
記住我
Duodenal cancer stands as the leading cause of cancer-related mortality in individuals with familial adenomatous polyposis (FAP) (1). While endoscopic surveillance is crucial for managing duodenal cancer, determining interventions based on endoscopic findings remains challenging. In response to this challenge, the Spigelman staging system, introduced in 1989 (2), has gained widespread adoption due to its simplicity, reproducibility, and ability to monitor disease progression across 4 stages.
In recognizing a greater cancer risk at higher stages, patients with stages 0–III receive increasingly frequent surveillance intervals. By contrast, aggressive cancer prevention measures, such as prophylactic duodenectomy or intensive endoscopic downstaging, are reserved for those at stage IV (3–6). However, the effectiveness of the Spigelman staging system in predicting the risk of duodenal and papillary cancers and identifying precancerous stages has mainly been evaluated in small-scale studies. Furthermore, due to insufficient follow-up, uncertainty remains regarding whether endoscopic downstaging represents an alternative to surgery in reducing cancer risk (7). In addition, there is a possibility that additional risk factors of duodenal and papillary cancers have emerged since Spigelman's original formulation. Bridging this knowledge gap is crucial because the surveillance intervals, timing of prophylactic surgery, and overall management of duodenal cancer risk all rely on the Spigelman stage.
To address these crucial issues, we conducted a comprehensive systematic literature search with 3 primary objectives. First, we aimed to assess the risk of duodenal and papillary cancers at each of the 4 Spigelman stages. Second, we sought to measure the sensitivity of the Spigelman staging system. Last, we aimed to identify additional risk factors that contribute to the development of duodenal and papillary cancers beyond those currently in the Spigelman system.
METHODS Systematic searchesWe conducted a systematic literature search across multiple databases: PubMed, Cochrane, EMBASE, and MEDLINE. The search spanned from January 1, 2006, to May 2023. Manual searches were also conducted to identify additional publications (see Supplementary Tables 1–3, Supplementary Digital Content 1, https://links.lww.com/AJG/D191). Duplicate entries and non-English articles were excluded. To ensure an unbiased evaluation, 2 authors (A.M. and G.M.C.) independently and blindly screened the titles and abstracts and subsequently assessed the full-length articles. In cases of disagreement, a third independent opinion (M.P. or G.M.) was consulted.
Outcomes of interestWe extracted information on 3 outcomes of interest: the cancer risk by stage, sensitivity of the Spigelman system, and risk factors of cancer development. This included information on the Spigelman stage and its individual components. Within this review, we distinguished between duodenal and papillary cancers.
Assessment for bias and heterogeneityAll studies included were case-control or cohort studies; therefore, we used the Newcastle-Ottawa Quality Assessment Scale, which evaluates studies on 3 domains: selection, comparability, and exposure/outcome (8). Each article was independently and blindly evaluated for the risk of bias by 2 authors (A.M. and G.M.C.), and in cases of disagreement, a third independent opinion was sought (M.P. or G.M.).
Selection criteria and synthesis methodsData from the included studies were collected by 2 authors and merged after reaching an agreement on the content and interpretation. Articles were included if they met our inclusion/exclusion criteria (see Supplementary Table 4, Supplementary Digital Content 1, https://links.lww.com/AJG/D191) and were categorized into 3 domains: cancer risk by stage, sensitivity, and risk factors.
In brief, studies that provided explicit information on the number of patients with Spigelman stages 0, I, II, III, and IV, the duration of follow-up, and the occurrence of incident duodenal, papillary, or either cancer were analyzed to determine the cancer risk in each Spigelman stage.
To assess the sensitivity of Spigelman stage IV in detecting cancer, we included studies that reported the Spigelman stage during papillary, duodenal, or either cancer diagnosis. Finally, studies reporting risk measures for duodenal or papillary cancer were examined to identify the most significant risk factors contributing to their development.
Because we anticipated between-study heterogeneity, a random-effects model was used to pool effect sizes. For proportions, we used the inverse variance method, while for risk and odds ratios, we used the Mantel-Haenszel method without continuity correction for zero cells (9–12). For proportions, the confidence intervals (CI) for individual studies were calculated with the Clopper-Pearson method. The restricted maximum likelihood estimator and the Paule-Mandel method were used to calculate the heterogeneity variance τ2 for proportions and for risk and odds ratios, respectively (13,14). In addition, given the small number of studies and the risk of heterogeneity, we applied the Knapp-Hartung adjustments to calculate the CI around the pooled effect (15). All statistical analyses and visual processing were conducted in R (16–20).
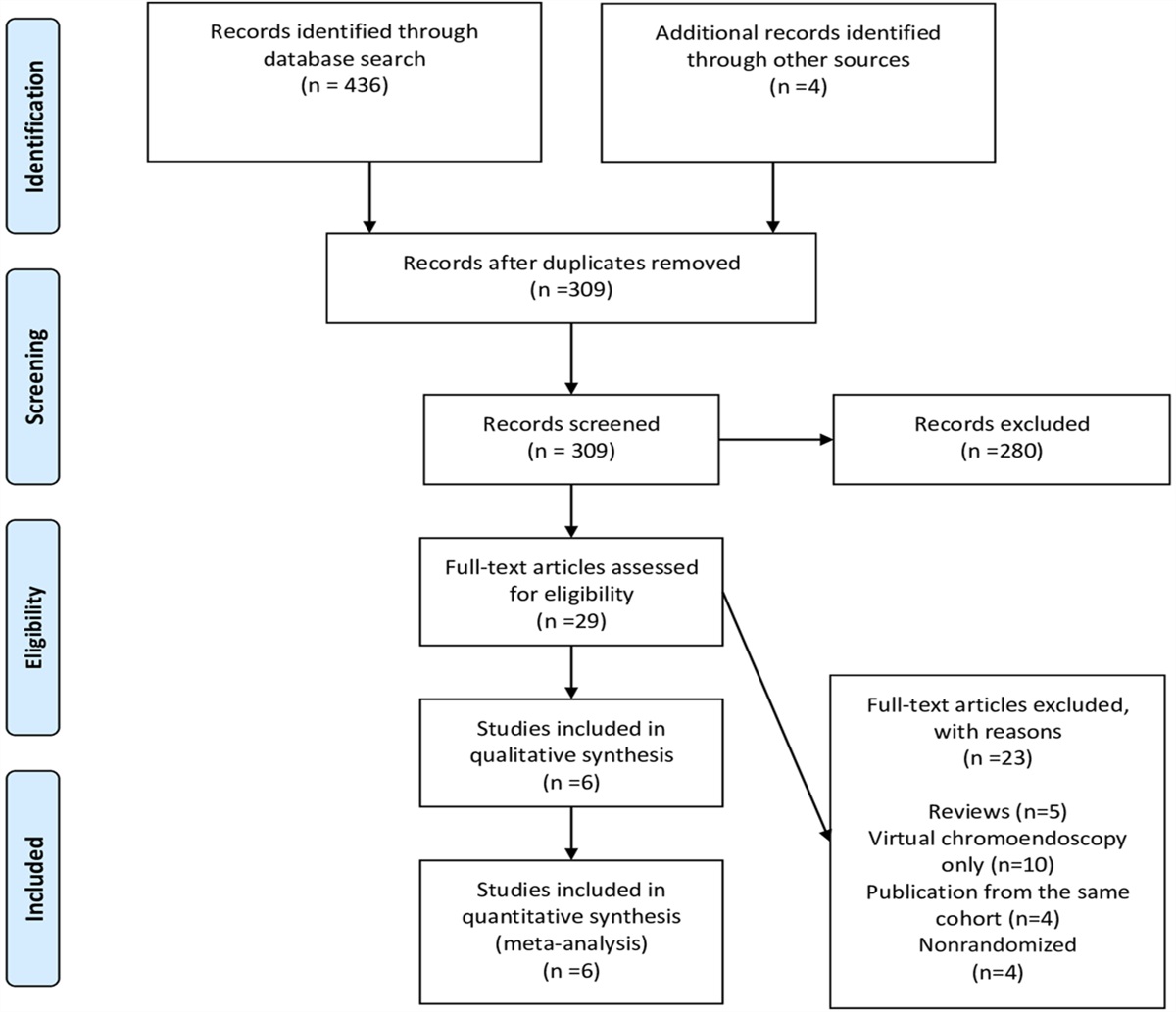
RESULTS Systematic review resultsOur systematic review was Preferred Reporting Items for Systematic Reviews and Meta-Analyses compliant and yielded 1,960 entries from multiple databases. After removing duplicates (774) and non-English articles (16), 1,170 article titles and abstracts were screened, and 150 articles were selected for full-text review. Ultimately, 27 articles were identified as relevant and contributed to the writing of this review (Figure 1). The design, study population, and risk of bias are summarized in Supplementary Table 5 (see Supplementary Digital Content 1, https://links.lww.com/AJG/D191).
 Figure 1.:
Figure 1.: Systematic review flowchart.
Duodenal and papillary cancer risks by Spigelman stageNine studies assessed the risk of duodenal and papillary cancers according to the Spigelman stage (Figure 2) (7,21–27). As anticipated, the risk of duodenal cancer progressively increased with each successive Spigelman stage.
 Figure 2.:
Figure 2.: Pooled risks of developing duodenal cancer, papillary cancer, or either cancer, for Spigelman stages 0, I, II, III, and IV. Squares of different sizes represent different weights. Total refers to the total number of patients with Spigelman stage 0, I, II, III, or IV in each study. N refers to the number of patients developing duodenal cancer, papillary cancer, or either cancer. CI, confidence interval; NA, not available: Singh et al reported only on the risk of papillary cancer, and therefore, data from this study were used for papillary cancer risk evaluation only.
After pooling results from 1,097 patients with FAP, we estimated a very low risk of duodenal and papillary cancers for patients in stages 0 and I, non-negligible cancer risk for Spigelman stages II and III (6% [95% CI 2%–16%] and 5% [95% CI 2%–13%], respectively), and significantly higher cancer risk for Spigelman stage IV (25% [95% CI 12%–45%]). Of importance, the risk of duodenal and papillary cancers in Spigelman stage IV was similar (16% [95% CI 7%–33%] and 12 [95% CI 5%–24%], respectively) (7,28,29). The risk of duodenal cancer increased in each successive Spigelman stage (3% for stage II [95% CI 1%–10%], 2% for stage III [95% CI 1%–5%], and 16% for stage IV [95% CI 7%–33%]). The risk of papillary cancer followed a similar risk pattern (4% [95% CI 2%–10%], 4% [95% CI 2%–10%], 12% [95% CI 5%–24%], respectively) (24,30–32).
Sensitivity of the Spigelman stages for duodenal and papillary cancersWe assessed the sensitivity of the Spigelman stage IV for duodenal cancer from 9 studies (Figure 3) (21–24,27,30,32–34). Of interest, although the lifetime risk of duodenal cancer was higher for patients with a baseline Spigelman stage IV (21,27), duodenal and papillary cancers frequently occurred in individuals with Spigelman stage III or lower (21,23,31). We estimated a pooled sensitivity of 51% (95% CI 42%–60%) for duodenal and papillary cancers but reaching as low as 39% (95% CI 16%–68%) for papillary cancer (24,27,33). For papillary and duodenal cancers, the Spigelman stage at cancer diagnosis ranged from II to IV, indicating a comparable likelihood of Spigelman stage IV between cases and controls (27,31). A single study reported that Spigelman stages III/IV did not predict the risk of a composite end point of papillary neoplastic progression (defined as adenocarcinoma or high-grade dysplasia, HGD) (hazard ratio 1.6; 95% CI 0.49–5.5) (23,32).
 Figure 3.:
Figure 3.: Pooled sensitivity of Spigelman stage IV for (a) duodenal cancer, (b) papillary cancer, and (c) papillary and duodenal cancers. CI, confidence interval.
As a consequence of the suboptimal sensitivity for cancer, patients undergoing prophylactic duodenal surgery often had duodenal cancer that was unforeseen and unexpected during surgery (31,33,35–37).
Risk factors of duodenal and papillary cancersWe investigated these low sensitivity values and explored potential avenues for improvement. Nine studies assessed the cancer risk associated with individual risk factors, including specific components of the Spigelman system (7,23–25,27,28,30,31,38) (Figure 4).
 Figure 4.:
Figure 4.: Pooled measures of risk for the development of duodenal and papillary cancers. On the left side, the diverging bar charts represent the pooled prevalence of endoscopic and pathologic risk factors among cases and controls for (a) duodenal and papillary, (b) papillary, and (c) duodenal cancers. On the right side, forest plots represent the pooled relative risks (diamonds) and pooled odds ratios (squares) of endoscopic and pathologic risk factors for the development of (d) papillary and duodenal, (e) papillary, and (f) duodenal cancers. Odds ratios are always presented below relative risks. Relative risk and odds ratios are presented on a logarithmic scale extending from 0.1 to 15 to improve readability. CI, confidence interval; HGD, high-grade dysplasia; OR, odds ratio; RR, relative risk; TV/V, tubulovillous/villous histology. *These data were generated from the following studies (alphabetical order): Burke et al (1999); Groves et al (2002); Labib et al (2019); Latchford et al (2009); Moussata et al (2014); Noda et al (1992); Singh et al (2022); Takeuchi et al (2023); and Thiruvengadam et al (2019).
Duodenal polyps larger than 10 mm were associated with an increased risk of duodenal cancer (pooled relative risk [RR] 1.9, 95% CI 1.4–2.6). Almost all duodenal cancers occurred in patients with a history of at least 1 duodenal polyp larger than 10 mm, suggesting a high sensitivity (91.5%) (27,31). Furthermore, patients with FAP with duodenal/papillary cancer were more likely to have duodenal polyps larger than 10 mm compared with patients with FAP without cancer (76.5% vs 47.1%, P = 0.027) (27). When considering duodenal cancer separately, cases were still more likely to have duodenal polyps larger than 10 mm (pooled odds ratio 9, 95% CI 1.1–75.1) (27). However, there was no significant difference for papillary cancer (62.5% [95% CI 28.5%–87.5%] vs 47.1% [95% CI 36.7%–57.6%]). In one study, patients with duodenal polyps larger than 10 mm underwent endoscopic resection, while those with polyps smaller than 10 mm were placed under surveillance (39). During a median 8.5-year follow-up, no patients under surveillance required duodenal treatment, resulting in a 96% survival rate with only 1 death from rectal cancer (39). These findings support the hypothesis that polyps larger than 10 mm are a sensitive indicator of duodenal cancer risk.
The presence of more than 20 duodenal polyps has been associated with an increased risk of duodenal and papillary cancers. However, individuals with fewer than 20 polyps can still develop these cancers (21,25,27,31,32,37,39–42). In fact, FAP carriers with more than 20 duodenal polyps were at no higher risk of duodenal cancer, papillary cancer, or either adenocarcinoma (pooled RR 0.9 [95% CI 0.6–1.5], RR 0.2 [95% CI 0.0–1.1], and RR 0.6 [95% CI 0.3–1.0], respectively).
Limited data exist regarding HGD and villous/tubulovillous histology. We observed a significant association between HGD in duodenal polyps and duodenal cancer (RR 7.6, 95% CI 2.5–23.2) but not papillary cancer (RR 2.1, 95% CI 0.3–16.0). No significant difference in tubulovillous or villous histology was observed between cases and controls (RR 1.1, 95% CI 0.6–1.9), including when examining cases with duodenal (RR 1.5, 95% CI 0.9–2.6) and papillary cancer separately (RR 0.6, 95% CI 0.2–2.0). HGD in the papilla was also found to be a risk factor of papillary cancer (RR 7.1, 95% CI 1.4–36.4) but not for duodenal cancer (RR 2.8, 95% CI 0.5–17.4).
Three studies have shown that almost all papillary cancers arise from papillae larger than 10 mm, indicating a pooled sensitivity of 82.5% (95% CI 63.1%–92.7%) and an RR of 3.5 (95% CI 1.4–8.5) (25,31,40). One study even suggested that papilla size is the most predictive risk factor of cancer (25).
Age is a well-established risk factor of developing duodenal cancer and duodenal HGD. The overall lifetime risk of duodenal cancer is estimated to be 18% (95% CI 8%–28%) (21), with an average age at diagnosis of 53 years (31). The cumulative incidence of duodenal cancer increases with age, ranging from 3.2% at 40 years to 34.0% at 75 years (37). The 10-year rates of progression to low-grade dysplasia, HGD, and cancer are 75.8%, 20.8%, and 5.4%, respectively (32). Specific statistics for papillary cancer are currently lacking.
There is inconclusive evidence regarding other potential risk factors such as sex, APC mutation site/type, colonic surgery, number of colorectal polyps, desmoids, fundic gland polyposis, and pregnancy (27,31,43). Studies on family history of duodenal and colorectal cancer have reported conflicting evidence (27,31).
DISCUSSIONThe Spigelman staging system is widely used and easily applicable due to its simplicity and familiarity among clinicians. It provides a practical and computationally straightforward method for assessing the progression and regression of duodenal polyposis and estimating the future risk of duodenal cancer. However, our systematic review highlights that the current reliance on Spigelman stage IV as the primary criterion for cancer prevention strategies may overlook a significant proportion of duodenal and papillary cancers.
Although the risk of developing duodenal cancer is higher in stage IV, it is important to note that cancers can develop across various Spigelman stages (22–24,27,31,32,34,44). Relying solely on stage IV may underestimate cancer risk in almost half of all patients (21,23,31,32). Ideally, a staging system should inform clinicians of a high risk of duodenal cancer before it manifests. However, patients who undergo prophylactic duodenal surgery may still be diagnosed with duodenal cancer at histological review, indicating the presence of undetected carcinomas during surgery (31,33,35–37). Furthermore, the individual components of the Spigelman score may not uniformly predict the risk of duodenal cancer despite all being similarly scaled from 0 to 3 (26,27). Evidence suggests that factors such as villous histology and the number of duodenal polyps may not be strong predictors of duodenal cancer (26,27). Similarly, the components of the Spigelman score may not effectively predict the risk of papillary adenocarcinoma (23,31,44,45). Therefore, the sensitivity of the Spigelman staging system may be enhanced by assigning greater weights to the variables that offer better sensitivity to cancer, rating only these as 0 to 3, while the less predictive variables may be attenuated, ranging from 0 to 2 or 1.
Endoscopic downstaging seems to be an intuitive and appealing solution to mitigate the duodenal cancer risk observed in Spigelman stage IV and has been evaluated in 5 studies (7,26,28,29,46). In one downstaging program, the mean Spigelman score decreased to 6 ± 2.2 after 9 ± 4.5 years (28). In a recent prospective single-arm study, the authors achieved downstaging in 67.2% of patients within 1 year (7). However, almost all studies identified a significant risk of rapid upstaging after a patient is downstaged (46). In one study, 33% of patients downstaged to stage I progressed back to stage IV within 5 years, with a progression rate of 0.4 per year (29). Similarly, 42% of patients downstaged to stage II and 50% of those downstaged to stage III progressed back to stage IV within 3 years and 1 year, respectively (progression rates: 0.42 and 0.5 per year, respectively) (29). These progression rates are considerably faster than expected based on the natural history of FAP (37). Another study reported that patients downstaged from stage IV to II remained stable during a median follow-up of 37 months, but nearly 50% of those downstaged to stage III progressed back to stage IV (26).
Some additional limitations require careful scrutiny. The fact that duodenal and papillary cancers can develop even in stages III or II suggests that the association between stage IV and cancer is not strictly causal (Figure 2). Therefore, additional factors beyond the Spigelman score need to be considered in the management and risk assessment of patients with FAP after downstaging (26,28,29,46). These findings align with National Comprehensive Cancer Network guidelines that emphasize close surveillance for Spigelman stage–downgraded individuals, guided by prior stage, family history, and clinical judgment (3).
The association between the number of duodenal polyps and the risk of duodenal and papillary cancers remains a topic of debate. Studies indicated that individuals with a few duodenal polyps can still develop these types of cancers (21,25,27,31,32,37,39–42), which may explain the relatively low sensitivity of Spigelman stage IV for cancer. Conversely, the number of duodenal polyps is a straightforward parameter to monitor, and it intuitively correlates with the perceived risk of cancer. This is evidenced by including duodenal burden (i.e., the sum of the diameters of all duodenal polyps) as a primary end point in various randomized clinical trials on chemoprevention (41,42). Hence, the ease of computation, the integration in clinical trials, and the presumed association with duodenal cancer collectively suggest that the number of duodenal polyps should remain part of an updated duodenal classification system. Nevertheless, it is important to recognize that the development of cancer in individuals with a low number of polyps likely contributes to the low sensitivity values. It is also worth noting that chromoendoscopy techniques (both digital and indigo) have demonstrated the potential to increase the polyp count (47,48). Whether this increase in polyp count accurately reflects a higher risk of duodenal cancer has yet to be fully elucidated.
Accurate visualization of the papilla is crucial for assessing the risk of papillary cancer, whether with cap-assisted or with side-viewing endoscopy (49,50). One study reported a higher risk of papillary cancer among patients who had incomplete visualization of the papilla (27), and compelling evidence indicated that papillary cancer predominantly arises from papillae larger than 10 mm (RR 3.5, 95% CI 1.4–8.5) (25,31,40) (Figure 4). While routine papillary biopsies are generally not recommended, given the risk of iatrogenic pancreatitis, a low threshold for performing papillary biopsies should be maintained in cases where the papilla diameter exceeds 10 mm or when there are optical suspicions of an ampulloma.
While our systematic review offers valuable insights into optimizing the Spigelman staging system, it is important to acknowledge its limitations. Measuring the risk of individual items was faced with statistical challenges due to limited sample sizes and the common practice of combining papillary and duodenal cancers, particularly regarding the histology of the papilla, duodenal polyps, and the grade of dysplasia. One statistical challenge was posed by the largest and most comprehensive case-control study involving 103 patients with FAP observed for more than 25 years, which was weighted the heaviest, and therefore could have biased the results of duodenal histological variables, restricting the ability to measure the risk of individual items with certainty (27). Therefore, it is necessary to validate them in larger studies before any refinement of the Spigelman system.
In conclusion, our systematic review has shed light on the limitations of the Spigelman staging system while uncovering crucial risk factors associated with duodenal and papillary cancers, thereby providing a framework for improving its performance (Figure 2). We have identified key variables, including the number and size of duodenal polyps, duodenal polyps and papillary HGD, papilla size exceeding 10 mm, and the age of the patient, all of which have demonstrated significant associations with duodenal cancer risk. In addition, although the evidence is somewhat less robust, factors such as papillary HGD and papilla size exceeding 10 mm have been implicated in the heightened risk of papillary cancer (Figure 4). Incorporating these findings into an optimized staging system would ensure its ability to accurately capture the dynamic nature of the disease while upholding the user-friendly nature and capacity for long-term tracking inherent in its predecessor. These advances hold great promise for enhancing clinical decision-making and improving FAP patient outcomes in managing duodenal and papillary cancers.
CONFLICTS OF INTERESTGuarantor of the article: The first author and all coauthors had full access to the data and had control of the decision to publish.
Specific author contributions: A.M., G.M., and G.M.C.: conception. A.M., G.M., and G.M.C.: design. A.M. and G.M.C.: acquisition of data. A.M. and G.M.C.: analysis of data. A.M., M.P., A.G., G.M., M.S.D.S., and G.M.C.: interpretation of data. A.M. and G.M.: work drafting. A.M., M.P., A.G., G.M., M.S.D.S., and G.M.C.: work review for critical intellectual content. All authors approved the final draft submitted.
Financial support: A.M. reports that part of this project was supported by Fight Colorectal Cancer and the Collaborative Group of the Americas on Inherited Gastrointestinal Cancer. All other authors report no funding sources, institutions, or otherwise referred sponsors to disclose.
Potential competing interests: None to report.
REFERENCES 1. Karstensen JG, Bülow S, Højen H, et al. Cancer in patients with familial adenomatous polyposis: A nationwide Danish cohort study with matched controls. Gastroenterology 2023;165(3):573–81.e3. 2. Spigelman AD, Talbot IC, Williams CB, et al. Upper gastrointestinal cancer in patients with familial adenomatous polyposis. Lancet 1989;2(8666):783–5. 3. Gupta S, Weiss JM, Axell L, et al. Genetic/Familial High-Risk Assessment: Colorectal. NCCN Guidelines Version 2.2023. NCCN: Plymouth Meeting, PA, 2023. 4. Monahan KJ, Bradshaw N, Dolwani S, et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut 2020;69(3):411–44. 5. van Leerdam ME, Roos VH, van Hooft JE, et al. Endoscopic management of polyposis syndromes: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy 2019;51(9):877–95. 6. Yang J, Gurudu SR, Koptiuch C, et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in familial adenomatous polyposis syndromes. Gastrointest Endosc 2020;91(5):963–82.e2. 7. Takeuchi Y, Hamada K, Nakahira H, et al. Efficacy and safety of intensive downstaging polypectomy (IDP) for multiple duodenal adenomas in patients with familial adenomatous polyposis: A prospective cohort study. Endoscopy 2023;55(6):515–23. 8. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 2010;25(9):603–5. 9. Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. JNCI J Natl Cancer Inst 1959;22(4):719–48. 10. Robins J, Greenland S, Breslow NE. A general estimator for the variance of the Mantel-Haenszel odds ratio. Am J Epidemiol 1986;124(5):719–23. 11. Higgins J, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. 2nd edn. John Wiley Sons: Hoboken, NJ, 2019. 12. Efthimiou O. Practical guide to the meta-analysis of rare events. Evid Based Ment Health 2018;21(2):72–6. 13. Viechtbauer W Bias and efficiency of meta-analytic variance estimators in the random-effects model. J Educ Behav Stat 2005;30(3):261–93. 14. Paule RC, Mandel J. Consensus values and weighting factors. J Res Natl Bur Stand (1977) 1982;87(5):377–85. 15. Hartung J, Knapp G. On tests of the overall treatment effect in meta-analysis with normally distributed responses. Stat Med 2001;20(12):1771–82. 16. Harrer M, Cuijpers P, Furukawa TA, et al. Doing Meta-Analysis with R: A Hands-On Guide. London Chapman Hall/CRC Press: Boca Raton, FL, 2021. 17. Noma H. dmetatools: Computational tools for meta-analysis of diagnostic accuracy test. 2023. 18. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw 2010;36(3):1–48. 19. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: A practical tutorial. Evid Based Ment Health 2019;22(4):153–60. 20. Lumley T. rmeta: Meta-Analysis. R package version 3.0. 2018. 21. Bülow S, Christensen IJ, Højen H, et al. Duodenal surveillance improves the prognosis after duodenal cancer in familial adenomatous polyposis. Colorectal Dis 2012;14(8):947–52. 22. Bülow S, Björk J, Christensen IJ, et al. Duodenal adenomatosis in familial adenomatous polyposis. Gut 2004;53(3):381–6. 23. Singh AD, Bhatt A, Joseph A, et al. Natural history of ampullary adenomas in familial adenomatous polyposis: A long-term follow-up study. Gastrointest Endosc 2022;95(3):455–67.e3. 24. Groves CJ, Saunders BP, Spigelman AD, et al. Duodenal cancer in patients with familial adenomatous polyposis (FAP): Results of a 10 year prospective study. Gut 2002;50(5):636–41. 25. Labib PL, Goodchild G, Turbett JP, et al. Endoscopic ultrasound in the assessment of advanced duodenal adenomatosis in familial adenomatous polyposis. BMJ Open Gastroenterol 2019;6(1):e000336. 26. Roos VH, Bastiaansen BA, Kallenberg FGJ, et al. Endoscopic management of duodenal adenomas in patients with familial adenomatous polyposis. Gastrointest Endosc 2021;93(2):457–66. 27. Thiruvengadam SS, Lopez R, O'Malley M, et al. Spigelman stage IV duodenal polyposis does not precede most duodenal cancer cases in patients with familial adenomatous polyposis. Gastrointest Endosc 2019;89(2):345–54.e2. 28. Moussata D, Napoleon B, Lepilliez V, et al. Endoscopic treatment of severe duodenal polyposis as an alternative to surgery for patients with familial adenomatous polyposis. Gastrointest Endosc 2014;80(5):817–25. 29. Balmforth DC, Phillips RKS, Clark SK. Advanced duodenal disease in familial adenomatous polyposis: How frequently should patients be followed up after successful therapy? Fam Cancer 2012;11(4):553–7. 30. Burke CA, Beck GJ, Church JM, et al. The natural history of untreated duodenal and ampullary adenomas in patients with familial adenomatous polyposis followed in an endoscopic surveillance program. Gastrointest Endosc 1999;49(3 Pt 1):358–64. 31. Latchford AR, Neale KF, Spigelman AD, et al. Features of duodenal cancer in patients with familial adenomatous polyposis. Clin Gastroenterol Hepatol 2009;7(6):659–63. 32. Sourrouille I, Lefèvre JH, Shields C, et al. Surveillance of duodenal polyposis in familial adenomatous polyposis: Should the Spigelman score be modified? Dis Colon Rectum 2017;60(11):1137–46. 33. Augustin T, Moslim MA, Tang A, et al. Tailored surgical treatment of duodenal polyposis in familial adenomatous polyposis syndrome. Surgery 2018;163(3):594–9. 34. Björk J, Åkerbrant H, Iselius L, et al. Periampullary adenomas and adenocarcinomas in familial adenomatous polyposis: Cumulative risks and APC gene Mutations. Gastroenterology 2001;121(5):1127–35. 35. Augustin T, Moslim MA, Cengiz TB, et al. Survival outcomes after surgical management of sporadic or familial adenomatous polyposis associated duodenal cancer. J Surg Oncol 2020;122(6):1132–44. 36. Watanabe Y, Ishida H, Baba H, et al. Pancreas-sparing total duodenectomy for Spigelman stage IV duodenal polyposis associated with familial adenomatous polyposis: Experience of 10 cases at a single institution. Fam Cancer 2017;16(1):91–8. 37. Lepistö A, Kiviluoto T, Halttunen J, et al. Surveillance and treatment of duodenal adenomatosis in familial adenomatous polyposis. Endoscopy 2009;41(6):504–9. 38. Noda Y, Watanabe H, Iida M, et al. Histologic follow-up of ampullary adenomas in patients with familial adenomatosis coli. Cancer 1992;70(7):1847–56. 39. Yachida T, Nakajima T, Nonaka S, et al. Characteristics and clinical outcomes of duodenal neoplasia in Japanese patients with familial adenomatous polyposis. J Clin Gastroenterol 2017;51(5):407–11. 40. Kashiwagi H, Spigelman AD, Debinski HS, et al. Surveillance of ampullary adenomas in familial adenomatous polyposis. Lancet 1994;344(8936):1582. 41. Samadder NJ, Foster N, McMurray RP, et al. Phase II trial of weekly erlotinib dosing to reduce duodenal polyp burden associated with familial adenomatous polyposis. Gut 2022;72(2):256–63. 42. Samadder NJ, Neklason DW, Boucher KM, et al. Effect of sulindac and erlotinib vs placebo: On duodenal neoplasia in familial adenomatous polyposis: A randomized clinical trial. JAMA 2016;315(12):1266–75. 43. Park SY, Ryu JK, Park JH, et al. Prevalence of gastric and duodenal polyps and risk factors for duodenal neoplasm in Korean patients with familial adenomatous polyposis. Gut Liver 2011;5(1):46–51. 44. Ma T, Jang EJ, Zukerberg LR, et al. Recurrences are common after endoscopic ampullectomy for adenoma in the familial adenomatous polyposis (FAP) syndrome. Surg Endosc 2014;28(8):2349–56. 45. Mathus-Vliegen EMH, Boparai KS, Dekker E, et al. Progression of duodenal adenomatosis in familial adenomatous polyposis: Due to ageing of subjects and advances in technology. Fam Cancer 2011;10(3):491–9. 46. Noh JH, Song EM, Ahn JY, et al. Prevalence and endoscopic treatment outcomes of upper gastrointestinal neoplasms in familial adenomatous polyposis. Surg Endosc 2022;36(2):1310–9. 47. Picasso M, Filiberti R, Blanchi S, et al. The role of chromoendoscopy in the surveillance of the duodenum of patients with familial adenomatous polyposis. Dig Dis Sci 2007;52(8):1906–9. 48. Hüneburg R, Heling D, Kaczmarek DJ, et al. Dye chromoendoscopy leads to a higher adenoma detection in the duodenum and stomach in patients with familial adenomatous polyposis. Endosc Int Open 2020;8(10):E1308–14. 49. Silva LC, Arruda RM, Botelho PFR, et al. Cap-assisted endoscopy increases ampulla of Vater visualization in high-risk patients. BMC Gastroenterol 2020;20(1):214. 50. Kallenberg FGJ, Bastiaansen BAJ, Dekker E. Cap-assisted forward-viewing endoscopy to visualize the ampulla of Vater and the duodenum in patients with familial adenomatous polyposis. Endoscopy 2017;49(2):181–5.
留言 (0)