
記住我

There are 27 reference centers for the management of patients with rare diseases in Brazil, and the Instituto Nacional de Saúde da Mulher, da Criança e do Adolescente Fernandes Figueira (IFF) in Rio de Janeiro is one of them. Patients with rare eye diseases are managed in ophthalmic centers, and those with a suspected genetic etiology are referred to rare disease reference centers. However, it is estimated that only 30% of all patients with rare diseases requiring clinical evaluation by specialized professionals receive an evaluation, representing a bottleneck toward the final genetic diagnosis of patients with rare eye diseases, such as pediatric cataracts [16]. In this scenario, the government pays up to 620 USD per year for the management (diagnosis, treatment, and rehabilitation) of a patient with any rare disease [21].
The Instituto Nacional do Coração (INC) in Rio de Janeiro is conducting an ongoing national research project for the diagnosis of suspected hereditary cardiovascular diseases (The Brazilian National Network of Cardiovascular Genomics) [22] and, in addition, performs molecular diagnoses of other genetic diseases. The INC and IFF established a partnership for testing for genetic diseases, where the IFF sends DNA samples from patients with rare diseases for next-generation sequencing to the INC.
Study design and perspectiveThis study is a cost analysis study of suspected hereditary pediatric cataract genetic diagnosis through the SUS perspective. We performed a mixed costing analysis, using reimbursement data to estimate the cost of clinical diagnosis and a microcosting approach with a bottom-up technique to estimate the cost of genetic diagnosis. The latter approach was used because genetic testing via WES for ocular diseases is not currently available in clinical practice in the SUS. The bottom-up technique uses detailed activity and input usage data from records or from observation (as in this study) at a health care service to estimate unit costs [23]. In our case, we obtained data from the observation of a sample of suspected hereditary pediatric patients who underwent WES. The analysis was performed using Excel 365 software (Microsoft, USA).
Population and settingThe eligible population included all patients with pediatric cataracts up to 18 years old in Rio de Janeiro and two additional family members, as our study included trio analysis for WES. The population estimate included epidemiological incidence and prevalence data for the first year of the economic model and incidence data for each of the 4 subsequent years, given the 5-year time horizon. We included a pediatric cataract cumulative incidence of 3.46:10,000 for the 15-year interval [24] and a congenital cataract incidence of 4:10,000 [3]. We assumed that the prevalence of pediatric cataracts would be the same as that of congenital cataracts, and we assumed that the cumulative incidence for 15 years would remain the same up to 18 years of age. We considered that 76% of the population uses the SUS, based on official governmental data from Brazil [25].
To identify and quantify health resources, a sample of patients with familial pediatric cataracts from the CATBRA study was used. The CATBRA study, a Brazilian study for genomic evaluation of suspected hereditary pediatric cataract patients (protocol code 21444619.0.0000.5269), aims to identify variants associated with suspected hereditary pediatric cataracts, to analyze the impact of the disease on the management of these patients and families, and to perform a budget impact analysis of WES for pediatric cataracts. The eligible population of the CATBRA study included one hundred and ten participants from twenty-nine different families within a cohort of pediatric cataract patients from a nonprofit health organization dedicated to the management (diagnosis, treatment and follow-up) of pediatric cataracts in Rio de Janeiro, Brazil [26]. The inclusion criteria were patients up to 18 years old with a history of pediatric familial cataracts in any family member, such as parents, siblings, grandparents, uncles or cousins. The exclusion criteria included a history of congenital TORCH infections (toxoplasmosis, rubella, cytomegalovirus, herpes simplex, syphilis, varicella zoster, or Zika) and the use of corticosteroids or ocular trauma.
This study was justified by the opportunity to carry out a cost analysis nested within the aforementioned study and by the possibility of identifying the causative variants of pediatric cataracts in the same family.
We considered pediatric cataracts to include those that appeared at birth (congenital cataracts) and those that appeared during infancy (childhood or infantile cataracts).
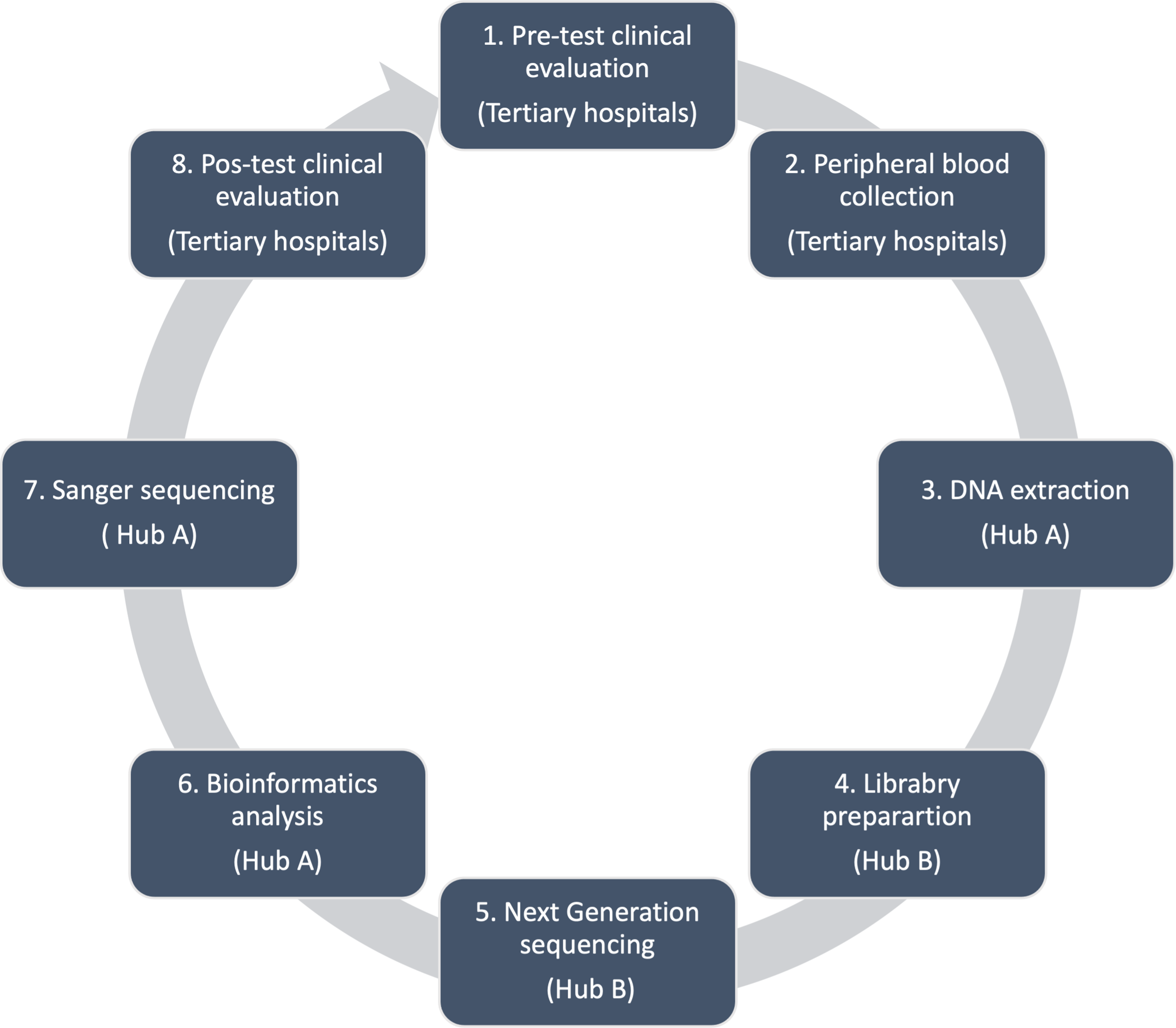
TechnologyThe genetic diagnosis of pediatric cataracts via WES was evaluated. The diagnostic protocol was divided into 8 steps to estimate the cost of each step (Fig. 1). A theoretical network of the 12 main governmental tertiary hospitals in the city of Rio de Janeiro with pediatric cataract patients eligible for ocular genetic testing was created, and two facilities (A and B) responsible for genetic testing were selected as hubs (Fig. 2). The steps were as follows:
Fig. 1
Diagnosis protocol for pediatric cataract patients comprising 8 steps: pre-test evaluation, peripheral blood collection, transportation of biological material, DNA extraction, library preparation, next-generation exome sequencing, bioinformatic analysis, Sanger sequencing, and post-test clinical evaluation
1.The pre-test clinical evaluation included two clinical ophthalmologic consultations and one clinical genetic consultation. The clinical diagnosis process included ophthalmic exams (slit-lamp biomicroscopy, intraocular pressure, indirect ophthalmoscopy, ocular ultrasonography and biometry for axial length measurement) and clinical genetic evaluations (family history, origins and pedigree; existence of other systemic conditions; and clinical‐morphological evaluation) [27].
2.Peripheral blood sample collection from eligible patients with pediatric cataracts and their family members was performed at each of the 12 tertiary hospitals (Fig. 2).
3.Genomic DNA extraction and evaluation of the quantity and quality of the genomic DNA from the peripheral blood sample were performed at hospital A (IFF).
4.Library preparation refers to the preparation of DNA for high-throughput sequencing of the exome, which was performed at facility B (INC).
5.WES, which involves sequencing of the protein-coding regions of the genome, was performed at facility B (INC).
6.Bioinformatics analysis included the use of computational tools and techniques for remote interpretation of WES data by an expert team.
7.Sanger sequencing for the validation of suspected pathogenic variants was performed in facility A (IFF).
8.The post-test clinical consultation included one clinical genetic consultation for genetic counseling and care at tertiary hospitals (Fig. 1).
Additionally, we estimated the operational cost of this process, which included administrative and logistic functions and biologic material transportation.
Fig. 2
Twelve governmental tertiary hospitals with pediatric cataract patients eligible for ocular genetic testing in the city of Rio de Janeiro (Fig. 2). Hospitals A and B were selected as hubs
Cost analysis scenariosWe estimated the cost of genetic diagnosis of pediatric cataracts in two scenarios. The first scenario, our reference scenario, included patients with pediatric cataracts and two family members (one affected and one unaffected) in the city of Rio de Janeiro. We assumed that trio analysis was needed for WES.
The second scenario, an alternative scenario, was created to estimate the minimal cost of WES with the hub working with maximum capacity. Currently, hospital B (INC), which sequences multiple cardiac genetic diseases, such as hypertrophic cardiomyopathy, within the research budget, has an Illumina NovaSeq 6000 sequencer [22]. Like for pediatric cataract cases, there is no reimbursement expected for genetic testing for cardiac diseases within the SUS [22]. Given that the sequencer has an annual capacity (63,360) of almost eight times the annual pediatric cataract demand in Rio de Janeiro (approximately 8,000), it should not only be used for pediatric cataracts but also for sequencing patients with other genetic diseases. The monthly capacity of the sequencer was determined based on the following characteristics: 2 × 100 bp coverage with two S4 flowcell plates with 240 samples each run for 36–48 h, 22 days per month ([240 samples per plate × 2 plates × 22 workdays in a month]/2 days, which is the longest duration of sequencing).
Costing modelFollowing the Brazilian Guideline for Budget Impact Analysis [28], we considered a five-year time horizon, with the first year costs including the acquisition and maintenance costs of the equipment plus consumables and staff and the second, third, fourth, and fifth years including consumables, staff and equipment maintenance costs.
The costs of pre-test clinical evaluation (step 1), post-test clinical evaluation (step 8) and complementary exams, such as ocular ultrasonography and biometry (step 1), were based on the SUS reimbursement table of ambulatory procedures [21]. This table provides the total reimbursement cost of the procedure, including consumables, staff and equipment costs.
The costs of the other steps are not provided by the above mentioned table and were estimated through the microcosting technique [21]. Peripheral blood sample collection (step 2), genomic DNA extraction and evaluation of genomic DNA quantity and quality (step 3), library preparation (step 4), exome sequencing (step 5), bioinformatics analysis (step 6), Sanger sequencing (step 7) and operation were estimated based on direct observation of the genetic testing performed in the one hundred and ten participants of the study, enabling us to list all the resources used.
Every step of the genetic testing protocol was parsed into an Excel spreadsheet to identify, quantify, and value each item used in the procedure. The cost of each step included the costs of disposable consumables, equipment and hands-on staff time. If available, components were priced using an official database [29]. Otherwise, the products were priced according to the manufacturer or wholesale supplier (Thermo Fisher Scientific, Sigma‒Aldrich, Illumina, Promega, Eppendorf). Overhead costs, including water, cleaning, electricity, safety, the internet, food and administrative items, were assumed to constitute a total of 10% of the cost per exam and were included in the operational step costs. Usually, overhead costs range between 20 and 30%; we assumed the lower rate because the facility’s infrastructure already existed.
Consumable costs were reduced to a per-unit cost (per exam). To estimate each step’s cost, the necessary item cost per unit was listed and multiplied by the minimal batch quantity needed for the eligible population. Given that reagent kits and some disposable consumables are available only in batches of a minimal quantity, if there is one additional patient above the minimal batch quantity, it will be necessary to buy another batch.
To estimate the equipment cost, we listed all the equipment used and distributed it between the two main facilities (A and B) according to the above steps. We assumed that the Illumina NovaSeq 6000 sequencer (facility B - INC) would work well, analyzing 5,280 samples monthly, as explained in the ‘scenarios section’, in both the reference and alternative scenarios. For other equipment, we estimated the quantity needed to perform 5,280 samples monthly, assuming maximum performance in a 40-hours/week workload, for 22 days per month (supplemental material). Equipment was priced according to the manufacturer or wholesale supplier. We did not use a straight-line depreciation rate because it is not included in the Brazilian Guidelines [28]. We considered the acquisition cost in the first year, and the maintenance cost in every year. Annual maintenance was estimated at 5% of the equipment cost [30].
To estimate the cost per step if one piece of equipment from the same facility was used in more than one step, we used a pro rata distribution to adjust its cost by the equipment usage percentage compared to the other steps. For instance, the Thermo Fisher QUIBIT is used in steps 3, 4, 5 and 7 but is used more frequently in step 5. Therefore, we assumed that its percentage of use in these steps would be 20%, 20%, 40% and 20%, respectively. In contrast, NanoDrop 8 is used in steps 3 and 7; we assumed its percentage of use as 50% for each step. The distribution is available in the supplementary material.
The annual salary of each personnel job class was obtained from hospital A, as this ward was responsible for the main steps. To obtain the real annual salary, the monthly wage was multiplied by 14.3 in accordance with the Brazilian Labor Law. This adjustment included 1/3 of the monthly salary for vacation, a thirteenth of the salary for December and a one-month payment for a staff substitute during mandatory vacation. We assumed a 40 h per week workload and 52 weeks per year. The personnel performed the specific step for 6 h a day, with the remaining 2 h for computer work and lunchtime. We estimated weekly, monthly and annual productivity per personnel according to the hands-on time per step.
If a suspected pathogenic variant was found during WES in CATBRA study, we performed Sanger sequencing for the single gene. With respect to the model, we assumed that half of the patients would need Sanger sequencing.
The logistic cost included the cost of transporting patient blood samples from tertiary hospitals to hub hospitals. Hospital A (IFF) received the samples to perform DNA extraction, library preparation and, after WES, Sanger sequencing for confirmation of pathogenic variants. Next, hospital B (INC) received the products for library construction and WES.
In our reference scenario considering pediatric cataract patients, we assumed the frequency of transportation based on the activity of each pediatric ophthalmology department. Hospitals with lower activity would need transportation once every 3 months; hospitals with moderate activity would need transportation once a month; and hospitals with high activity would need transportation twice a month. The Google Maps platform was used to calculate the distance among the units, assuming a car performance of 8 km per liter for the gasoline cost estimator. We also assumed that it would be possible to use one of the available vehicles at hospital A. Staff included one hired driver for these periods.
We considered the exchange rate to be 1.00 USD = R$5,1686 (from January 2022-June 2023) [31]. Model data are available upon request.
OutcomesThe primary outcome was the cost per genetic of diagnosis of suspected hereditary pediatric cataracts via WES. The secondary outcome was the cost per step.
EthicsThe study was approved by the Ethics Committee of INSTITUTO FERNANDES FIGUEIRA-IFF/FIOCRUZ‐RJ/MS (protocol code 21444619.0.0000.5269), 17 October 2019.
Sensitivity analysisWe conducted a one-way sensitivity analysis for fluctuations in the unit costs of the most expensive consumables (+ 30% and − 30%), staff (+ 30% and − 30%) and equipment (+ 100% and − 20%). The choice of these range values was justified by the absence of studies estimating the cost of WES for familial pediatric cataracts within the SUS, so we used range values from another ocular disease [30, 32]. As in our reference and alternative scenarios, the equipment costs were estimated considering the high capacity of the equipment, and we also estimated the cost of genetic testing if all the equipment was used only for pediatric cataract patients and their families. In addition, we performed sensitivity analysis using an overhead range of 20–30%.
留言 (0)