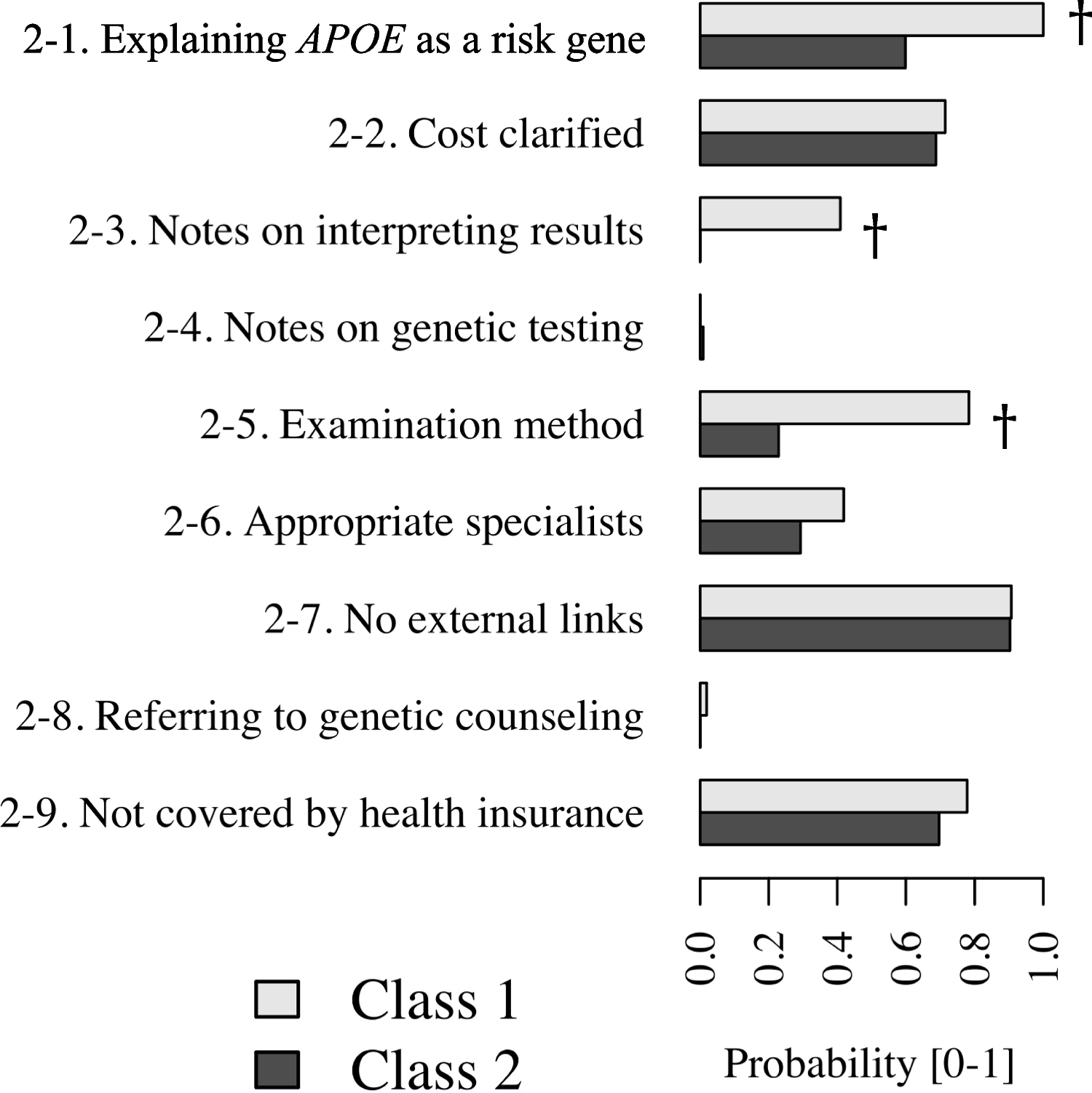
We analyzed the websites of 220 medical facilities advertising APOE genetic testing in Japan. As a result, most websites met the following regulatory requirements for posting APOE testing advertisements: contact information, details, testing costs, and a statement indicating that the tests are not covered by health insurance. The description of “examination methods” (e.g., blood sampling) or “notes on interpreting APOE results” varied significantly among facilities. References to “notes on genetic testing” and “genetic counseling” were infrequently mentioned, and “specialists with appropriate expertise” were reported to be involved in clinical practice in approximately one-third of these facilities providing APOE testing services. These results suggest that self-determination and its quality of APOE testing at some of these medical facilities in Japan could potentially be compromised, at least regarding patients’ initial decisions on whether to undergo testing.
Although all facilities met the contact information criterion (Tier 1–1) and the majority also provided details or costs of APOE testing (Tier 1–2), which are legal requirements for lifting restrictions on medical advertisements, with compliance rates of 100% and 94.5%, respectively, we should not overemphasize the findings of Tier 1–2 or Tier 2–1. This caution is due to our study’s aim, which was not to rigorously assess each individual website advertisement’s compliance with legal requirements. Furthermore, the observed reliability was only moderate to fair, and the lower bounds approached zero, potentially resulting from our broad definition of eligibility for Tier 2–1 in the manual search.
Tier 1–3 criteria were met in only half of the facilities with substantial reliability. This may be attributable to two reasons: (i) the possible risk of harm to patients (e.g., increased anxiety or depression levels (Green et al. 2009; Bemelmans et al. 2016; Alber et al. 2022)) following the disclosure of results may not be sufficiently acknowledged, and (ii) the invasiveness of specimen sampling for APOE testing (e.g., sampling of blood, hair, or buccal mucosa) is limited. According to the English translation of the Medical Care Act by the Ministry of Justice, legal requirements for lifting advertising restrictions include providing “information on particulars pertaining to major risks and adverse reactions, etc., by medical care not covered by health insurance.” Although the harmful risk level following APOE result disclosure may not be “major,” if such risks are under-recognized or overlooked by clinicians, they may overlook the necessity that they should describe its risks and adverse effects on their websites.
Approximately one-third of the facilities advertising APOE testing reportedly involved specialists with the appropriate expertise (Tier 2–6). This figure might be an underestimation since the determination of specialist involvement was based solely on the presence of clinician names on the website, without considering their actual employment status. Furthermore, such a limited proportion of specialists involved raises concerns about the adequacy of explanations regarding the testing’s significance and whether notes on genetic testing (Tier 2–3) are provided to patients before and at the time of result disclosure. Moreover, our findings suggest that dementia experts may be more hesitant to conduct APOE testing compared to their counterparts, inferred from the lower proportion of specialists versus non-specialists and the general clinician demographic in Japan. This reluctance may be informed by clinical practice guidelines for dementia that do not advocate routine APOE testing (Japanese Society of Neurology n.d.) and by another set of guidelines that recommend APOE testing after thorough consideration of its validity and utility (The Japanese Association of Medical Sciences n.d.; Ethical guidelines for medical and biological research involving human subjects n.d.). Similarly, a hesitance among genetic specialists to engage in APOE testing is also suspected; geneticists were rarely seen during our website review, although we have not noted them statistically. This indicates that a significant amount of out-of-insurance APOE testing at Japanese medical facilities may occur without the involvement of genetic specialists.
Genetic counseling was infrequently mentioned (Tier 2–8, 0.9%). It is indeed not required to be posted by the guideline of medical advertisements and is also not always required to be provided in the actual practice by the current guidelines on genetic testing (The Japanese Association of Medical Sciences n.d.; Ethical guidelines for medical and biological research involving human subjects n.d.) where clinicians or researchers are only to consider the necessity of genetic counseling for testing of susceptibility genes. However, because the proportion of specialists enrolled was relatively low, the necessity may not always be considered appropriately, which is another matter of concern. Furthermore, the shortage of medical facilities offering genetic counseling in Japan, for a range of conditions beyond APOE, could be a contributing factor to this deficiency.
The advertisement on APOE testing is occasionally accompanied by descriptions of benefits of testing, such as “APOE genetic testing is useful in understanding the future risk of dementia to prepare for its prevention.” However, we did not analyze such appealing expressions here. The clinical utility of drug intervention with DMT to prevent AD or dementia, or the clinical utility of multifactorial interventions, including management of vascular risk factors (e.g., hypertension, diabetes, and dyslipidemia), nutritional guidance, and exercise training (Ngandu et al. 2015; Solomon et al. 2018), has not been established so far. We are concerned that advertisements describing benefits of APOE testing may be overstated, depending on how they are described.
Our study had several potential shortcomings. First, we do not know how APOE testing is explained and conducted in actual clinical practice in each facility. The poor explanation in the website advertisement does not always mean that the in-person information provided to patients is poor. In addition, we examined facilities that made advertisements on their websites, so we could not examine those providing the testing service without doing website advertisement. In addition, this study focuses on the appropriateness of the advertisement, which has limitations in its scope in discussing how to support well-informed self-determination on whether to take the test.
Second, although we had to rely on publicized certifications to distinguish individual clinicians’ expertise, clinicians with a certification in the specific expertise areas related to dementia treatment may not always be familiar with APOE testing. In addition, even in the case of clinicians without specific certification testing, the actual conditions may differ between general internal medicine clinics and out-of-insurance beauty clinics, which we could not examine here.
Third, the inter-rater reliability for some features was not consistently sufficient, especially concerning “explaining as a risk gene” (i.e., Tier 1–2, 2–1), which may be because of its broadly defined yet somehow unspecified criteria. We may need to refine definitions, or to introduce another feature with a narrower scope. Additionally, adjusting the number of sampled websites to evaluate the kappa coefficient may be warranted, given that the assumptions made in the sample size calculation may not be robust. Incorporating adjustments for demographic factors, such as location or years of experience, may also be beneficial during sampling.
Lastly, we were unable to assess the quality of APOE testing provided by individual medical facilities, as such information is not ascertainable through website descriptions. The testing’s accuracy, which plays a crucial role in the interpretation of APOE results, may vary among facilities, because they usually outsource their testing to different companies. Including details about the testing methods and their reliability on the websites could prove to be beneficial.
Although current clinical practice guidelines do not routinely recommend APOE testing in medical practice, it is conceivable that APOE testing might become more widely used in the near future. Its use would not only be limited to stratifying patients according to the risk of developing ARIA before starting DMT treatment (Cummings et al. 2023), but could also promote health-related behavioral changes in individuals with the ε4 allele[s] (Marshe et al. 2019), such as managing potentially modifiable risks of AD (e.g., smoking, social isolation) (Livingston et al. 2020), or facilitating the recruitment of at-risk individuals to AD prevention trials (Langbaum et al. 2019; Fockler et al. 2021; Ryan et al. 2021).
Integrating APOE testing by DTC services into medical care services may potentially be advantageous, serving as a complement of out-of-insurance APOE testing at medical facilities before starting treatment with DMT. In Japan, a single medical facility is prohibited from offering a combination of treatments that are both covered and not covered by public health insurance for the same disease. For such cases, it is essential to provide DTC users with adequate information about APOE testing, facilitate their access to genetic counseling upon request, and ensure the quality of sample collection and testing procedures. These are critical concerns that need specific attention and evaluation in the future. This is not only true for the APOE testing, but also for other genetic tests available in DTC services.
In conclusion, our analysis revealed that the features of website advertisements varied among individual facilities. Additionally, only about one-third of these facilities had specialists with the appropriate expertise involved in their practices. These results suggest that the self-determination of patients regarding APOE testing could be improperly influenced by some medical facilities in Japan, particularly at the initial decision-making stage. Therefore, it is necessary to further discuss how and to what extent information about APOE testing should be conveyed to patients through medical facility website advertisements.


留言 (0)