
Remember me

The patient was a 26-year-old man with a history of cerebral palsy and epilepsy. He was admitted to a local hospital with a fever and bloody diarrhea. Stool culture testing detected Enterohemorrhagic E. coli, indicating a gastrointestinal infection. On the sixth day of hospitalization, blood tests revealed thrombocytopenia, hemolytic anemia, and renal failure. Based on these features, the patient was diagnosed with HUS caused by Shiga toxin-producing Escherichia coli (STEC). His blood pressure and oxygenation began to deteriorate on the tenth day of hospitalization, and he was transferred to our hospital.
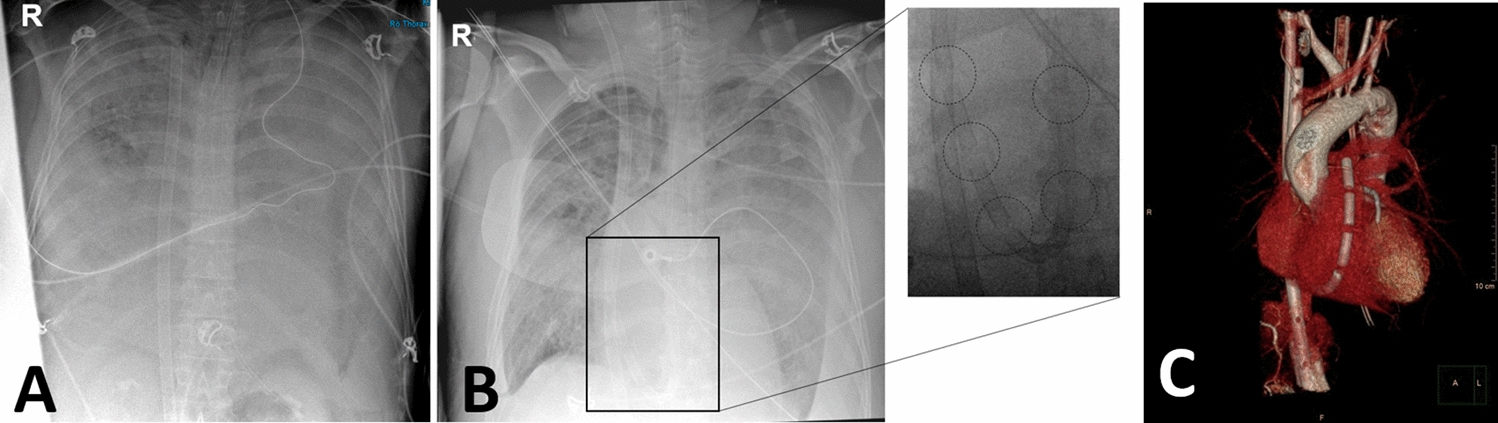
On arrival, he presented with septic shock, with a systolic blood pressure of 50 mmHg, tachycardia, and metabolic acidosis. Soon after admission to the intensive care unit (ICU), his systolic blood pressure dropped to 26 mmHg, and he went into cardiac arrest. The patient was soon resuscitated and commenced vasopressin and continuous renal replacement therapy (CRRT). Laboratory tests showed features of disseminated intravascular coagulation (DIC) with a platelet count of 20 × 109/L, activated partial thromboplastin time 85.5 s, prothrombin time – international normalized ratio of 1.77, and D-dimer of 6,750 ng/mL. Other laboratory tests showed C-reactive protein (CRP) 427.6 mg/L, white blood cell count 18.83 × 109/L, procalcitonin 0.38 μg/L, hemoglobin 43 g/L, lactate dehydrogenase (LDH) 1478 IU/L, and fragmented red blood cells in the peripheral blood smear (Fig. 1a). The haptoglobin level was 0.441 g/L on arrival to the hospital, which was higher than in the previous hospital, but decreased again to 0.07 g/L on the fourth day of hospitalization. The patient also presented with oliguria and an elevated creatinine of 304.98 μmol/L. ADAMTS13 activity was 31.58%, and ADAMTS13 inhibitor level was below 0.5 BU/mL, excluding thrombotic thrombocytopenic purpura (TTP). AmpC beta-lactamase-producing Enterobacter ludwigii was isolated from blood cultures, and the initial antibiotics meropenem and vancomycin were continued. Chest computed tomography (CT) revealed diffuse bilateral ground-glass opacities, consolidation, and interlobular septal thickening, indicating pulmonary edema (Fig. 1b). Abdominal computed tomography (CT) revealed intestinal wall thickening and ascites, indicating severe colitis (Fig. 1c). Based on these findings, we suspected ARDS secondary to septic shock caused by bacterial translocation.
Fig. 1
(a) Fragmented red blood cells are found in peripheral blood smears. (b) Chest CT showing diffuse bilateral ground-glass opacity, consolidation, and interlobular septal thickening. (c) Abdomen CT showing intestinal wall thickening and ascites
After resuscitation, he required 0.1 µg/kg/minute intravenous infusion of norepinephrine and 0.03 units/minute intravenous infusion of vasopressin to achieve a mean blood pressure of 65 mmHg. He had severe hypoxia with a PaO2/FIO2 ratio of 55 under PEEP settings of 15 cmH2O and FIO2 of 1.0. Arterial blood gas analysis showed pH 7.121, partial pressure of carbon dioxide (PaCO2) 51.9 mmHg, bicarbonate (HCO3−) 16.5 mmol/L, and lactate 2.7 mmol/L. We performed prone positioning for a few hours but with no oxygenation improvement. Although the patient was an adult, we consulted a pediatric cardiac surgeon for ECMO cannulation because of the short stature and small size of the blood vessels. Since the patient’s respiratory status continued to decline despite high mechanical ventilation settings and prone positioning, and also because the pediatric cardiac surgeon team was needed for ECMO cannulation, the decision to implement VV-ECMO was made on the second day of hospitalization before a full session of prone positioning was performed. Since his blood pressure was manageable with vasopressor drugs, we planned to start with VV-ECMO and insert an additional arterial cannulae when there was prominent hemodynamic instability. A 22 Fr drainage cannula was inserted into the right femoral vein, and an 18 Fr return cannula was placed in the right internal jugular vein. Heparin infusion was used for anticoagulation, along with nafamostat mesylate as an anticoagulant for CRRT to prevent membrane occlusion. As nafamostat mesylate has an extremely short half-life, we used both anticoagulants so that systemic heparin could be titrated according to ECMO anticoagulation protocols while maintaining CRRT anticoagulation and preventing circuit clotting events. Adequate oxygenation was achieved at a flow of 3.3 L/minute, 2900 revolutions per minute (rpm) under lung-protective ventilation settings. His blood pressure gradually improved upon the implementation of ECMO.
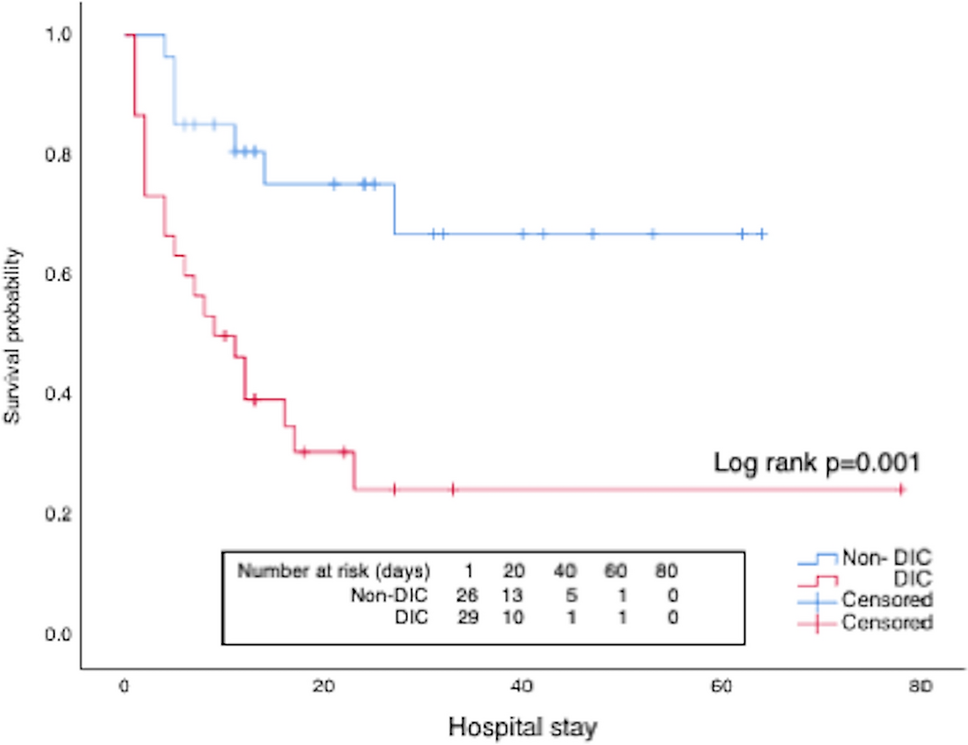
Since features of hemolysis were observed from the beginning of ECMO implementation, careful monitoring was continued. On day one of VV-ECMO, the patient’s plasma free hemoglobin level was 20 mg/dL. Plasma-free hemoglobin was measured daily, with the highest value being 40 mg/dL. However, there were no sudden or pronounced elevations throughout the course (Fig. 2). Other hemolytic features were also observed after the implementation of ECMO. High levels of LDH and fragmented red blood cells were present for the first three days of ECMO but rapidly decreased. Haptoglobin levels increased compared to the level before transfer on the first day of hospitalization but decreased again after the initiation of ECMO. Routine ECMO circuit monitoring of pre-membrane pressure, post-membrane pressure, and pump inlet pressure was performed, along with pre- and post- ECMO membrane blood gas measurement, and anticoagulation monitoring using thromboelastography. While there were prominent features of hemolysis, monitoring of ECMO circuit pressures and oxygenation performance showed no suspicion of thrombosis. Inflammatory markers such as CRP showed marked improvement after hospitalization. The hypoxemia improved, and the patient was weaned off ECMO on the eleventh day of hospitalization without any complications. The patient was weaned off the mechanical ventilator on the fifteenth day and returned to the local hospital on the twenty-second day.
Fig. 2
The plasma-free hemoglobin level was higher than 10 mg/dL throughout ECMO but did not exceed 50 mg/dL. LDH and CRP levels rapidly decreased within the first 3, 4 days. Fragmented red blood cells appeared only in the first 4 days of hospitalization
Comments (0)