
Remember me
Two decades ago, the first report appeared on watch-and-wait for rectal cancer patients with a clinical complete response (cCR) after neoadjuvant (chemo)radiotherapy.1 This report sparked a large interest and was followed by many more studies exploring watch-and-wait and organ-preserving treatment strategies for rectal cancer.2–11 Initially, patients were only considered for watch-and-wait when meeting the strict criteria of a cCR1,2,5: absence of residual abnormalities with digital rectal examination (DRE), flat white scar on endoscopy, substantial downsizing without signs of residual tumor on T2-weighted (T2W) MRI, and the absence of diffusion restriction on diffusion-weighted MRI (DWI).12,13 However, surgery in patients with minor residual abnormalities on restaging revealed a pathological complete response (pCR) in around half of the patients.14–16 These patients who underwent rectal resection were denied organ preservation. This led to more liberal selection criteria, and patients with a so-called clinical near-complete response (nCR) were also considered for watch-and-wait.13,17,18 Recently, a study from the large International Watch-and-Wait (IWWD) database revealed that watch-and-wait is a valid treatment option for patients with an nCR.19 Therefore, watch-and-wait for patients with a cCR or nCR is incorporated in different inter(national) guidelines.20–22
In contrast to the well-defined criteria of a cCR, the criteria and features of an nCR vary substantially.13,17,23,24 A wide variation in scoring systems and terminology used for an nCR was described in a systematic review of the definition of an nCR.25 This variability is likely the result of different views on what an nCR is applied to, the appropriateness of watch-and-wait in case of an nCR, and patient preference in decision-making. The systematic review revealed that very little evidence is available to support the use of specific feature combinations to define an nCR. Consequently, consensus on the definition of an nCR after neoadjuvant (chemo)radiotherapy for rectal cancer is lacking.
Therefore, a consensus process was initiated to improve consistency in practice and research while awaiting new evidence. The results of this expert-based consensus process may provide guidance in clinical decision-making and can be used in planning new studies that use this definition of an nCR. Therefore, the aim of this study was to reach expert-based consensus on the definition of an nCR after neoadjuvant (chemo)radiotherapy for rectal cancer using a modified Delphi method.
MATERIALS AND METHODSThe modified Delphi consensus process included first and second phases. The first phase started with a survey on potential clinical and imaging features and was based on a previously performed and published systematic review.25 Subsequently, an online expert panel meeting was performed to discuss these features. The second phase consisted of 2 surveys—a survey on individual features and a survey on feature combinations—and was followed by a second online expert panel meeting. The outline of the study is provided in Figure 1.
 FIGURE 1.:
FIGURE 1.: Study outline and details on the 3 online surveys. DWI = diffusion-weighted imaging; T2W = T2-weighted.
Panel SelectionFor this study, an international expert panel was selected, including 7 colorectal surgeons (G.L.B., S.P.B., N.F., A.M., J.M., R.O.P., and J.J.S.) and 4 dedicated abdominal radiologists (L.K.B., M.J.G., C.D.O., and M.M.). All experts have clinical expertise in the field of watch-and-wait and organ preservation for rectal cancer and are involved in the IWWD. To ensure widespread support of the proposed definition of an nCR, experts were selected who were affiliated with different institutions in various countries and continents and contributed significantly to the research field of watch-and-wait and organ preservation.
Online SurveysThis modified Delphi process included a first survey based on the previously published review, a second survey on individual features, and a third survey on endoscopy, T2W-MRI, and DWI feature combinations. The first survey consisted of 21 individual features; 20 feature combinations; and 20 statements on different imaging modalities, lymph nodes, and the role of biopsies. Of this survey, 8 features and 5 statements on the assessment by endoscopy were only scored by the surgical panelist. The second survey included 21 individual features and 12 statements on the indication for using the nCR terminology and the role of baseline characteristics when deciding on an nCR. The third survey consisted of 30 feature combinations and 15 statements on the importance of different imaging modalities for luminal response assessment. Details on all surveys are provided in Figure 1.
The expert panel was asked to assign the features and feature combinations to 1 of 3 categories: cCR, nCR, or incomplete response (iCR). In addition, the panelists were asked to rate their comfort level to extend the waiting interval with another 6 to 8 weeks for each feature and feature combination of the last 2 surveys. All surveys were conducted using an online tool (survio.com) and were constructed by 1 author (P.A.C.) under the supervision of 2 senior authors (G.L.B. and M.M.). All images used were obtained at restaging 8 to 12 weeks after long-course neoadjuvant chemoradiotherapy. The images were accompanied by a brief description, which was put forth to minimize interpretation bias. Consensus was defined as 80% or more agreement.
Online Expert Panel MeetingsTwo online expert panel meetings were held. Both meetings were prepared and documented by 1 author (P.A.C.) under the supervision of 2 senior authors (G.L.B. and M.M.). Statements were prepared for discussion in both meetings based on the completed surveys. After discussion, these statements were adapted to reach consensus if necessary.
The first online meeting took place on November 29, 2021. Ten of the 11 panelists attended the meeting. The purpose of this meeting was to get more insight into what was considered an nCR, including features indicative of an nCR and timing of establishing an nCR. In addition, the terminology for an nCR and the methodology for the second part of this study were discussed.
The second and final online meeting took place on June 22, 2022. Nine of the 11 panelists attended the meeting. The aim of this meeting was to achieve more uniformity in the definition of an nCR and to establish a schedule to guide clinical practice for patients with an nCR.
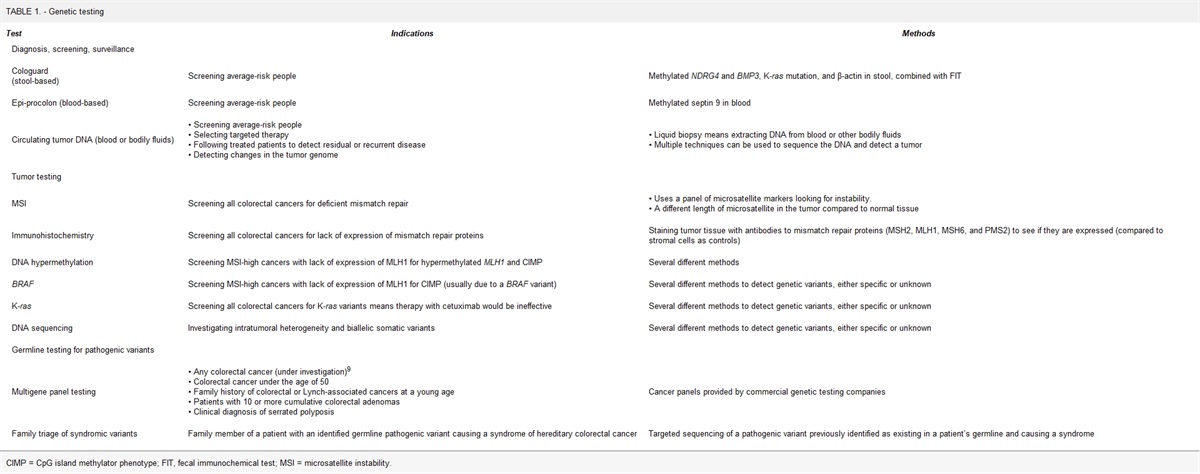
RESULTS Survey ResultsConsensus was reached on 8 of 21 (38%) features, 6 of 20 (30%) statements, and 6 of 20 (30%) feature combinations of survey 1 and on 5 of 12 (42%) statements and 14 of 20 (67%) features of survey 2. In survey 3, consensus was reached on 5 of 15 (33%) statements and 9 of 30 (30%) feature combinations. Table 1 shows all statements with and without consensus included in all 3 surveys. Table 2 shows all feature combinations with and without consensus of survey 3. Other outcomes are provided in Supplemental Tables S1 to S4 at https://links.lww.com/DCR/C300.
TABLE 1. - Statements of all 3 surveys with and without consensus Statements on which consensus was reached % Consensus Survey 1 There is an incomplete response if there are multiple suspected residual lymph nodes. 100% Agree To decide whether there is a (near)-complete response, lymph node status should always be taken into account. 91% Agree There is an incomplete response if there is a suspicious residual lateral lymph node. 82% Agree If a near-complete response is found, a biopsy is always needed. 100% Disagree Assessing the overall response of the tumor, the response on endoscopy is equally important as the response on MRI. 91% Disagree On endoscopy, adenomatous tissue and regenerative tissue can be considered as equal. Both features can be categorized as 1 group. 86% Disagree Survey 2 With further follow-up, a near-complete response should, in principle, evolve into either a complete response or an incomplete response. 100% Agree I use the label clinical near-complete response when at the first assessment, after 8 to 12 wk, there is not a typical complete clinical response, but a very good response that, with further waiting, could become a typical complete clinical response. 91% Agree A clinical near-complete response (8–12 wk) is a response category indicating major tumor regression. Whether there is pathology-proven adenocarcinoma is irrelevant. 82% Agree The label clinical near-complete response at 8 to 12 wk is determined only by the clinical diagnostic examinations and does not depend on whether a choice is made to resect or to watch-and-wait. 82% Agree I don’t use the terminology near complete. 91% Disagree Survey 3 When on T2W-MRI irregular homogenous fibrosis is observed and on DWI a linear signal is observed, the importance of endoscopy is 91% High When on T2W-MRI irregular heterogeneous fibrosis is observed and on DWI small spots are observed, the importance of endoscopy is 91% High When on T2W-MRI regular homogeneous fibrosis is observed and on DWI no high signal is observed, the importance of endoscopy is 82% High When on endoscopy a tumour remnant (biopsy proven) is seen and on T2W-MRI irregular heterogeneous fibrosis is observed, the importance of DWI is 82% Low A solution to get more uniformity regarding the definition of a near-complete response is to split the near-complete response category into 2 separate categories with different terminology and different clinical criteria and features: 1) for a response with a high likelihood of progression into a clinical complete response after which watchful waiting can be considered, and 2) for a major response after which additional local treatment (such as local excision) aiming at organ preservation can be considered as there is still a possibility of (a small) residual tumor. 82% Agree Statements on which no consensus was reached % Consensus Survey 1 On endoscopy, tumor mass is always an incomplete response, irrespective of the response on MRI. 73% Agree There is an incomplete response if there is 1 suspicious residual lymph node. 73% Agree On endoscopy, an ulcer with elevated borders is always an incomplete response, irrespective of the response on MRI. 71% Agree On T2W-MRI, a tumor mass is always an incomplete response, irrespective of the response on endoscopy and DWI. 64% Agree On endoscopy, a flat scar with some red spots and a flat white scar can be considered as equal. Both features can be categorized as one group. 57% Agree On DWI, 1 single spot of high signal and a linear focal signal can be considered as equal. Both features can be categorized as one group.a 45% Agree On DWI, 1 single spot of high signal and a linear focal signal can be considered as equal. Both features can be categorized as one group.a 45% Don’t know On endoscopy, the size of the ulcer is not relevant for the response assessment. 71% Disagree Assessing the response on the T2W-MRI, the heterogeneity of the fibrosis is equally important as the regularity of the fibrosis. 64% Disagree On DWI, a mass-like diffusion signal is always an incomplete response, irrespective of the response on endoscopy and T2W-MRI. 64% Disagree When on T2W-MRI mucinous spots are seen and there is a clinical complete response on endoscopy and DWI-MRI, the overall tumor response is a complete response. 64% Disagree Whether lymph node status should be taken into account when deciding on a (near)-complete response depends on the location of a suspicious lymph node. 64% Disagree Assessing the response on MRI, the response on T2W-MRI is equally important as the response on DWI. 55% Disagree On DWI, multifocal spots are always an incomplete response, irrespective of the response on endoscopy and T2W-MRI. 55% Disagree If there is downsizing of the lymph nodes, lymph node status should not be taken into account when deciding on a (near)-complete response and subsequent choice for watchful waiting. 45% Disagree Statements on which no consensus was reached (continued) % Consensus Survey 2 A response grading in a number of categories with an increasing percentage of “true complete response” such as used in other diagnostic fields (BIRADS, PIRADS) would be more helpful than the label “near-complete” response. 73% Agree The only criterion standard of a “true complete response” can only be established retrospectively: a durable and persisting clinical absence of tumor during follow-up after watch-and-wait. 64% Agree Baseline characteristics have to be taken into account when deciding on a near-complete response. 64% Agree A correlation of the different response features at different time intervals with a % of “true complete response” would be more helpful than the label “near-complete” response. 64% Agree When there is a (very) small residual tumor remnant, that can be treated with organ preservation intent (local excision and contact radiotherapy), I also use the label near-complete response. 55% Agree When there is a very good response at first assessment, but not (yet) a clinical complete response, I discuss the option of further waiting, but I don't label this near-complete response. I rather consider it an extended observation period. 73% Disagree A clinical near-complete response (at 8–12 wk) is a response category indicating a major tumor regression. Whether it will progress to a clinical complete response is irrelevant. 55% Disagree Survey 3 When with endoscopy a large ulcer with elevated border is seen and on DWI no high signal is observed, importance of T2W-MRI is 73% High When on T2W-MRI irregular heterogeneous fibrosis is observed and on DWI a mass-like diffusion signal is observed, the importance of endoscopy is 73% High When with endoscopy a flat white scar is seen and on DWI a linear signal is observed, the importance of T2W-MRI is 64% High When with endoscopy a flat red scar is seen and on T2W-MRI irregular heterogeneous fibrosis is observed, the importance of DWI is 64% High When with endoscopy a large flat ulcer is seen and on T2W-MRI regular fibrosis is observed, the importance of DWI is 64% High When with endoscopy a flat white scar is seen and on DWI no high signal is observed, the importance of T2W-MRI is 45% High When with endoscopy a tumor remnant (biopsy proven) is seen and on DWI a mass-like diffusion signal is observed, the importance of T2W-MRI is 73% Low When with endoscopy a flat white scar is seen and on T2W-MRI regular homogeneous fibrosis is observed, the importance of DWI is 36% Low When there is a discrepancy between T2W-MRI and DWI, T2W-MRI and DWI are equally important. 64% Disagree When there is a discrepancy between endoscopy and MRI, endoscopy and MRI are equally important. 55% DisagreeBIRADS = Breast Imaging Reporting and Data System; DWI = diffusion weighted imaging; PIRADS = Prostate Imaging Reporting and Data System; T2W = T2 weighted.
aSame statement.
DWI = diffusion-weighted imaging; T2W = T2-weighted.
Table 3 provides the statements and recommendations that the panelists agreed on during the 2 online panel meetings. The most relevant recommendations for clinical practice are as follow:
TABLE 3. - Statements and recommendations on which all panelists agreed during the 2 online expert panel meetings Online expert panel meeting 1 The response category “near-complete response” is a category that can be used only temporarily. A near-complete response is a temporary state that can be used in the first 6 mo from the end of chemoradiotherapy. The response assessment should be based on all 3 modalities: endoscopy, T2W-MRI, and DWI. Online expert panel meeting 2 When a flat white scar and a flat red scar are seen on endoscopy, the comfort level in waiting 6 to 8 wk longer is equal. When deciding on a near-complete response, the size of the adenomatous tissue is not of importance. When there is a discrepancy between the response on endoscopy and MRI, the overall response should rely more on endoscopy than on MRI (in case of the absence of extramural disease). When mucinous spots are observed on T2W-MRI, the overall response should rely more on endoscopy than on MRI.DWI = diffusion-weighted imaging; T2W = T2-weighted.
Although consensus was reached on multiple features, feature combinations, and statements, it became clear during the process that it was impossible to form 1 unequivocal definition of an nCR. The expert panel regarded the nCR category as a continuous spectrum of good responses with a high to low likelihood of evolving into a cCR with further observation. The panelists reached consensus that a subcategorization of the nCR category based on this likelihood may be a solution to be explored to reach more uniformity and practical applicability than defining a single category. Subsequently, the panelists agreed on the use of a 3-tier subcategorization of an nCR, stratifying an nCR with a high, intermediate, and low likelihood to achieve successful organ preservation. Based on the results of the questionnaires, 3 proposals for the 3-tier subcategorization were made. After the final expert panel meeting, 9 of 11 (82%) experts agreed on the use of the nCR subcategorization as provided in Figure 2. Figure 3 provides a pictorial overview of the features used in Figure 2. Moreover, agreement was reached on the responses at both ends of the nCR category. On one hand, a cCR is defined as a flat white/red scar on endoscopy, regular homogeneous fibrosis on T2W-MRI, and no diffusion restriction on DWI. On the other hand, an iCR is defined as an ulcer with elevated borders of >3 cm or tumor mass of >3 cm on endoscopy or extramural disease on MRI with remaining evidence of tumor signal on T2W-MRI and DWI.
Comments (0)