
記住我


A systematic literature review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [28]. The following research question was addressed in the systematic literature review: What is the persistence/non-persistence and adherence/non-adherence among adults with diabetes using basal insulin in Western Europe? The two electronic databases MEDLINE (via the PubMed platform) and Embase were searched in June 2022. The details of the search strings applied in this systematic literature review are presented in Table 1. In addition to the systematic search, EASD and ISPOR were manually searched for relevant peer-reviewed conference abstracts. These conferences are some of the leading societies for health economics and outcome research as well as diabetes research, and they are known to publish relevant abstracts on adherence or persistence in diabetes care.
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Eligibility CriteriaThe PICO (population, intervention, comparator and outcomes) reporting system was used to define a relevant review question and to help formulate the search strategy. The eligibility criteria are presented in Table 2. The systematic literature review included studies in which there was a population of adults from Western Europe (including the UK, France, Spain, Switzerland, Netherlands, Ireland, Austria, Portugal, Denmark, Norway, Sweden, Finland, Italy, Germany, Iceland and Belgium) with diabetes treated with basal insulin. In addition, studies had to present original data and analyses. The predefined outcomes of interest were all findings related to adherence/non-adherence or persistence/non-persistence to basal insulin treatment reported as proportions of patients. Treatment persistence is defined as continuing to take medication throughout the prescribed period, and treatment adherence is defined as complying with the prescribed medicine in terms of drug schedules and dosages [21]. The included studies were English-language studies published between 2012 and 2022.
Table 2 Inclusion and exclusion criteriaStudy Selection and Data CollectionAll studies were reviewed in a blinded two-step process by two independent reviewers. The first step was screening of title and abstract. In the second step, eligible studies were screened at full-text level. The studies were included in accordance with the predefined eligibility criteria and any case of disagreement about the eligibility of a study was resolved through discussion between the two reviewers or by referral to the project manager. Each study could only be included once, meaning that a publication would be excluded if it presented a study already included through another publication. However, background information such as study characteristics could be combined from both publications if complete information was not available in one of the publications. Silvi was used to ensure a structured review process [29].
Any measures of adherence/non-adherence and persistence/non-persistence available from the literature were considered relevant regardless of the follow-up period or methodology. Adherence/non-adherence was often measured by medication possession ratio (MPR) which is calculated as the proportion (or percentage) of days covered by the medication dispensed during a specified time period or over a period of refill intervals (using a threshold of 80%). Other measures of adherence/non-adherence included missed doses, mistimed doses and reduced doses. Persistence/non-persistence was measured as uninterrupted treatment administration.
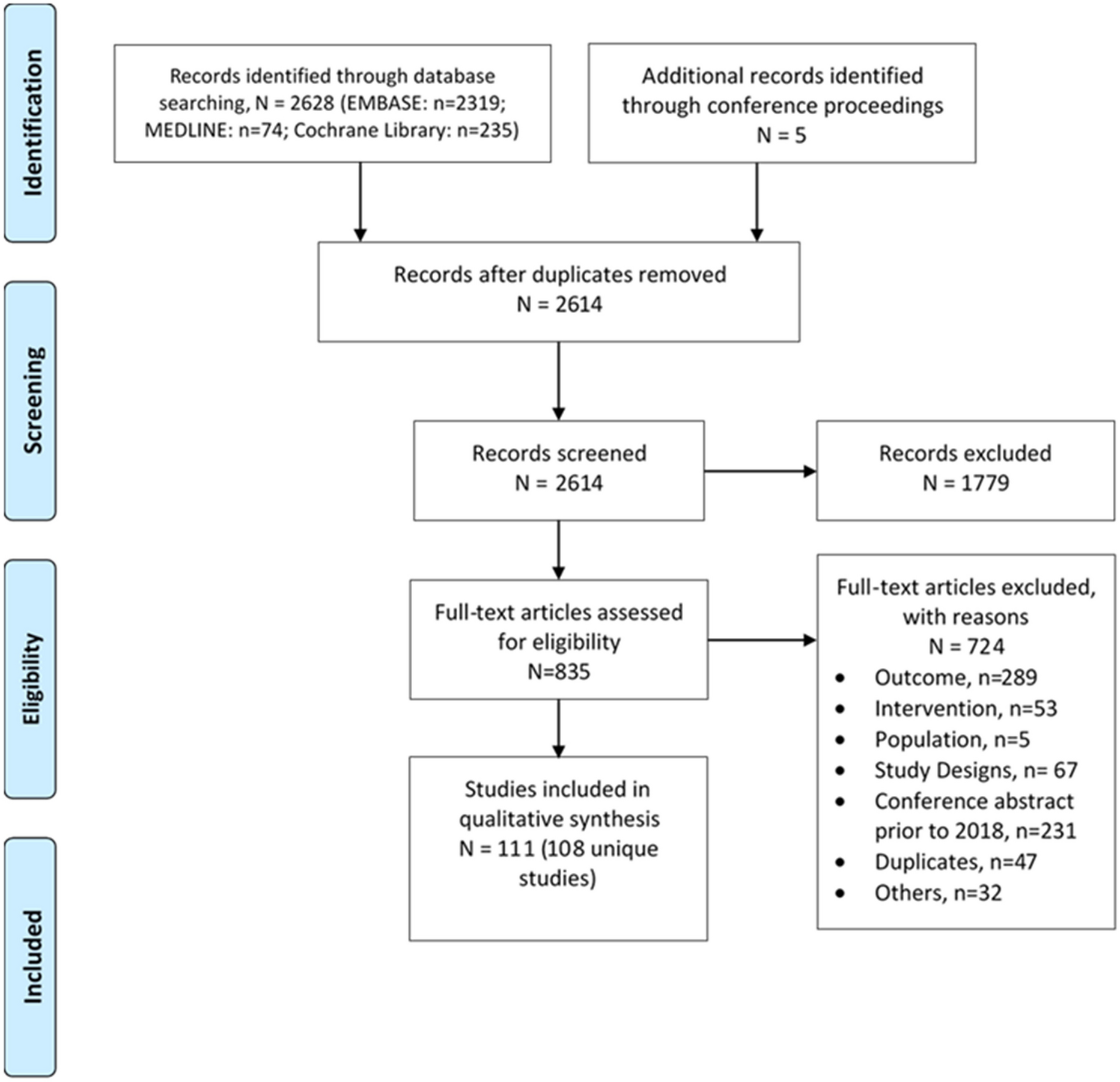
Identified StudiesThe systematic literature search of Medline and Embase resulted in 11 eligible studies. Additionally, we identified two relevant poster abstracts from EASD and ISPOR, yielding a total of 13 eligible studies [9, 15, 16, 25, 30,31,32,33,34,35,36,37,38]. The flow of studies through the two-step study selection process is presented in a flowchart in Fig. 1. This manuscript presents results from the studies regarding insulin adherence/non-adherence and persistence/non-persistence among people with T2D. By further excluding studies that do not present any subgroup results stratified by T2D, this manuscript includes 12 eligible studies. From the 12 studies, a total of 30 relevant subgroup results were identified. It should be noted that one subgroup could present results on multiple outcome measures.
Fig. 1
Flowchart. †Although the studies were excluded, they contributed with background information about the subpopulations
Of the 12 studies included in this manuscript, four presented results on adherence/non-adherence [15, 30, 32, 37] and nine presented results on persistence/non-persistence [9, 16, 25, 31, 33,34,35,36,37], one of which presented results on both adherence/non-adherence and persistence/non-persistence [37]. This last-mentioned study included people treated with all kinds of insulin, which is why it was not possible to extract results for basal insulin only. Therefore, the insulin type in the study will be categorised as basal-bolus insulin throughout this manuscript.
Data Extraction and Statistical AnalysesA comprehensive data extraction was conducted from all eligible studies following the PRISMA checklist [28] and using a pre-specified data extraction form in Microsoft Excel. Separate data points were extracted for each population and subpopulation with individual findings, i.e. subgroups by country, insulin type or background therapy. Data extraction included information on study characteristics, i.e. author, year of publication and information about the study population (size, country, mean age, background therapy, diabetes status, insulin status and diabetes-associated complications), methodology, i.e. data source and follow-up time, and findings from all outcomes deemed relevant for the research question.
When appropriate, a proportional meta-analysis calculating pooled rates was performed to assess insulin adherence/non-adherence and persistence/non-persistence among people with T2D in Western Europe. As recommended in the literature, the pooled rates were based on a random-effects model and Freeman–Tukey transformation using the software JBI SUMARI [39, 40]. Heterogeneity between the included studies was assessed through tau squared, chi squared and I2 statistics. As a result of high variance in the outcome definitions applied in the included studies, comparative narrative analyses were performed, when proportional meta-analysis was inappropriate. In studies not reporting non-persistence or non-adherence rates, these were calculated as 1 minus the reported persistence or adherence rate.
To investigate the identified data further, a number of sensitivity analyses were conducted, including an analysis of persistence rates when results on NPH were excluded, and analyses of both persistence and adherence findings when data not differentiating between basal and bolus insulin were excluded.
留言 (0)