
Remember me
This review found that lottery incentives have variable effects on target behaviours depending on several factors, such as the context in which the incentive was being offered, the target population, and the incentivised behaviour. To provide greater insight into the findings, this section has been divided into three main categories: the effects of lottery incentives on HIV testing-, HIV prevention-, and HIV treatment services.
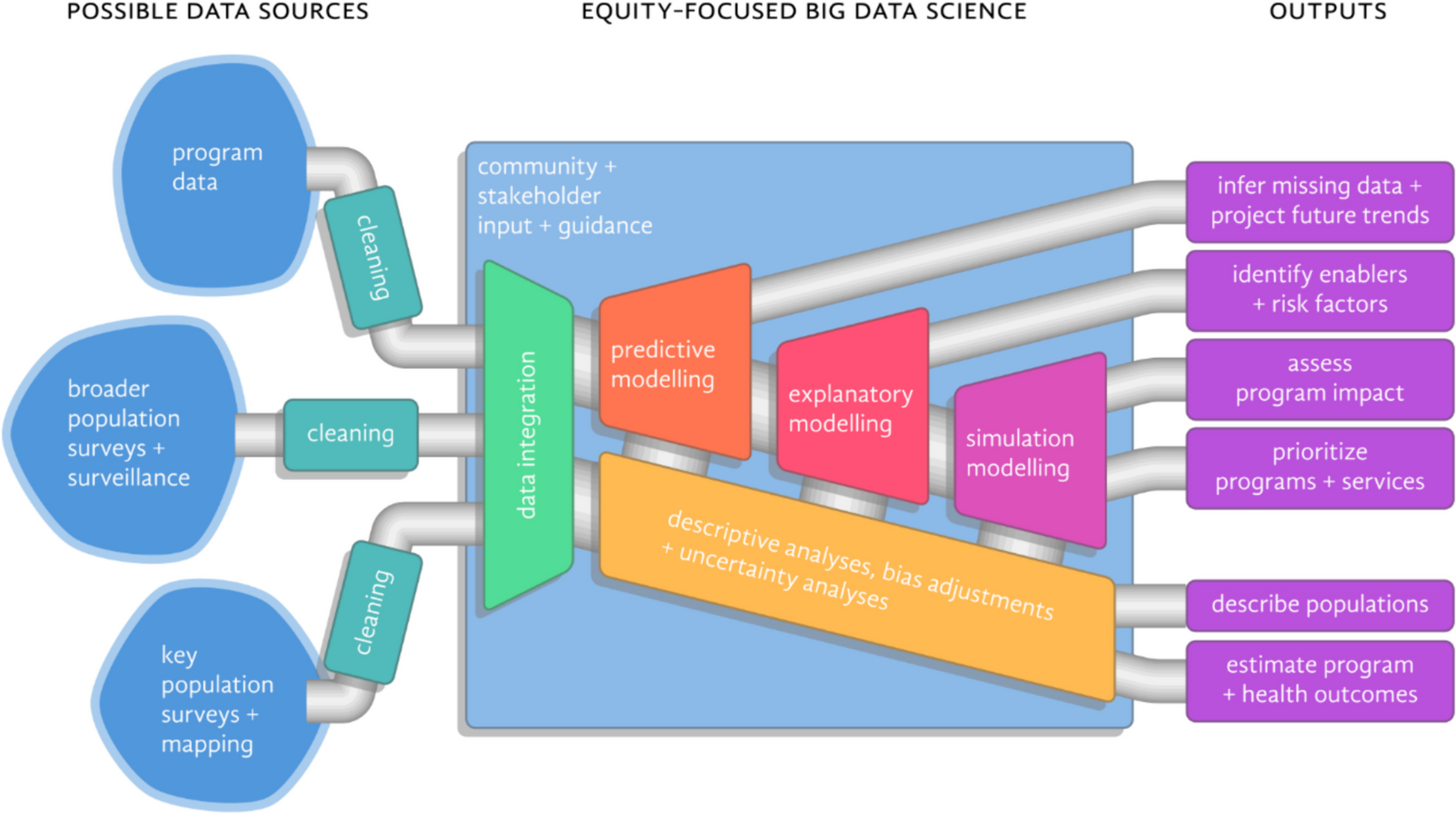
The Effects of Lottery Based Incentives on HIV Testing ServicesHIV testing is the first critical step to achieving the UNAIDS 95–95-95 targets. Incentivising HIV testing addresses the first 95 target and may support improved linkage to HIV prevention and treatment services. As seen in Fig. 2, four articles were reviewed that explored lottery incentives as an intervention to improve the uptake of HIV testing [5, 6, 9, 10].
Fig. 2
HIV-related services and the potential areas of impact for lottery incentives
A randomised control trial (RCT) in urban Malawi assessed the effect of financial incentives on the secondary distribution of HIV self-test (HIVST) kits to men through their pregnant partners attending antenatal care (ANC) [6]. A sample size of 2349 pregnant women and their partners were randomised into one of the following arms: the standard of care (an invitation to male partners for clinic-based HIV testing), HIVST alone, and HIVST coupled with three financial incentive conditions: $3 or $10 fixed incentive or an entry to a $30 lottery [6]. Women who attended ANC for the first time were given the relevant referral/HIVST to give to their partners who then needed to return to the clinic for post-test counselling services within 28 days [6]. The lottery arm was dropped at interim analysis because no difference was observed between HIVST with lottery and HIVST alone [6]. However, the HIVST coupled with fixed incentives increased the uptake of post-test counselling services among the male partners, with the $10 incentives having a greater effect [6]. Various factors may affect how incentives are perceived by their intended beneficiaries. Formative qualitative work conducted before the RCT, highlighted important factors that may have mediated the acceptability of incentives in this intervention [5]. Feedback regarding lottery incentives was largely negative; they were regarded as unfair, and there was concern that participants who did not win would dissuade others from attending the clinic [5]. Fixed incentives, however, were perceived to compensate for the costs of clinic attendance [5]. Taken together with the results from the RCT, these data suggest that fixed incentives are preferable to lottery incentives in low economic settings as they better address the financial barriers to service uptake.
A study comprising 2050 households in Harare, Zimbabwe, examined the use of financial incentives to improve the uptake of clinic-based HIV testing for children and adolescents [8–17 years old] [9]. This study evaluated the effect of no incentives, fixed incentives ($2), and lottery incentives ($5 or $10) on uptake of referral for HIV testing. The rates of HIV testing significantly increased with both fixed incentives (48%) and lottery incentives (40%) as compared to the control group (20%); however, there was no statistical difference between the two incentivised groups [9]. In this study, both fixed and lottery incentives were sufficient to encourage caregivers to take their children to the clinic for HIV testing. [9] These interventions may be bolstered by incentivising both the children and the caregivers. Incentivising caregivers only could raise ethical concerns, such as the possibility of caregivers pressuring their children to participate. [9] Lottery incentives, however, may serve as a means of overcoming this concern, as they are not guaranteed. [9].
A qualitative study, in rural Uganda, examined men's perceptions of using lottery incentives to improve the uptake of community-based HIV testing. [10] Sixty in-depth interviews were conducted with purposefully sampled men (age, incentive group and campaigns attended). Similar to findings of the other qualitative study reported above [5], participants noted that incentives may offset associated costs of testing, such as loss of wages. However, participants conveyed that testing should be convenient but that incentives alone were insufficient to overcome anticipated stigma associated with testing. There were concerns about whether lottery incentives were real and could be won. Observing others winning the lottery for testing served as “social proof”, that lottery prizes were winnable. When the prize was perceived to be of low value, the lottery did not motivate the uptake of testing services. Where participants had already decided to test for HIV, lottery incentives served as a “cue to action” and “sweetened the deal”, acting as a secondary motivator. Lottery incentives may serve as an added motivation for HIV testing uptake and offer an offset of financial barriers.
The use of fixed and lottery incentives promotes uptake of HIV testing, as noted in Fig. 2 (green star). While the use of lottery incentives to enhance the uptake of HIV testing services may serve as an added motivation [5, 6, 9, 10], and has increased the uptake of testing in children and adolescents, it has not proven beneficial in increasing men attending the clinic for post-HIVST counselling services. A well-designed lottery incentive intervention can be useful in promoting the intended target behaviour.
The Impact of Lottery based incentives on HIV Prevention ServicesFigure 2 above depicts the HIV prevention strategies (four articles) that examined the use of lottery incentives, aimed to motivate prevention behaviours. These prevention strategies included voluntary medical male circumcision (VMMC) and condom use. [4, 8, 27, 28] The use of oral pre-exposure prophylaxis (PrEP) is an effective prevention tool and has been incentivised using fixed financial incentives. [29] This review found no examples of lottery incentives being used to promote PrEP.
Voluntary Medical Male CircumcisionThree articles explored the use of lottery incentives in promoting uptake of VMMC. [4, 27, 28] Two articles reported findings from RCTs, which showed that lottery incentives did not significantly increase the uptake of VMMC. In an RCT conducted in Tanzania, lottery incentives were offered to participants contingent on their uptake of VMMC. There was a greater increase in the VMMC uptake in lottery intervention clinics (47%) than in the control group (8%), however, this increase was not statistically significant, shown in Fig. 2 (orange diamond). Smartphones were offered as the incentive, which participants reported to be irrelevant to their setting – where there was no electricity. The nature of the incentive is a critical consideration, and in this context small cash incentives or transport reimbursement were preferred. [4].
An RCT conducted in Kenya reported that fixed incentives were found to significantly increase VMMC uptake, compared to lottery and control groups. [4, 27] There was no statistical difference in the uptake of VMMC between the control and lottery groups. Fixed incentives offered $12.50 food voucher to all participants, lottery incentives offered a variety of prizes and probabilities, and the control group offered $0.60 cash. All incentives were contingent on having a VMMC done within three months. [27] Lottery incentive intervention offered a certainty of winning; with an 85% chance of receiving a $2.50 food voucher, 10% chance of winning a $45 standard phone or pair of shoes, and a 5% chance of winning a $120 bicycle or smartphone. [27] Both the fixed and lottery incentive groups had a certainty of winning a prize, with varied values. The minimum lottery incentive ($2.50) may have been inadequate to overcome physical, financial and psycho-social barriers to VMMC and may explain why fixed incentives were more effective. [27, 30, 31].
The third article described a discrete choice experiment conducted with 325 adult men in Tanzania, exploring preferences for VMMC. Men were divided into two groups by latent class analysis to test the hypothesis that men who engaged in more risky sexual activity would find lottery incentives more acceptable. An overwhelming majority of men (84%) showed a preference for transport vouchers over lottery incentives. [28] Where the behaviours are more complex (e.g., VMMC), participants may require a more definite form of compensation, such as fixed incentive or alternatively, a higher value lottery.
These findings highlight the importance of conducting formative research when designing lottery interventions to ensure these incentives are relevant and are sufficiently valuable to encourage target behaviours.
Condom UseLottery incentives have been tested for improving dual protection (contraception and condom use) amongst women, in Cape Town, South Africa. [8] Participants were incentivised to achieve an STI-free status by using condoms. At the six-month post enrolment visit participants were tested for STIs, and those who were negative received a lottery entry. The study found that lottery incentives increased the odds of returning to the clinic, as seen on Fig. 2 (orange diamond) and the uptake of dual protection which resulted in fewer STIs in the lottery group as compared to the control. [8].
These findings suggest that the nature of the target behaviour being incentivised is important. Complex behaviours such as VMMC may not be appropriate for lottery interventions, whereas comparatively simpler behaviours such as condom usage are strengthened by lottery incentives. While condom use does require partner negotiations and navigating complex social issues, it has fewer mitigating factors than undergoing VMMC which is a surgical procedure.
The Impact of Lottery Based Incentives on HIV TreatmentTreatment initiation, adherence and retention in care are vital for attaining viral suppression which in turn prevents onward transmission, disease progression and viral resistance; critical to achieving the UNAIDS 95–95-95 goals. [1, 2] A South African study showed that, following HIV testing, lottery incentives decreased the time it took for participants to register at a local clinic, but did not influence the rate of ART uptake between the intervention and control groups. [3] This same study also showed an increase in rates of viral suppression among participants who received lottery incentives, as seen in Fig. 2 (green star), but the viral suppression phase of the study was underpowered to make any definitive conclusions. [3] However, the improvement in linkage to care is significant, as the sooner PLHIV are initiated on ART, the sooner they can achieve viral suppression, through maintained adherence.
A USA-based study showed that lottery incentives improved the rates of ART adherence, among HIV-positive men and women. [7] Participants were incentivised to adhere to their treatment by receiving a fixed or lottery incentive when they tested virally suppressed at four- and eight-month follow-up visits. While both fixed ($300) and lottery incentive groups showed an increase in viral suppression, the lottery incentive was significantly more effective. Interestingly, this lottery was set up in such a manner that all participants were guaranteed to win a prize, the only variable was the amount of money they received (70% chance of winning $250 and 30% chance of winning $500). [7].
This is significant because receiving a prize was guaranteed. However, a guaranteed prize in and of itself is insufficient to encourage target behaviours as shown above with the VMMC study conducted in Kenya. Key differences with the intervention include the much higher value of the incentives and the comparative difference between the value of lottery and incentives. Considering that this was the only one of ten studies that was conducted in the USA, further research is needed to see if these results translate into a Sub-Saharan African LMIC context where HIV is most prevalent.
Although ART is a lifelong treatment, incentive-based interventions are only offered for a short period of time with the intention of building a habit that would sustain the behaviour change beyond the intervention period. In the USA-based study, participants expressed their commitment to maintaining medication adherence even after the intervention concluded (i.e., once incentives have stopped), but more information is needed to assess sustainability of treatment adherence. [7] Additional data is required to determine the optimal duration for providing incentives to encourage ART adherence. Research is needed to evaluate how the length of time for which the incentive is offered, affects this habit formation and the applicability across contexts, as well as the sustainability of lottery incentives as a public health intervention.
Figure 2 outlines the articles included in this review, which indicate the promise of lottery incentives, in improving linkage to care and motivating treatment adherence. While lottery intervention shows promise in supporting viral suppression in the short term, more data is needed to assess the long-term effects, particularly in Sub-Saharan African contexts.
Comments (0)