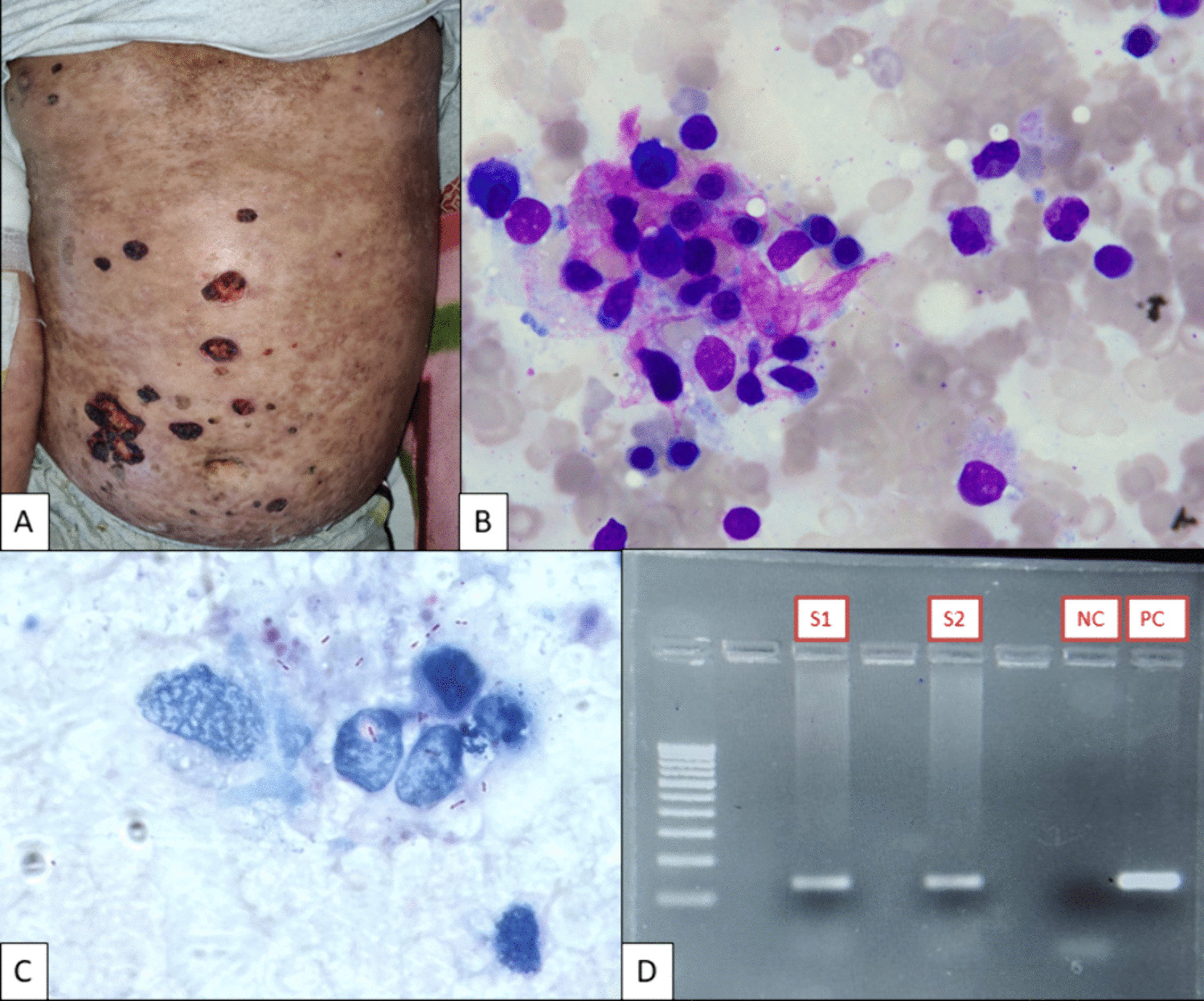
ALK + LBCL is a distinct, rare, and aggressive type of large B cell lymphoma, which typically presents in lymph nodes, most commonly the cervical [7, 8, 11, 15, 16]; however, extranodal sites are also affected. There is a wide age range at presentation with a median of 35–38 years and a male predominance. Patients present with high stage disease in most cases with median survival of 11–24 months [4, 6, 8]. There is no known association with immunodeficiency or viral association including Epstein Barr virus, HHV8, or HIV. Architecture of the lymph node is diffusely effaced but often shows a partial sinusoidal pattern. Cellular morphology appears immunoblastic and/or plasmablastic [7, 8, 11, 15]. Rarely large Reed-Sternberg-like cells can be present [7]. There is increased mitotic activity and can be necrosis. Our case showed effaced architecture with the neoplastic cells showing a plasmablastic appearance.
Immunohistochemistry evaluation of the neoplastic cells in ALK + LBCL shows expression of plasmacytic markers including CD138, MUM1, CD38, and VS38. CD20 is often negative or weakly positive in a minority of cases. Other B cell antibodies including CD19 and CD22 are negative. PAX5 and CD79a are seen in a minority of cases. Other stains, which may be positive, include EMA, BOB-1, OCT-2, and CD45RB (may be weak). Cytoplasmic immunoglobulin most often IgA can be positive. CD10, MYC, and STAT3 can be positive. Lineage-specific T cell antigens and T cell-associated antigens are generally negative; however, CD4, CD57, and CD43 expression is reported in approximately half of cases. Immunohistochemistry in our case was compatible with ALK + LBCL, but the cells demonstrated partial CD3 expression, a finding that has been reported in only rare cases [9, 12]. EBV is almost uniformly negative, although rare cases have been positive [14]. CD30 is negative in the majority of cases.
All cases express ALK protein or contain the ALK translocation [9]. The staining pattern of ALK is most often in a cytoplasmic granular pattern; this expression pattern is the result of the lymphomagenic translocation ALK::CLTC [t(2;17)(p23;q23)] in the majority of cases. Other translocation partners include NPM1, SEC31A, SQSTM1, RANBP2 GORASP2, EML4, and IGL; these translocations can give distinct staining patterns [7]. Our case shows cytoplasmic granular ALK staining. ALK by FISH was disrupted in our case; however, the partner gene cannot be determined in the FISH assay and NGS was not performed. FISH for BCL2, BCL6, and MYC were intact.
Aberrant T cell-specific markers expressed on LBCL have been reported, most notably CD5, but other markers including CD2, CD4, CD7, and CD8 have also been reported [18, 19]. Aberrant CD3 on LBCL is unusual but is reported sporadically [18,19,20,21,22]. Some cases with CD3 expression on LBCL have been associated with EBV [13] leading to speculation that EBV may promote linage infidelity; however, EBV is not uniformly present, and our case does not express EBER. Expression of more than one T cell-specific or associated marker is seen in rare cases of LBCL. The biologic significance is unknown in cases of LCBL with aberrant CD3 due to their rarity [13, 19, 20].
ALK + LBCL has not been studied extensively with IGH and TCR previously, but in studies where IGH and TCR rearrangements were performed, no TCR clonal rearrangement was identified; however, no case showed CD3 expression in these studies [8, 11]. Coexisting IGH and TCR clones in gene rearrangement studies is not previously reported, but there are limited studies looking at TCR rearrangements in ALK + LBCL. Although our case may be considered “borderline” in some laboratories due to the apparent polyclonal background, the TCR assay was read as clonal following the manufacturer’s instructions. The source of this peak may derive from the focal neoplastic cells, which express aberrant CD3 or conversely, the peak may derive background T cells reacting to the neoplastic B cells. It has also been documented that false positive TCR rearrangements can occur in B cell lymphomas and reactive processes using BIOMED-2 assays [23, 24]. Although theoretically TCR gamma and TCR beta assays together could be used to confirm the clone, both may sometimes be clonal in the same reactive process [23]. Although the source and significance of the T cell peak in our case is uncertain, the utility of BIOMED-2 assays is well documented, and this assay is standard worldwide but caution in reading the assay should be observed.
In conclusion, we present a case of ALK + LBCL with aberrant expression of CD3 and gene rearrangement of both IGH and TCR. A panel of immunohistochemistry markers including multiple T cell, B cell, and plasmacytic markers was necessary to characterize the lymphoma, which is recommended when lineage-specific antigen expression is ambiguous. Because aberrant expression of CD3 is rare in ALK + LBCL, we performed IGH and TCR to help delineate lineage of this ALK + LBCL, testing which may be helpful particularly if aberrant T cell markers are expressed. However, as this case illustrates, gene rearrangement studies should be interpreted with caution and considered within the clinical and pathologic context. The clinical behavior of our case of ALK + LBCL is uncertain due to the rarity of aberrant CD3 in this entity and the lack of clinical follow-up information. The clinical behavior may not differ from conventional cases of ALK + LBCL; however, further study is necessary.










Comments (0)