Drug-related deaths constitute a large proportion of forensic cases in Denmark because current legislation requires routine autopsies in these deaths. This study showed that this subgroup of deaths could be eligible for COD prediction based on EA-Triage including PMCT and QTA. Notably, EA-Triage and conventional autopsy agreed on COD in 99% of drug-related deaths with nonsuspicious circumstances.
Many countries, including Denmark, which has the lowest autopsy rate among the Nordic countries, are experiencing declining autopsy rates [22]. The reasons for this decline are most likely a combination of prioritizing resources; religious, cultural or emotional reluctance against invasive autopsy; variable legislation; and biosafety awareness [23]. To accommodate this trend, an increasing need for alternatives to autopsies has emerged. Therefore, the incorporation of minimally invasive screening techniques in the forensic field has been widely researched for different subgroups. In other investigations on preautopsy COD determination, toxicological analysis has been shown to improve the diagnostic agreement. Hueck et al. increased the agreement on COD from 85.9 to 95.3% when considering histological and toxicological findings in unnatural deaths [11]. Leth et al. also had toxicological analysis available on large amounts of material from the Danish forensic population [12]. Consistent with our results, they found that in 50% of cases with intoxication, a COD could have been predicted if a day-to-day toxicological service combined with PMCT had been available. In a study from New Mexico, cases of drug-related deaths were examined to evaluate the ability to determine COD prior to autopsy when considering PMCT and toxicology analysis. The COD agreement was 78%, but it was higher for individuals younger than 50 years (84%) [3]. Hence, our study results are consistent with prior research. Overall, we demonstrated a substantial agreement of 73% (99% when excluding cases with unknown COD) for cases without suspicious circumstances between EA-Triage and conventional autopsy in determining COD in drug-related deaths when toxicological analysis is considered.
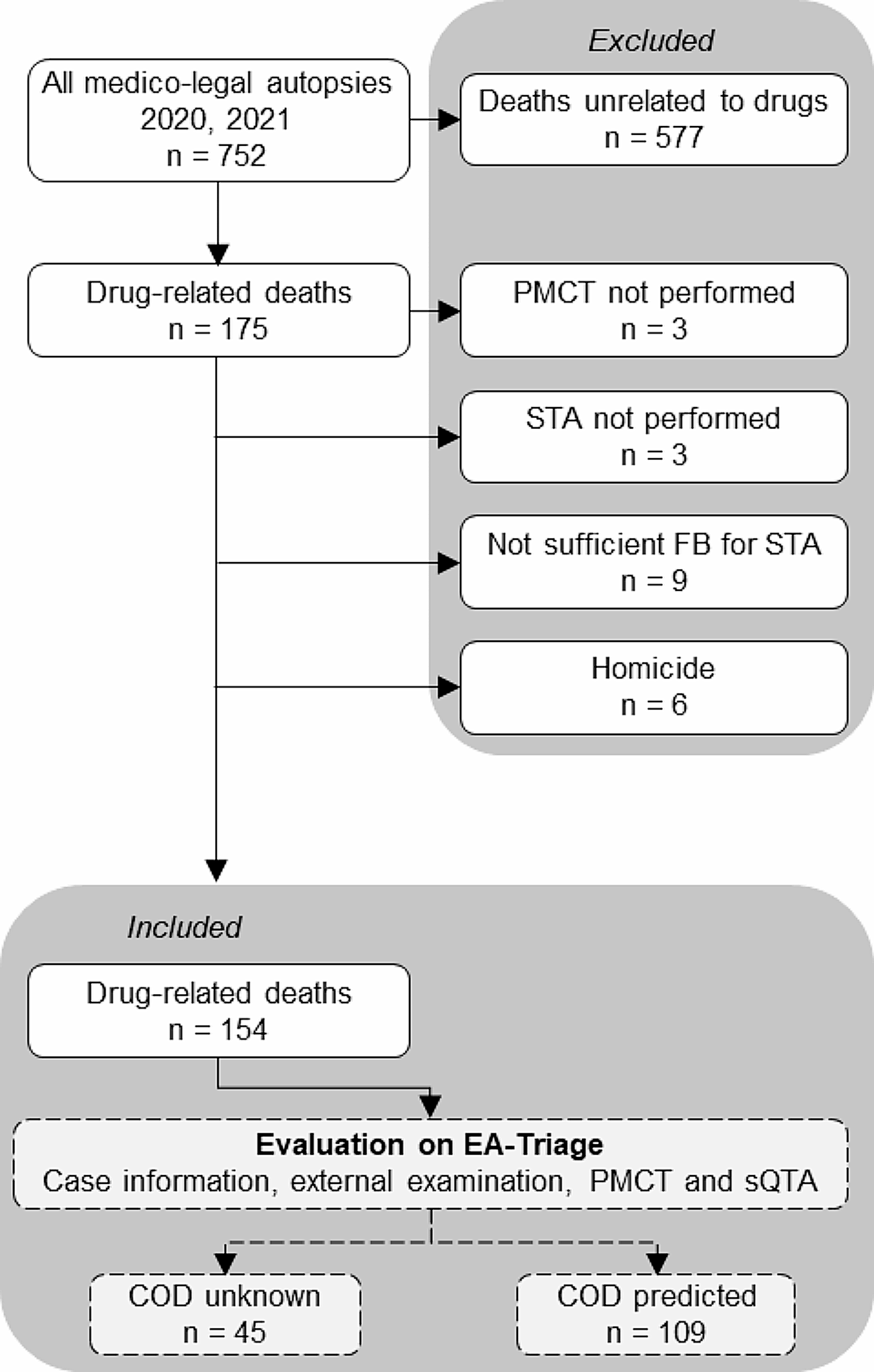
In other subgroups, the use of EA-Triage might be more complex. Previous studies on the use of PMCT for nontraumatic deaths have shown poor diagnostic accuracy. Femia et al. reported only 35% agreement on COD in unexplained deaths between PMCT and conventional autopsy [24]. PMCT was considered beneficial only for neurological, traumatic, and gastrointestinal deaths. We also found that EA-Triage had a greater proportion of patients with an unknown COD (29%) than did medico-legal autopsy (3%). Cases with an unknown COD were mostly natural deaths due to disease, suggesting that in this subgroup, it could be difficult to predict a COD based only on EA-Triage. Therefore, other screening techniques could be considered relevant to preautopsy investigations for natural deaths. Femia et al. also showed that postmortem computed magnetic resonance (PMMR) identified COD in 50% of suspected cardiac and neurological deaths compared to 35% identified by PMCT [24]. In another study of cardiovascular deaths, compared with unenhanced PMCT, contrast-enhanced PMCT increased the agreement on COD from 65 to 95% [25].
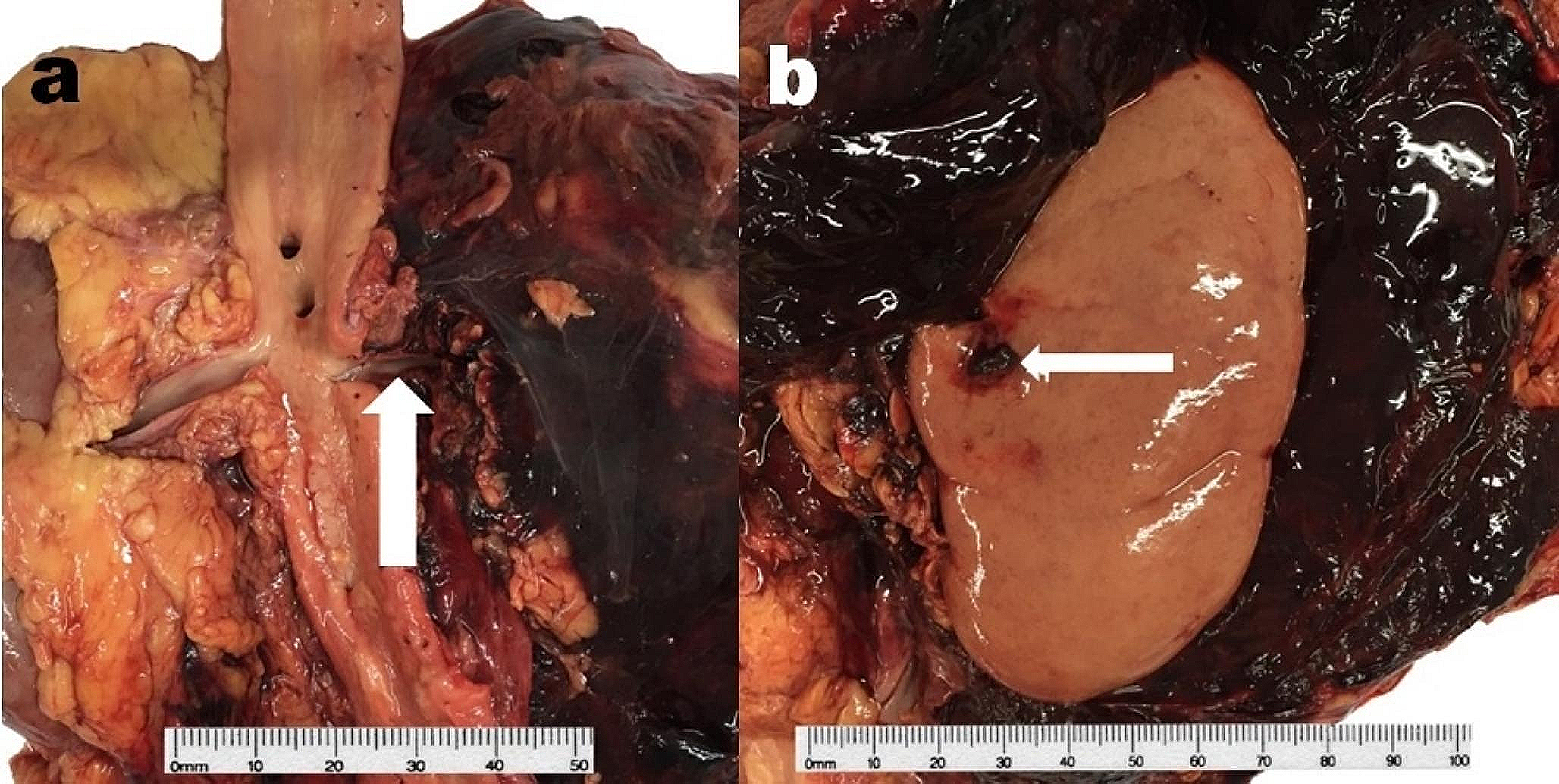
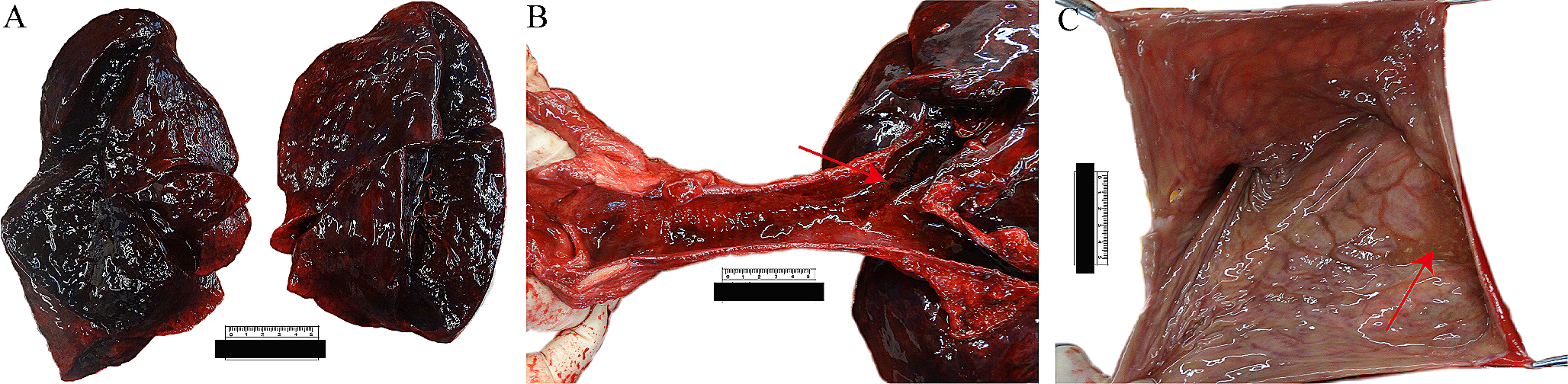
Drug-related deaths are frequently nontraumatic on PMCT, and lethal concentrations of drugs is detected in postmortem blood. PMCT can be used to rule out injuries and serve as a screening tool to exclude any traumatic involvement incompatible with the case circumstances. Additionally, resuscitative efforts, e.g., rib fractures compatible with the case circumstances, can be identified. Combined with QTA, which can detect and quantify the most common lethal intoxications within 24–48 h, the ability to determine COD was comparable to that of conventional autopsies in this subgroup. Thus, EA-Triage has the possibility to accurately predict COD prior to autopsy in selected subgroups. This approach could guide police investigations at an early stage, minimize the burden of family members and offer an alternative in cases where autopsy is refused, e.g., those where it is prohibited by religious beliefs.
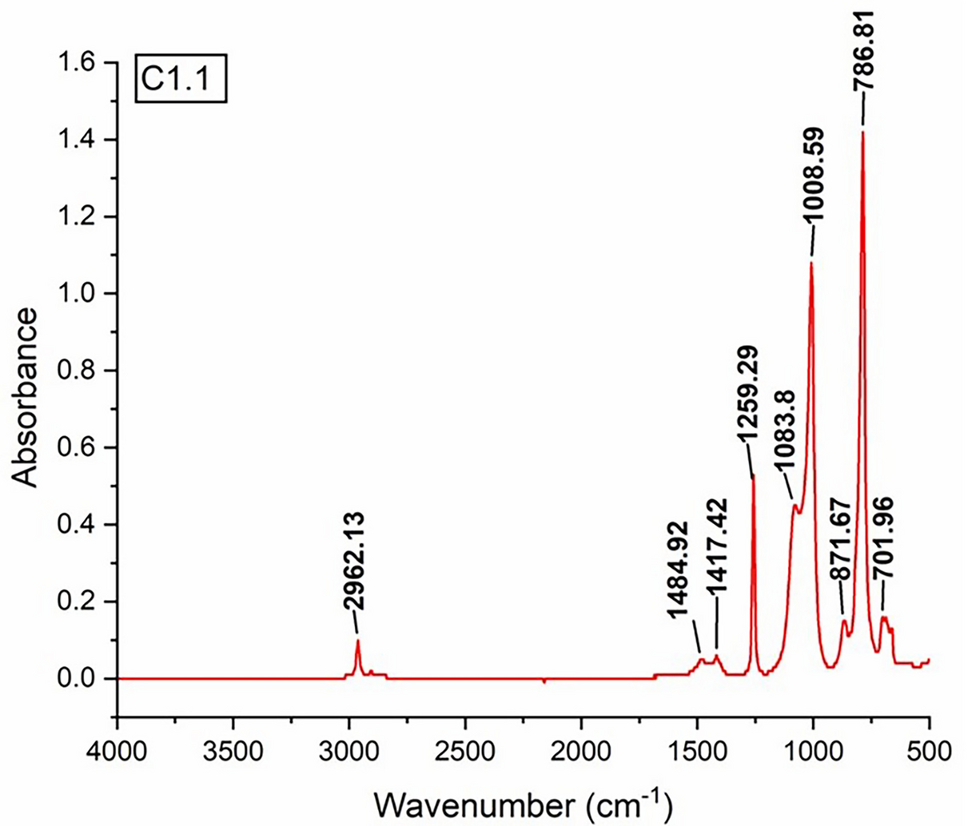
sQTA identified most lethal intoxications in the present study (94%). However, it was not suitable for cases with suspicion of the use of volatiles, designer drugs or uncommon drugs. Volatiles require further analysis upon request based on circumstances, and the remaining drugs would be detected in the qualitative screening. In one case of suspected intoxication with insulin, neither sQTA nor STA would have been able to detect exogenous insulin, and the COD was determined from case circumstances with strong indications of excess insulin intake. QTA was originally designed for clinical purposes in the emergency department, where it is acceptable that reliability can be compromised if treatment is necessary for preventing death. QTA in a forensic setting requires high reliability because the results must be valid in a legal setting. Standard toxicological analysis always includes verification of the screening results with a different technique, meaning that behind a reported result, there are two different analyses carried out by different technicians, usually on different subsamples. This procedure lowers the risk of sample mix-up and the reporting of false-positive results, which should not be neglected as a limitation of QTA. Simultaneous testing of postmortem urine, cardiac blood or vitreous humor as well as femoral blood could verify the analytical results and toxicological assessment, increasing the reliability of QTA. The sampling of postmortem FB can be challenging due to decomposition and low blood volume. The technique is well known from studies on PMCT angiography but will not be further addressed here [26]. However, to ensure that all forensic concerns are met, there should always be recommendations for medico-legal autopsy in cases without sufficient material or quantitative results explaining the COD.
EA-Triage may contribute substantial value to preautopsy COD determination in the subgroup of drug-related deaths. The agreement between EA-Triage and conventional autopsy for cases with nonsuspicious circumstances was 99%. The discrepancy in COD arose in one case of competing CODs. This case was determined to be intoxication with prescription drugs by EA-Triage; however, the medico-legal autopsy microbiology analysis revealed sepsis. EA-Triage missed this competing COD and potentially other natural CODs, such as certain cardiovascular events, uncommon intoxications, and other bacterial infections, if there was no history to suggest this possibility. In cases with no indication for further examination, there is also a risk of incorrect determination of COD during conventional autopsy. For drug-related deaths, competing CODs rarely occur. However, the expansion of EA-Triage to other groups at the medicolegal inquest could improve the selection for medico-legal autopsy. Some cases may not need an autopsy according to national legislation and guidelines. In others, the possibility arises that EA-Triage results would determine an unforeseen need for autopsy, prompting selection of the “proper” forensic population for conventional autopsy. Retrospective studies, such as this one, are the first step toward implementing triage of the complete forensic population. Implementation of EA-Triage will be possible once QTA has been validated in a forensic setting. The anticipated challenges of implementation include logistics and geographic considerations, as well as the likelihood of additional costs and workload. These factors should be taken into account during the implementation phase.
When comparing the experience of implementing screening tools prior to autopsy, generalization should be performed with caution. The use of different populations and selection methods for autopsies limits the ability to compare countries. At the Department of Forensic Medicine, AU, one-third of medico-legal autopsies are intoxication cases, but in other countries, firearm fatalities and homicides may be more prevalent. Although our findings support previous research on the high agreement in COD when comparing PMCT and QTA with conventional autopsy for drug-related deaths, this agreement might not be as high for other subgroups of the Danish population or other forensic populations. Further research and experience in this area are needed to determine the accuracy of COD determination obtained from conventional autopsies.
Limitations of our study included the selection of drug-related cases. It would have been optimal to have prospectively selected cases in cooperation with the deciding police officer at the current medico-legal inquest. Instead, the study group was based on an in-house coding system of drug users, and since the coding was registered after the results of the STA, some cases may have been irrelevant in a prospective scenario (e.g., traumatic deaths). Another limitation of the retrospective study design was the variation in case material available from ongoing cases during a medico-legal autopsy compared to the summarized material presented at the EA-Triage setup. This resulted in fewer details in ICD-10 coding compared to the original COD coding from the medico-legal autopsy. A conservative diagnostic approach was applied because any suspicious case circumstances, regardless of the results from EA-Triage, led to recommendations for medico-legal autopsies. This likely led to an overestimation of suspicious cases recommended for medico-legal autopsy. However, a conservative approach must be advised in this stage of research. Testing the ability of EA-Triage to assess manner of death was not the focus of this study; however, determination of manner of death is important to close a forensic case without autopsy.



留言 (0)