
Remember me







The monitoring of Streptococcus pyogenes infections in Poland on the national level is based on the reports submitted by healthcare service providers to the Chief Sanitary Inspectorate. The epidemiological data is then analysed; the incidence ratio calculated and published as bulletins by the National Institute of Public Health — National Institute of Hygiene. The data collection does not require providing the strains for the molecular analysis. Due to voluntary reporting, in many cases, the data suggests misdiagnosis. For example, incidence data suggests overdiagnosis of scarlet fever instead of pharyngitis as the ratios are extremely high in comparison with the data from other countries (Fig. 1A).
Fig. 1
A Incidence of scarlet fever in Poland 2003–2017 in age groups based on the data reported by health authorities. B Upper respiratory tract infections reported to the authorities and collected isolates (by age groups). C Comparison of seasonal variability of infections based on report and strain data
Over the years, parallel data has been gathered by the NMI as a part of surveillance programs (http://koroun.edu.pl/koroun/projekt-aleksander/, in Polish). The information about the strains sent to the NMI does not contain the diagnosis, but the source info, i.e. upper respiratory tract or other body sites, information about sex and age of the person who was the source of the strain. Between 2003 and 2017, NMI received 1780 isolates with confirmed upper respiratory tract origin. Strains were isolated from males and females in equal proportions. Strains sent to NMI were predominantly collected from children, and about 65% of strains were collected from children up to 15 years of age. A slight increase was observed for those aged 30–39 what might reflect a group of parents with children aged 0–15 (Fig. 1B). The metadata from the analysis of collected strains reflects multiple epidemiological aspects such as seasonal variability (Fig. 1C), with the highest number of collected strains in April and December and the lowest in August and September.
The strains collected as a part of those surveillance programs were used for molecular analysis to describe molecular dynamics of the S. pyogenes population in Poland over 15 years.
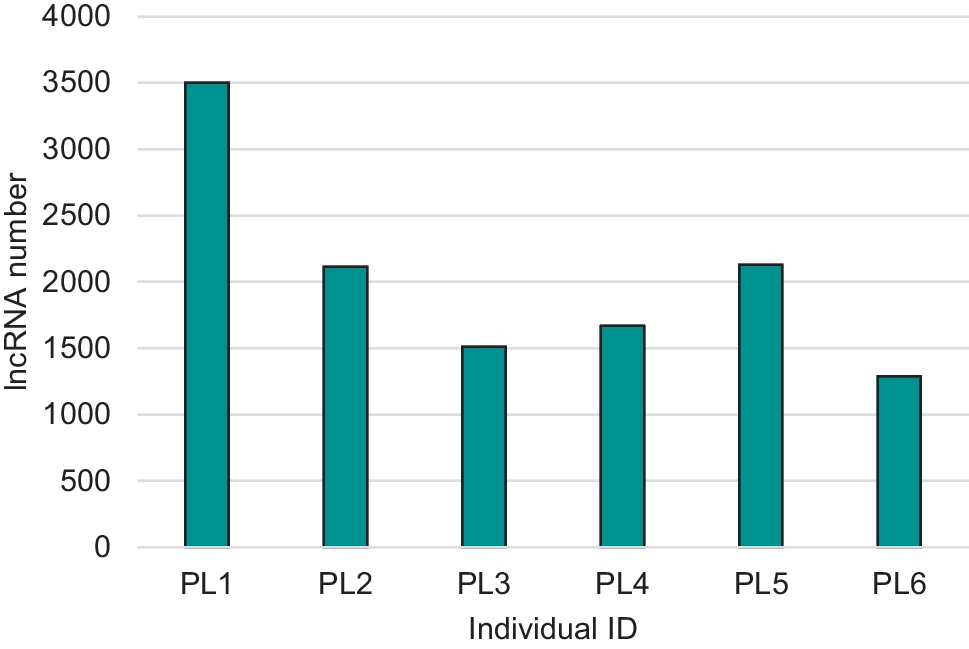
Distribution of M types and association with the respiratory tract infectionsWe assigned M types to 1753 isolates from the upper respiratory tract collected between 2003 and 2017. We detected over 65 different M types; however, 10 M-types constituted almost 88% of all strains (Fig. 2). The largest number of strains belonged to serotypes M1 (287 isolates, 16.4% of collected strains), M12 (283, 16.1%), M28 (235, 13.4%), M89 (187, 10.7%), M77 (129, 7.36%), M4 (120, 6.8%), M3 (113, 6.5%), M6 (82, 4.7%), M75 (58, 3.3%), and M2 (47, 2.7%).
Fig. 2
Yearly distribution of 10 the most common M types between 2003 and 2017. As the number of strains sent every year varied, we compared fractions represented by each serotype in a particular year
To test if any particular serotype is responsible for more upper respiratory tract than other types of infections, we performed the correlation analysis for five top serotypes (M1, M12, M28, M89, and M77) (Fig. 3). We compared the year-to-year percentage of strains causing upper respiratory tract vs other types of infections. We did not observe significant differences between M12, M28, and M89 strains isolated from upper respiratory tract vs other available sources (P > 0.2). However, a percentage of M1 strains isolated from the upper respiratory tract infections was significantly lower than the percentage of M12 and M28 strains (P = 0.0021 and P = 0.0149 respectively) that suggests a correlation between M1 serotype and invasive infections. On the contrary, significantly more M77 strains originated from the upper respiratory tract than M89 and M1 (P = 0.023 and P < 0.0001 respectively).
Fig. 3
Correlation between the fraction of upper respiratory tract infecting strain compared with for serotypes M1, M12, M28, M89, and M77. Combined data represents years 2003–2017
Virulence factor distributionAs the virulence of GAS is closely related to the ability of this pathogen to cause the disease, we wanted to test the presence of the virulence factors encoded by upper respiratory tract isolates. However, the presence of certain virulence factors is more related to the invasive disease; we wanted to test the distribution of genes encoding these factors to compare the profiles to profiles from invasive strains in the future. We used a set of multiplex PCR reactions to detected GAS superantigens, DNAses, proteases, and sic gene.
All strains carried at least three virulence genes, with the 80% of strains containing 7–12 virulence factors. We identified only one strain that carried 14 virulence factors. Majority of strains carried smeZ, speG, and sdaB, virtually all strains carried speB, mac, and spyCEP. SpeC was carried by 40% of strains, and other superantigens were encoded by 10–20% of strains, with the smallest fraction carrying speL (70 of 1780 strains). Sic gene was detected in about half of M1 and single M12 strains.
The analysis of strain similarity based on the presence/absence of the genes encoding virulence factors has shown a close correlation of distinct patterns with the serotype (Fig. 4A). Also typing, based on phage profiling (PP) method, shows correlation between type of PP pattern/type and the serotype (Fig. 4B).
Fig. 4
A Neighbour-joining tree generated based on the presence of virulence patterns. B Neighbour-joining tree based on phage profiling patterns
Evolutionary framework (MLVA based)We performed an analysis of polymorphic loci in GAS genomes (MLVA — multi locus variable tandem repeats analysis) to establish clonal variability of the studied population (Obszańska et al. 2011). Strains of M1 serotype were highly clonal and over 98% of detected MLVA patterns belonged to the single pattern type with subtypes (A-A2). Other serotypes were more diverse, with M12 and M4 strains being the most diverse (Fig. 5).
Fig. 5
Variability of MLVA patterns detected for 10 the most common serotypes
Antibiotic resistanceWe screened by PCR all isolates for the presence of genes responsible for the majority of erythromycin (mefA, ermA, and ermB) and tetracycline (tetM and tetO) resistance in GAS. Three hundred and sixty-seven of 1780 strains carried at least one of the resistance genes (20.6%). Overall, 259 strains carried erythromycin resistance gene (129 ermA, 72 ermB, 58 mefA) and 238 carried tetracycline resistance gene (132 tetO, 106 tetM), what makes 14.6% and 13.4% respectively. However, the fraction of strains carrying antibiotic resistance genes varied from year to year (erythromycin 7.4 to 21.8%; tetracycline 4.7 to 27.8%) without any noticeable increasing or decreasing trend over the years (Fig. 6). The fraction of tetO carrying strains was slightly higher than tetM (7.1% vs 6.5%). Among macrolide-resistant strains dominated those carrying ermA (6.6% of all strains) in comparison with ermB (4.4%) and mefA (3.35%).
Fig. 6
Distribution of erythromycin (red/pink) and tetracycline (orange/yellow) resistance genes by year. Each column shows cumulative fraction that includes ermA/ermB/mefA or tetO/tetM genes. Data from 1996 to 2002 are after (Szczypa et al. 2004) without resistance gene analysis, shown as comparison to our data; red columns show the phenotypically assessed levels of erythromycin resistance and the yellow one — tetracycline resistance
We noted reported previously specific associations between certain M type and carried antibiotic resistance genes. Average resistance to erythromycin in strains with assigned M type was 14,29% (95% CI 12.72 to 16.02%); however, certain M types exhibited significant (P < 0.05) increase or decrease in the fraction of resistant genes in comparison with the population average. For example, over 66%, 65%, and 19.6% of M44, M77, and M28 strains, respectively, were resistant to erythromycin, while only 1% of M3, 2.2% of M89, and around 6% of M1, M6, and M2 were found to be resistant. The fraction of erythromycin-resistant strains carried by other M types was within the 12.7% and 16% range.
ErmA gene was detected predominantly among M77 and M28 strains (64% and 9.3% of ermA carrying strains respectively). ErmB gene was distributed among M28 and M12 strains (46% and 33% of ermB carrying strains respectively). Majority of mefA carrying strains were of M12, M1, and M4 serotypes (26%, 21%, 19% respectively). On the other hand, 119 of 132 (90%) of tetO carrying strains were classified as M77. tetM gene was strongly associated with M1 (22.6%) and M28 (18%) strains. The M77 strains that carried tetO or ermA/tetO genes were highly clonal, all belonged to ST63, and they cluster together based on MLVA and phage profiling.
To confirm a resistance phenotype, we performed MIC analysis for penicillin, erythromycin, clindamycin, and tetracycline for every strain with the detected resistance gene. In addition, for every putative erythromycin-resistant strain, we performed double disc diffusion test to detect a phenotype of inducibility for the erm gene. MIC assays showed that all analysed strains were sensitive to penicillin. MIC median value for penicillin was 0.015 mg/L (MIC50 0.015 mg/L, MIC90 0.03 mg/L). For tetracycline, the MIC values of the resistant strains were either 32 mg/L or 16 mg/L. For erythromycin, over 85% of strains had MIC values above 16 mg/L, regardless of the gene or inducibility mechanism; however, strains that had lower MIC value exhibited either M or iMLSB phenotype.
Comments (0)