
記住我
Individual patient-level data were obtained from the phase 3, global, randomized MAIA trial (ClinicalTrials.gov identifier NCT02252172) based on a median follow-up of 64.5 months, and from the phase 3, USA-based, randomized SWOG S0777 trial (ClinicalTrials.gov identifier NCT00644228) based on the primary data cut with a median follow-up of 55 months [3, 4]. Relative treatment effects across the two trials were compared using an anchored ITC design (Fig. S1 in the electronic supplementary material) with matched patient eligibility criteria (Fig. 1). Additional details are provided below in the “Statistical Methods” section.
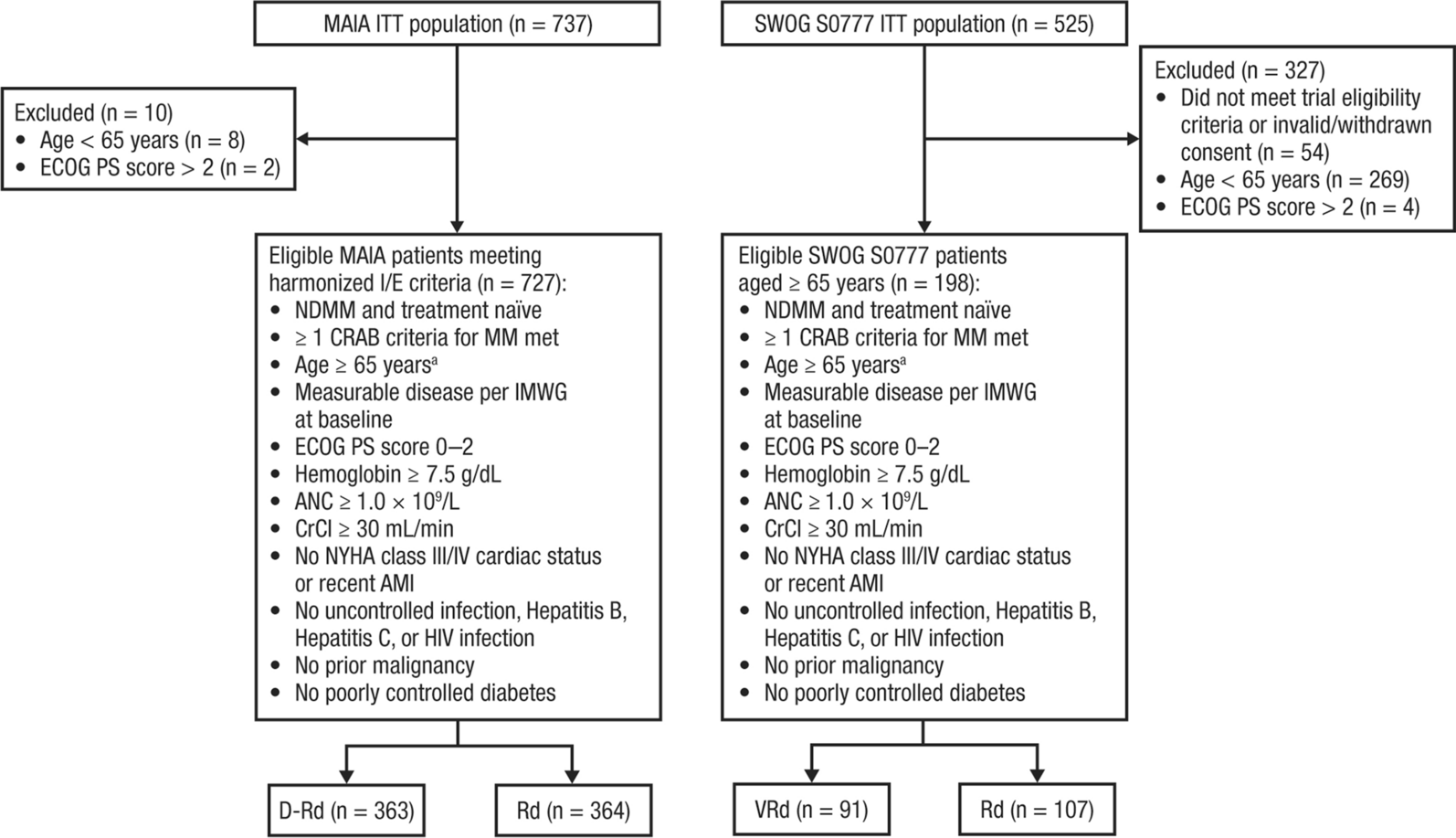
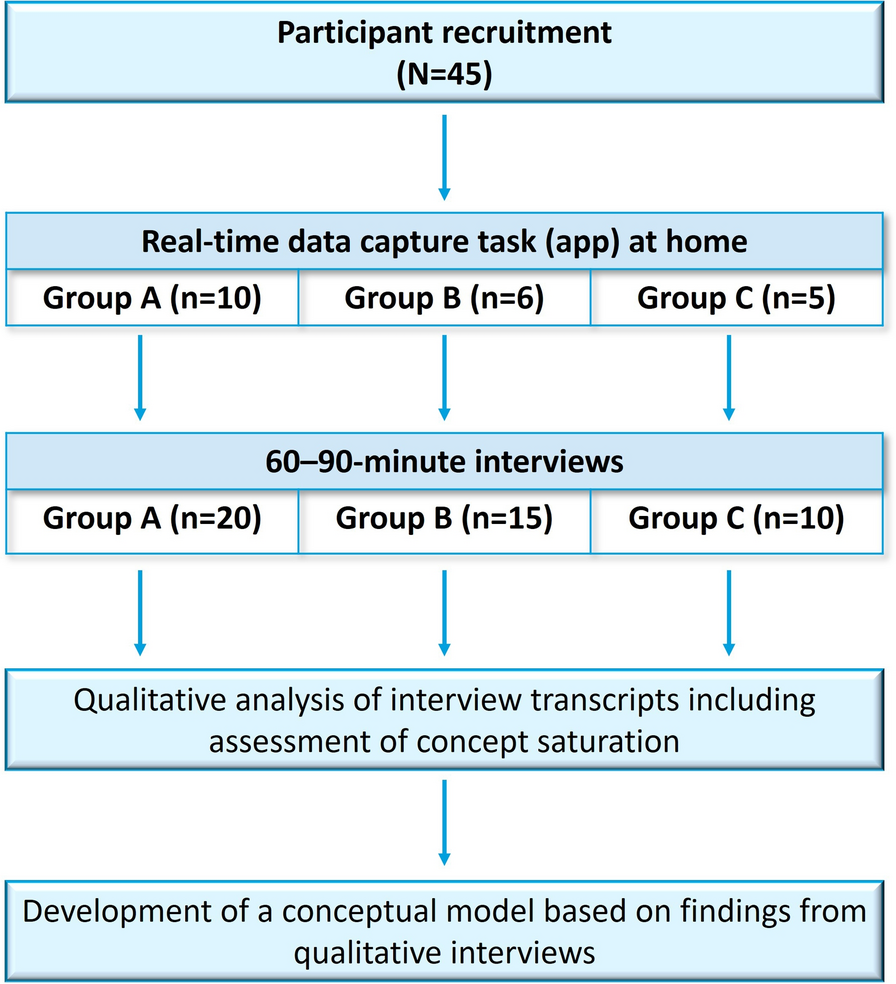
Fig. 1
Selection of eligible patients from the MAIA and SWOG S0777 trials with TIE NDMM. SWOG Southwest Oncology Group, TIE transplant ineligible, NDMM newly diagnosed multiple myeloma, ITT intent-to-treat, ECOG PS Eastern Cooperative Oncology Group performance status, I/E inclusion/exclusion, CRAB calcium elevation, renal impairment, anemia, bone involvement, MM multiple myeloma, IMWG International Myeloma Working Group, ANC absolute neutrophil count, CrCl creatinine clearance, NYHA New York Heart Association, AMI acute myocardial infarction, HIV human immunodeficiency virus, D-Rd daratumumab plus lenalidomide/dexamethasone, Rd lenalidomide/dexamethasone, VRd bortezomib plus lenalidomide/dexamethasone, Rd lenalidomide/dexamethasone. aAge ≥ 65 years used as a proxy for transplant ineligibility. In the MAIA trial, which enrolled patients considered ineligible for transplant because of age ≥ 65 years or comorbidities precluding transplant, 99% of patients were aged ≥ 65 years at enrollment. In the SWOG S0777 trial, which enrolled patients without intent for immediate transplant (including TIE and transplant-eligible patients), 202 of 471 (43%) patients eligible for analysis were aged ≥ 65 years at enrollment
MAIA TrialThe MAIA trial enrolled patients aged ≥ 18 years with NDMM who were ineligible for high-dose chemotherapy with autologous stem cell transplantation (ASCT) because of age (≥ 65 years) or the existence of adverse comorbidities, satisfied CRAB criteria (C = calcium elevation; R = renal impairment; A = anemia; B = bone involvement) for multiple myeloma, had measurable disease, and had an Eastern Cooperative Oncology Group (ECOG) performance status score of ≤ 2. Patients were enrolled from March 2015 through January 2017, across 176 sites in 14 countries globally [5]. Patients were randomized 1:1 to receive D-Rd or Rd [5]. Patients in both treatment groups received 28-day cycles of orally administered lenalidomide (25 mg on days 1–21 of each cycle) and orally administered dexamethasone (40 mg on days 1, 8, 15, and 22 of each cycle). Patients in the D-Rd group additionally received intravenously administered daratumumab (16 mg/kg, once weekly during cycles 1–2, once every 2 weeks in cycles 3–6, and once every 4 weeks thereafter). Treatment was given until disease progression or unacceptably toxicity [5].
SWOG S0777 TrialThe SWOG S0777 trial enrolled patients with NDMM who were ineligible or without intent to receive an ASCT as part of first-line therapy, satisfied CRAB criteria, had measurable disease, and had an ECOG performance status score of 0 to 3. Patients were enrolled from participating SWOG and National Clinical Trial Network (NCTN) institutions throughout the USA [4]. Patients were randomized 1:1 to receive VRd or Rd alone [4]. The Rd regimen was given as six 28-day cycles, in which patients received orally administered lenalidomide (25 mg on days 1–21 of each cycle) and orally administered dexamethasone (40 mg on days 1, 8, 15, and 22 of each cycle). The VRd regimen was given as eight 21-day cycles, in which patients received intravenously administered bortezomib (1.3 mg/m2 on days 1, 4, 8, and 11 of each cycle) combined with orally administered lenalidomide (25 mg on days 1–14 of each cycle) and dexamethasone (20 mg on days 1, 2, 4, 5, 8, 9, 11, and 12 of each cycle). Treatment was given until disease progression or unacceptable toxicity [4]. Individual patient-level data from the SWOG S0777 trial were obtained from the NCTN/National Cancer Institute Community Oncology Research Program (NCORP) Data Archive of the National Cancer Institute’s (NCI) NCTN.
Harmonized Inclusion/Exclusion CriteriaHarmonized key inclusion/exclusion criteria were applied to align the trial populations, allowing for treatment effects to be estimated in a similar target patient population. The harmonized inclusion criteria applied for the present study included NDMM, age ≥ 65 years (a proxy for transplant ineligibility), symptomatic disease (≥ 1 CRAB criteria satisfied), measurable disease per International Myeloma Working Group criteria, ECOG performance status score ≤ 2, hemoglobin ≥ 7.5 g/dL, absolute neutrophil count ≥ 1.0 × 109/L, and creatinine clearance ≥ 30 mL/min. Key exclusion criteria included New York Heart Association class III/IV cardiac status or recent acute myocardial infarction, uncontrolled infection, human immunodeficiency virus infection, hepatitis B or C infection, prior cancer, or poorly controlled diabetes (Fig. 1; Table S1 in the electronic supplementary material).
Because the SWOG S0777 trial included a mixed population of patients without intent for immediate ASCT, age ≥ 65 years was used as a proxy for transplant ineligibility [7]. For consistency, the age ≥ 65 years restriction was also applied to the MAIA trial population, 99% of whom were aged ≥ 65 years at enrollment.
Baseline Patient CharacteristicsAs explained in more detail below in the “Statistical Methods” section, key baseline patient characteristics were identified for cross-trial covariate adjustment based on their potential role as treatment-effect modifiers. These baseline patient characteristics included age, sex, International Staging System disease stage, ECOG performance status score, hemoglobin, estimated glomerular filtration rate, lactate dehydrogenase (LDH), and cytogenetic risk, with high risk defined as the presence of ≥ 1 high-risk cytogenetic abnormality (del17p, t[14;16], or t[4;14]).
OutcomesThe primary outcome was PFS, defined as the time from treatment randomization to disease progression or death, whichever occurred first. Progressive disease was determined in accordance with the International Myeloma Working Group criteria [8, 9]. In the primary analysis of PFS in the MAIA trial, patients were censored if subsequent therapy was initiated prior to disease progression; however, this was not done in the SWOG S0777 trial. To align the censoring rules for the present ITC, no censoring for subsequent therapy was done for PFS analyses in either the MAIA or SWOG S0777 trials.
Statistical MethodsThe present study used an adjusted anchored ITC design, a preferred approach for conducting a cross-trial comparison of treatment effectiveness when outcome data are available from two randomized controlled trials in which two different treatments were each compared against the same comparator or “anchor” (Fig. S1). In an anchored ITC, the magnitudes of relative treatment effects versus the common comparator are contrasted to make indirect inference about the relative effectiveness of the two treatment regimens not directly compared in a head-to-head trial [10, 11].
A critical assumption for an anchored ITC is that the two trials being compared need to have enrolled patients who are similar with respect to possible treatment effect modifiers, such as patient age, fitness, or cytogenetic risk [12]. The availability of individual patient-level data from both trials allows for adjustment for cross-trial differences in trial inclusion/exclusion criteria and patient baseline characteristics. As a result of differences in patient populations between the MAIA and SWOG S0777 trials, a harmonized set of inclusion/exclusion eligibility criteria were applied to ensure the balance of potential treatment effect modifiers across both data sources (Fig. 1; Table S1). Propensity-score weighting was then used to balance the two trial populations on key baseline characteristics [13, 14]. Baseline covariate balance after propensity-score weighting was assessed using standardized differences, with an absolute standardized difference > 0.1 considered a meaningful imbalance [15].
For ITCs, Rd was used as the common anchor across the MAIA and SWOG S0777 trials. To determine differences in PFS, Cox proportional hazards regression was used to calculate HRs between treatments relative to the common Rd anchor within each trial (MAIA, D-Rd vs Rd; SWOG S0777, VRd vs Rd). Using these calculated direct HRs, an ITC was then used to indirectly estimate the HR between trials (D-Rd vs VRd). Robust standard errors were used in the Cox regression models to account for the use of propensity-score weighting. Inspection of Kaplan–Meier survival plots and the statistical interactions between treatment and follow-up time were used to evaluate the Cox regression model’s proportional hazard assumption.
Missing baseline covariate data were addressed with multiple imputation. Multiple imputation by chained equations was used to assign missing baseline covariate values and was repeated to create ten complete datasets [16, 17]. Following multiple imputation, each complete dataset was analyzed separately, and the resulting parameter estimates and standard errors were pooled to obtain a summarized parameter estimate and standard error [18].
All statistical analyses were performed using Statistical Analysis System (SAS) version 9.4 (SAS Institute, Cary, NC).
Sensitivity and Subgroup AnalysesThree sensitivity analyses analyzing PFS were performed. The first was an unweighted analysis in which harmonized inclusion/exclusion criteria were applied to both trial populations without propensity-score weighting. The second was a doubly robust analysis in which both propensity-score weighting and Cox outcome regression model adjustment for baseline covariates were used. The third was an analysis restricted to only patients with hemoglobin ≥ 9 g/dL. In terms of inclusion criteria, the MAIA trial required a baseline hemoglobin of ≥ 7.5 g/dL and the SWOG S0777 trial required a hemoglobin of ≥ 9 g/dL; however, both trials included patients with hemoglobin < 9 g/dL (14% and 8% of MAIA and SWOG S0777 patients, respectively, aged ≥ 65 years). In contrast, in the primary analysis of PFS, propensity-score weighting was used to adjust for baseline hemoglobin, but no restriction based on hemoglobin was applied (Table S1). Additionally, a subgroup analysis was performed in patients with high cytogenetic risk.
Research Ethics StatementsThe MAIA and SWOG S0777 trials were conducted in accordance with the principles of the Declaration of Helsinki, with study protocols approved by independent ethics committees and/or institutional review boards at each site. All patients provided written informed consent.
留言 (0)