
Remember me

A 30-year-old man was admitted to a nearby hospital for acute decompensated heart failure. On admission to that hospital, echocardiography showed that the left ventricular end-diastolic diameter (LVDd) was 62 mm and left ventricular ejection fraction (LVEF) was only 17%. The patient had left and right ventricular enlargement, moderate mitral regurgitation (MR), and moderate tricuspid regurgitation (TR). Tricuspid annular plane systolic excursion (TAPSE), a measure of right heart systolic function, was reduced to 10 mm. He was diagnosed with dilated cardiomyopathy based on normal coronary angiography findings and myocardial pathology examination of a right ventricular myocardial biopsy. The patient experienced cardiogenic shock, which was caused by acute decompensated heart failure associated with dilated cardiomyopathy. This was his first admission for a heart condition. Inotropic drugs (dobutamine 4.0 µg/kg/min, milrinone 0.25 µg/kg/min) were administered, but his symptoms did not improve. Thus, intra-aortic balloon pump (IABP) was added for more support and the patient was transferred to our hospital (day 1).
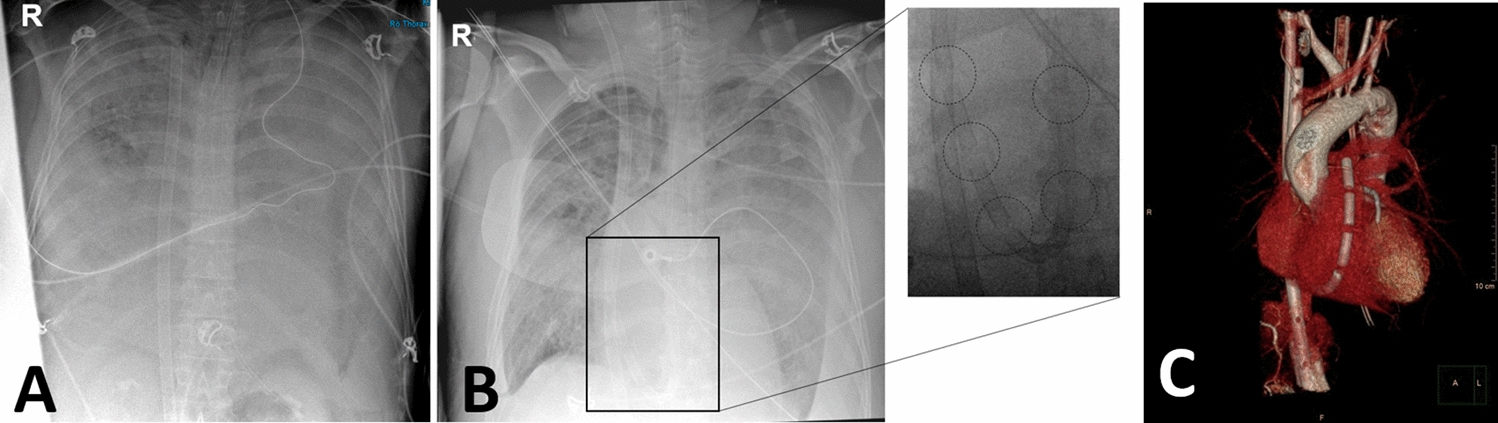
After transfer to our hospital, the patient’s height, weight, and body surface area were 165 cm, 72 kg, and 1.79 m2, respectively, and echocardiography showed an LVDd of 64 mm and an LVEF of 23% on day 1. Even with IABP support, his systolic blood pressure was still below 80 mmHg and he was not hemodynamically stable, with hepatic dysfunction (aspartate aminotransferase, 37 U/L; alanine aminotransferase, 90 U/L; γ-glutamyltranspeptidase, 73 U/L; total bilirubin, 3.7 mg/dL) and renal dysfunction (blood urea nitrogen, 22.0 mg/dL; creatinine, 1.11 mg/dL; estimated glomerular filtration rate, 65.2 mL/min/m2) observed on day 6. Owing to worsening of the patient’s hemodynamic status by infection at the catheter site on day 6, we upgraded the mechanical circulatory support (MCS) from IABP to Impella CP (Fig. 1), which was placed via the left femoral artery approach on day 6. Given his relatively small stature, we determined that the Impella CP would be sufficient for MCS. After replacing the IABP with the first Impella CP, LVDd was 60 mm and LVEF was 12% on day 6. We used the recommended purge solution composition (heparin 25 U/mL, 5% dextrose solution), and the purge flow rate was approximately 14.9 mL/h. Meanwhile, the platelet count decreased steadily from 162,000/L at the time of transfer to 31,000/L on day 9, and laboratory data revealed platelet-activated anti-platelet factor 4/heparin antibody > 5.0 U/mL (normal range < 1.0 U/mL) (Fig. 2). Heparin had been used before the patient was transferred to our hospital, and after his transfer, heparin was continued. Therefore, this event occurred on day 15 of heparin use. The 4Ts Score of 6 points (Thrombocytopenia, 2 points; Timing of platelet count fall, 2 points; Thrombosis of other sequelae, 1 point; Other causes of thrombocytopenia, 1 point) indicated a high possibility of HIT (6 points). Finally, the diagnosis of HIT was confirmed by a hematologist. As systemic anticoagulation therapy, heparin (10,000–15,000 U/day) was used until HIT was identified. After the discovery of HIT, argatroban (0.3–0.35 µg/kg/min) was used for systemic anticoagulation.
Fig. 1
Trends in Impella purge flow and pressure. BBPS, bicarbonate-based purge solution; DOB, dobutamine; HIT, heparin-induced thrombocytopenia; MCS, mechanical circulatory support; MIL, milrinone; NAD, noradrenaline; VA-ECMO, veno-arterial extracorporeal membrane oxygenation
Fig. 2
Trends in blood lactate dehydrogenase, hemoglobin, and platelet count. BBPS, bicarbonate-based purge solution; Hb, hemoglobin; HIT, heparin-induced thrombocytopenia; LDH, lactate dehydrogenase; MCS, mechanical circulatory support; Plt, platelet; VA-ECMO, veno-arterial extracorporeal membrane oxygenation
After changing to argatroban as the alternative purge solution (argatroban 0.05 mg/mL, 5% dextrose solution) on day 14, the purge flow showed an abrupt decline to 9.2 mL/h, and a high risk of emergency shutdown of the Impella CP pump was indicated. Therefore, we changed the device to Impella 5.0 (Fig. 1), which was placed via the right femoral artery approach on day 14. We choose Impella 5.0 instead of Impella 5.5 because the subclavian artery diameter was only 6.5 mm on blood vessel echocardiography and computed tomography, which would have made the Impella 5.5 approach challenging. After switching to Impella 5.0, LVDd was 59 mm and LVEF was 18% on day 14. However, the purge flow of Impella 5.0 again showed a decline to 5.5 mL/h on day 18, likely owing to Impella pump thrombus, so we switched the device to the second Impella CP, which was placed via the left femoral artery approach on day 18. We also changed the purge solution from an argatroban solution to the BBPS (25 mEq/L sodium bicarbonate, 5% dextrose solution). After switching Impella 5.0 to the second Impella CP, LVDd was 66 mm, LVEF was 21%, and TAPSE was 12.6 mm on day 18. After switching to BBPS, the purge flow of Impella CP could be sustained for more than 7 weeks. The purge flow and pressure were approximately 9–12 mL/h and 400–500 mmHg, respectively. As well as MCS by Impella CP (2.5 L/min), inotropic drugs were used. However, the cardiac index was 1.6 L/min/m2, mixed venous oxygen saturation was 59%, and mean blood pressure was 70 mmHg. Moreover, there was progression to multiorgan damage with hepatic dysfunction, renal dysfunction, and decreased urine output (20–30 mL/h), and the patient was determined to be in a low cardiac output state.
Therefore, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) was added as MCS via the left femoral arteriovenous approach, along with the third Impella CP (Fig. 1) placed via the right subclavian artery approach on day 24 to maintain systemic hemodynamics. After the addition of VA-ECMO support, the patient’s circulatory status stabilized and was maintained at an approximate Impella CP pump flow of 2.1 L/min and VA-ECMO flow of 3.3 L/min. As a result, the cardiac index increased to 2.0 L/min/m2, mixed venous oxygen saturation increased to 80%, and mean blood pressure increased to 78 mmHg. Organ damage improved and urine output increased (60–80 mL/h). On day 24, LVDd was 60 mm, LVEF was 23%, and TAPSE was 15.2 mm. Thereafter, LVDd, LVEF, right ventricular contraction, and degree of MR and TR were maintained without deterioration under stable MCS with the use of BBPS. Despite the addition of VA-ECMO to Impella CP as MCS, there was no exacerbation of hemolysis, and the patient could be managed for approximately 1 month (Fig. 2). There were no adverse events associated with BBPS, such as alkalosis, hypernatremia, or other electrolyte abnormalities.
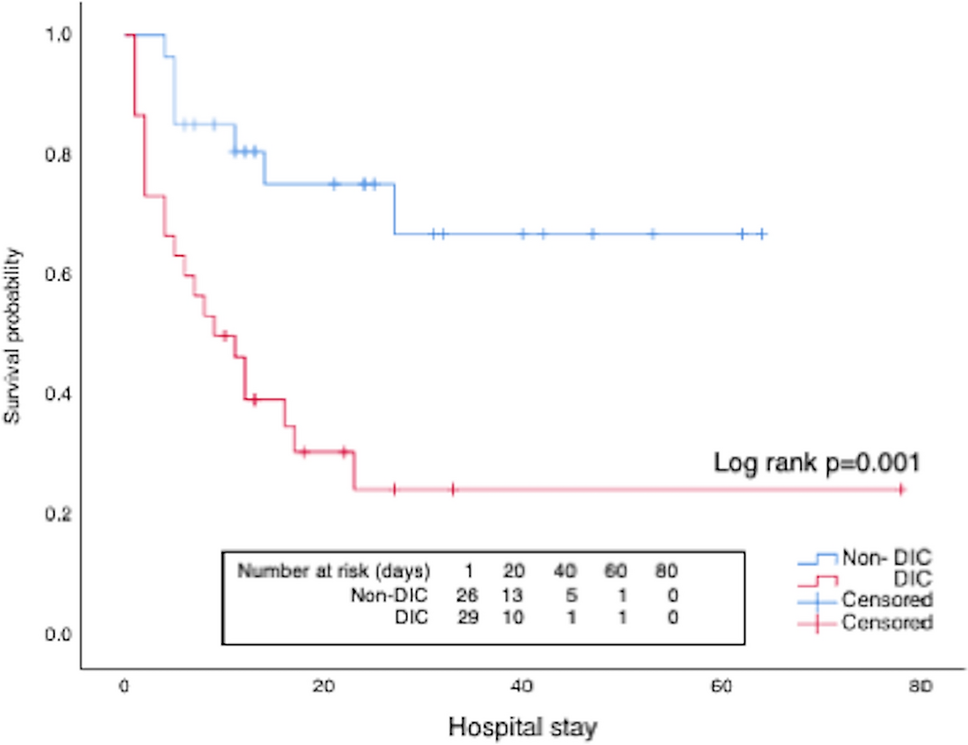
Unfortunately, the patient died on day 69 owing to infection and consequent disseminated intravascular coagulation, resulting in multiple organ failure while awaiting implanted VAD treatment with the expectation of a heart transplant. Nonetheless, Impella CP was still functioning normally when the patient died, with a purge flow of 12.4 mL/h and a purge pressure of 420 mmHg.
Comments (0)