
記住我





Today, quality assurance should be indispensable as part of the corporate culture of a clinical department [12]. There is almost a moral obligation to generate quality-controlled clinical data, considering that therapies and treatment recommendations are derived from translational research. As a result, data transparency plays an essential role. The ability to validate and possibly correct clinical documentation through regular checks in the clinical process (monitoring) is an integral part of quality assurance and quality management since the results can be acted upon. Regular audits of surgical documentation, surgical processes, and, for example, infection or pain control measures would help to identify and correct deficiencies. In addition to this clinical aspect, QA includes patient safety initiatives, such as surgical checklists [13] and handovers, to prevent errors and increase patient safety [14]. Furthermore, third parties (auditing) should be allowed to verify the data based on the original documents, such as the physician’s letters and operating room reports.
However, monitoring and especially auditing clinical data in a medically oriented documentation system is hardly established in any institution. Lack of data transparency is one of the primary sources of scientific fraud [15]. Analyses show that 72% of researchers know someone in their immediate professional environment who has manipulated data on a small or large scale [16]. It is a fact that data in translational and clinical research are predominantly opaque. Verifiable and transparent data must replace the “mere” trust in presenters and authors regarding data quality. Top journals have already responded by increasingly requiring original data sources for publication [17]. Internal departmental and supra-regional registries in health services research, including those run by the state, often show considerable quality deficits [18]. This is not least because too little importance is attached to clean and controlled data documentation, which is a medical task. It has been shown that only 80% of adverse events are documented by physicians [19]. Furthermore, the Swedish Rectal Registry published deficiencies in crucial parameters, such as the rate of anastomotic dehiscence, because the collection and documentation were delegated to non-physician personnel [20]. The establishment and maintenance of multi-institutional registers is exceptionally complex [18]. Therefore, there are several calls for registries to include quality assurance measures similar to those established in clinical controlled trials, including monitoring and auditing. These registries are called quality-controlled registries (qcRegistries), and statistical methods—including randomization—can be used to obtain results from them (registry-embedded clinical trials) that are equivalent to and should be considered additive to controlled randomized trials (CRT). Statistical methods include propensity score analysis, paired analysis, trials within cohorts (TwiCs) designs (rCRT), and batch randomization [21]. These can remove biases inherent to CRT, such as the age of the patients enrolled.
Quality assessmentQuality in medicine is fundamentally challenging to measure. For this reason, it has become common practice to measure quality in medicine using surrogate parameters. Ideally, these quality indicators (QIs) should be multifactorial (composite QI). Depending on their characteristics, they provide a graded distinction between excellent and poor quality. The requirements for QIs, the so-called QUALIFY criteria [22], include relevance, scientificity, and practicability. According to the medical field, quality indicators are defined by professional societies, for example, by the Studien, Dokumentations- und Qualitätszentrum (StuDoQ) [23] of the German Society for General and Visceral Surgery (DGAV) for the Rectal Cancer Registry, or by expert committees, or by departments themselves. Established QI examples are failure to rescue, textbook outcome, postoperative in-hospital, 30-day, and 90-day mortality, and other preferable composite QIs. The analysis of QI based on quality-assured documentation forms the framework for assessing the quality of services provided. For example, it can be clarified whether a goal was achieved, partially met, or missed, or a comparison with other hospitals can be made. In the case of registries, this comparison is made anonymously concerning all participating hospitals. This comparison is different from benchmarking in the narrower sense. The basic principle does not compare with the average of achievable results but with the best postoperative results that can be achieved under multifactorial, real-life conditions. The difficulty lies in identifying the “frontrunner(s),” the “leader in the class,” in determining generally valid parameters [24, 25], and in the quality of accessible databases of selected cooperating hospitals, which do not always have quality-controlled data that can be audited. In principle, however, this would be an interesting aspect in the field of quality management in that benchmarking promotes the intrinsic striving, the imperative must of surgeons, for perfection, rather than assessing the performance of the center or the surgeons [26,27,28].
From a vision to ChiBASEFrom what has been described so far, it is clear that valid and thus controlled and transparent data, which third parties can verify, is a central, obligatory factor in all quality management areas. These so-called quality-controlled registries (qcRegistries), whether set up at a departmental, supra-regional, or international level, do not exist in the quality described. Regarding the vision of a registry-embedded clinical trial, it is undisputed that surgical documentation can increase knowledge to better treat patients. The strategy is, therefore, to develop a comprehensive, department-wide, quality-controlled registry for medical documentation. This strategy was realized in Innsbruck with the proprietary documentation system ChiBASE, which provides quality-controlled data over several levels in clinical routine, which can be verified from within the program by third parties using unalterable original documents. ChiBASE was developed because there is currently no alternative to approach the vision of a registry-embedded clinical trial [29, 30]. Previous systems for clinical documentation were almost exclusively derived from other industries and were only modified for medicine, with the main focus on economic aspects. Mainly due to the documentation of surgical services using the LKF coding in Austria, these systems are unusable for the goals of quality-controlled surgical documentation. Many surgical services do not have a unique code. Another inherent problem is the complexity of surgical conditions, which makes it challenging to develop commercially available systems suitable for surgical documentation. The development effort is disproportionate to the size of the market. In addition, ChiBASE delivers not only quality of results but also quality of processes, in that the program accompanies the daily clinical routine so that the processes are mapped and checked for completeness and plausibility. The result of 30 years of development is a modular system. In addition to the possibilities of quality-controlled recording of procedures, postoperative morbidity, adverse events, and the history of the clinical course, a tool for personnel development and deployment, a recording of teaching and publication performance, a reporting of critical data and key point indicators (KPI), a knowledge database, a content database for standard operating procedures (SOP), a blog, handovers for services, and much more are available (Fig. 1). As the modules interlock like gears, they open up unprecedented dimensions of interrelationships. Basically, a medical documentation system requires six dimensions of data quality: completeness, accuracy, consistency, validity, uniqueness, and integrity [31]. All problems related to these parameters in uniform coding and assignment have been solved in ChiBASE. Completeness is ensured by the establishment of a “minimal dataset” and by the introduction of closure routines. Unambiguity is ensured by integrating jargon catalogs relating to surgical services (ICPM++) and diagnoses (ICD-10++). The surgical procedures have been modified in wording according to the International Codes of Procedures in Medicine (ICPM) [32] (one “plus” stands for this, and the second “plus” stands for additional procedures that do not appear in the ICPM). The same applies to diagnoses, where complications had to be mapped more precisely in the ICD-10++ catalog. Currently, the ICPM++ comprises 1056 procedures and the ICD-10++ 15,144 diagnoses. Another problem was the specific automatic assignment of postoperative morbidity to operations or procedures. Understandably, with more than 100,000 operations at present, this cannot be done manually. The solution is to define a leading operation and its procedures when checking an operation with several operations during an inpatient stay, and to define the leading procedure for an operation within several procedures. Thanks to the special user-friendly tools included in the program, this can be done in a few seconds and does not interfere with the checking process in any way. The modified terminology catalogs (ICD-10++ and ICPM++) ensure uniqueness, which can be considered a table, where the first column contains the terminology text with numerous synonyms, followed by several other expressions. The international code, the wound class according to Cruse [33], the affiliation of the service to the Surgical Training Certificate, the responsible working group, and so on (see Fig. 2), are such additional characteristics. This makes it possible, for example, to stratify wound infection rates according to wound classification or to provide trainees with an up-to-date overview of their training status.
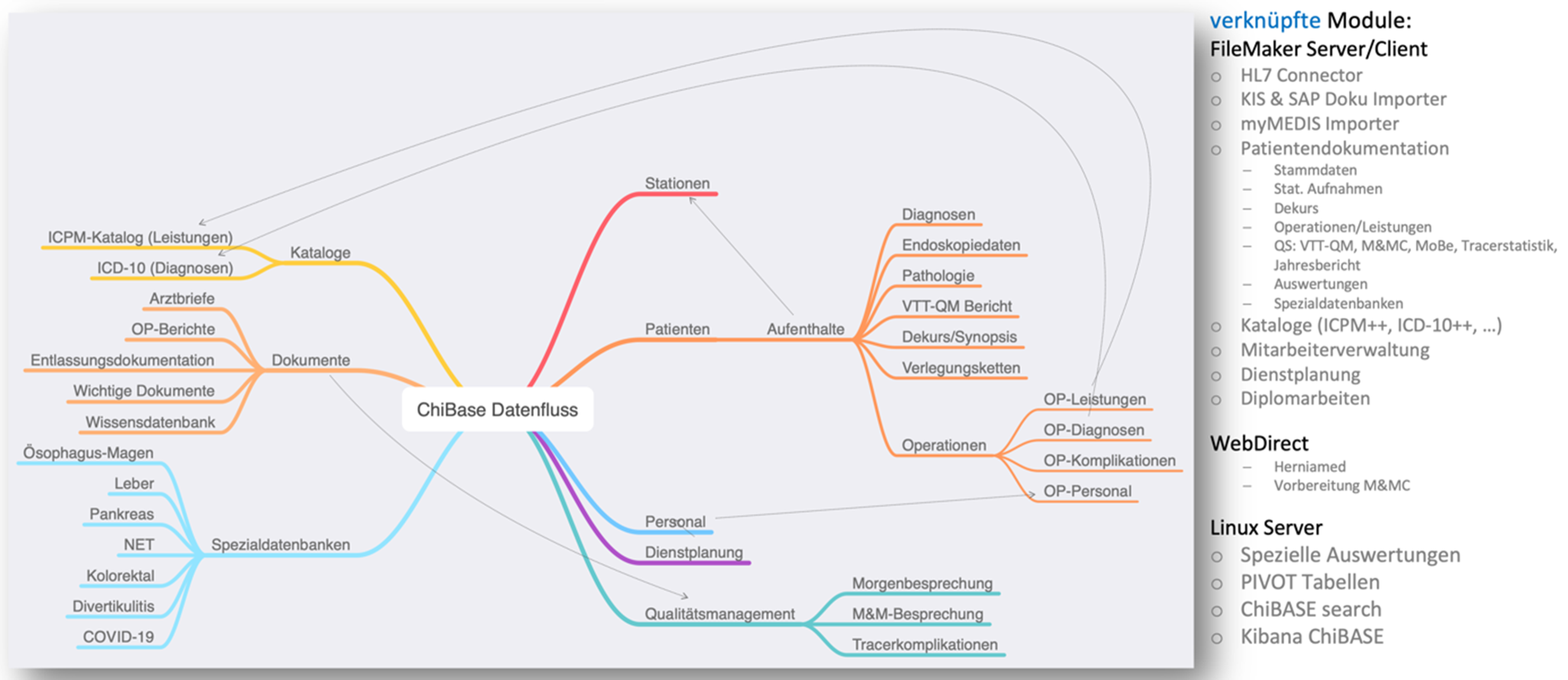
Fig. 1
Data stream and modules in ChiBASE, courtesy of B. Schulz, Salzburg
Fig. 2
So-called jargon catalog of procedures (ICPM++ codes). ICPM International Codes of Procedures in Medizine, MEL Medizinische Einzelleistung, SURG suergery
留言 (0)