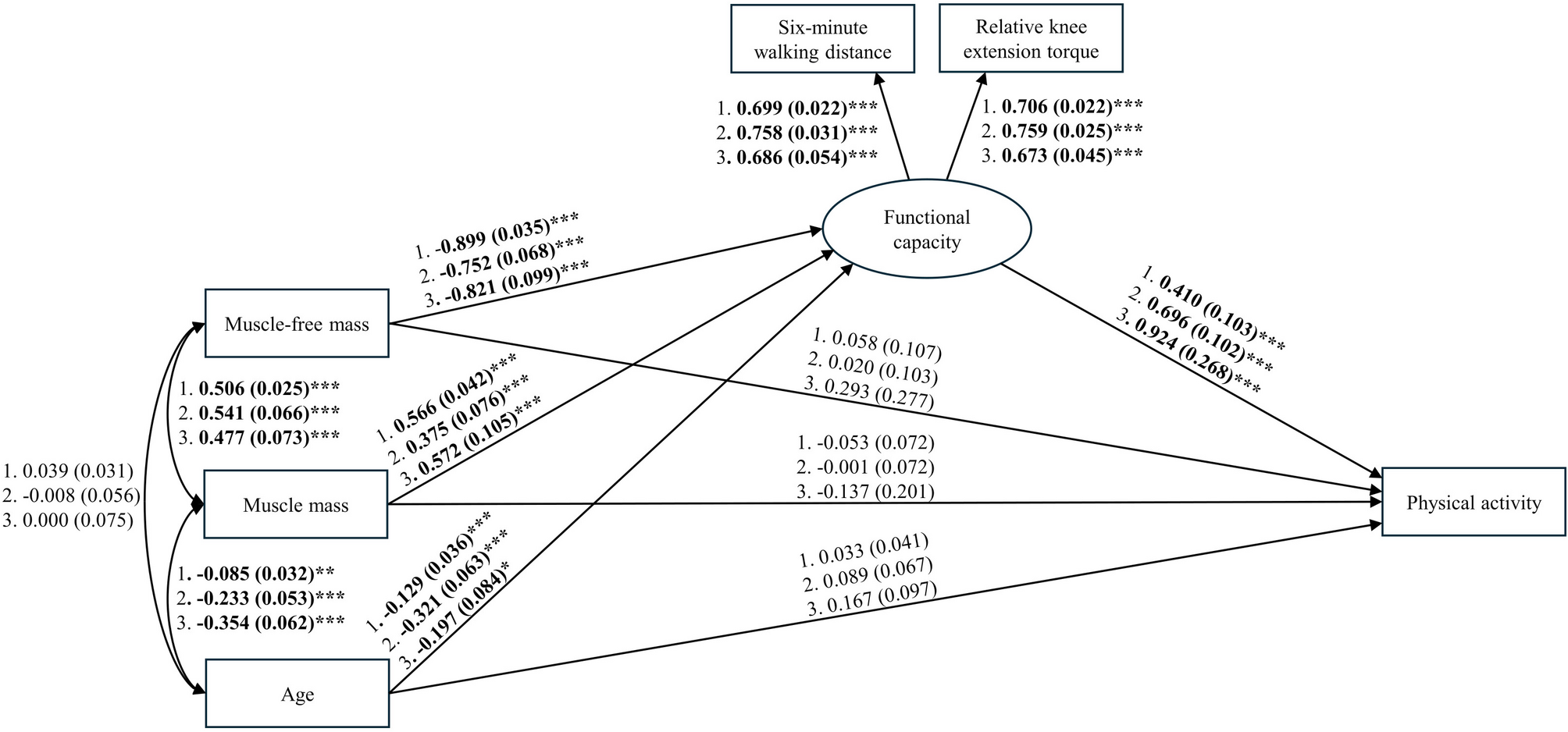
AnalysisSample characteristics were summarized using descriptive statistics. Participants without complete data were excluded from subsequent analyses. Pearson and point-biserial correlations were computed to evaluate the relationship between self-reported physical activity and self-reported general health, social support, and sociodemographic and related features. For the main analysis, we conducted a mediation analysis with bootstrap confidence intervals. We incorporated social support (exposure), self-reported general health (mediator), self-reported physical activity (outcome), and the sociodemographic features of age, gender, and race and ethnicity (covariates) into the mediation model determined a priori based on review of the literature [11]. Figure 1 shows the mediation model. For model estimation, 5000 bootstrap samples were employed to attain 95% confidence intervals, which were deemed significant if they did not overlap with 0. SPSS Statistics 29 was used for statistical analysis.
Fig. 1
Mediation model relating social support and self-reported general health to self-reported physical activity. Parameter displayed is the standardized beta coefficient. Asterix reflects a statistically significant path based on bootstrap confidence interval
Comments (0)