
Remember me






ACCORDING TO THE Centers for Disease Control and Prevention (CDC), heat illnesses are the leading cause of weather-related deaths in the United States, and their incidence has been increasing as global temperatures have risen (Buzan & Huber, 2020; CDC, 2022a). There were an average of 619 annual heat-related deaths in the United States recorded from 1999 to 2010 (CDC, 2122b). Heat-related deaths increased significantly during 2018–2020 to an annual rate of 1,022 (CDC, 2022a), and in 2022 1,670 deaths were reported (Reese, 2023).
Despite the universal concern among health experts about the danger of heat illnesses, that are expected to increase as ambient temperatures and humidity increase with ongoing climate change, there are no universal standardized protocols for management of heat-related illness in the emergency department (ED). The lack of a standardized approach has resulted in varying institutional and system approaches to care contributing to treatment delays, adverse outcomes, and deaths. This Research to Practice article reviews a systematic review conducted by Rublee et al. (2021) designed to synthesize existing evidence to develop a unified, evidence-based algorithm for management of heatstroke in the ED.
THE CASEA 45-year-old Hispanic male construction worker with an unknown medical history was brought to the ED by ambulance (emergency medical services [EMS]). EMS reports that the patient, who only speaks Spanish, was working on the roof of a new construction home in direct sunlight for the past 6 hours during a heatwave with temperatures at 97 °F, 60% humidity, and a heat index exceeding 120 °F. According to other workers on the scene, the patient suddenly collapsed and appeared disoriented and agitated before losing consciousness. The coworkers stated that the patient was on ground level at the time of the collapse and that it was witnessed by several of them. They told EMS that the patient had been acting normally until about 30 min before the collapse, at which time he seemed to be a little dazed and confused. One of his coworkers suggested that he come down from the roof and drink some of the sports drink they kept on site, which he did. He sat in the shade and drank a plastic cup of the sports drink. After a couple of minutes, he stood up to go back to work and collapsed and started to convulse for several minutes.
EMS reported that when they arrived, the patient was unconscious, wearing a long sleeve shirt, safety vest, long pants, and a hard hat. His Glasgow Coma Scale score was 6 (no eye opening 1, incomprehensible sounds 2, and flexion to pain 3). The patient's vital signs were: forehead temperature scan 105.6 °F (40.9 °C), heart rate 140 beats per minute, blood pressure 90/60 mmHg, respiratory rate 28 breaths per minute, and oxygens saturation of 92% on room air. His pupils were constricted, and he exhibited profound confusion upon stimulation. EMS removed his vest and shirt, loosened his pants, and applied chemical cold packs to his neck, bilateral axillae, and groin. They placed the patient on a cardiac monitor and obtained a 12-lead electrocardiogram (EKG), which revealed sinus tachycardia. They started a normal saline intravenous (IV) fluid bolus at 1000 ml/hr enroute.
Upon arrival in the ED, the patient was rushed directly into a resuscitation room where several actions all started simultaneously. A rectal temperature was recorded at 104.2 °F, with otherwise unchanged vital signs. The nurses started a second access line and performed an EKG. The EKG revealed sinus tachycardia at 138 beats per minute with a prolonged QTc and nonspecific T-wave abnormalities. The following laboratory examinations were drawn: complete blood count (CBC), complete metabolic panel (CMP), arterial blood gas, magnesium, phosphorous, troponin, prothrombin time/international normalized ration (PT/INR), urinalysis with microscopy and drug screen, lactic acid level, creatinine kinase (CK), acetaminophen, salicylate and blood alcohol levels, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Given the patient's altered mental status, a Foley catheter was placed to collect a urine sample and monitor urine output. At that time the nurse noted that the urine was dark, and tea colored. A portable chest radiograph was performed and interpreted at beside as unremarkable, and a stat CT head was ordered. Ice packs were placed on the neck, under the axillae and on the groin, and two fans were pointed toward the patient. Differential diagnosis included heat syncope, heatstroke, heat exhaustion, sepsis, seizure, and cerebrovascular accident.
RESEARCH ARTICLERublee, C., Dresser, C., Giudice, C., Lemery, J., & Sorensen, C. (2021). Evidence-based heatstroke management in the emergency department. Western Journal of Emergency Medicine, 22(2), 186–195. doi:10.5811/westjem.2020.11.49007
Purpose, Design, and MethodsThe purpose of Rublee et al.'s (2021) literature review was to evaluate existing standards of care for management of acute hyperthermia/heat illness to develop an evidence-based algorithm to standardize and expedite care of heatstroke patients in the ED. The authors (Rublee et al., 2021) emphasize that despite existing national emergency medical service (EMS) protocols for the prehospital care of hyperthermic patients (National Association of State EMS Officials Medical Directors Council, 2017) their use varies by state and institution. There are also consensus-based protocols for exertional heat illness published by the American College of Sports Medicine (Roberts et al., 2023) and by the Wilderness Medicine Society (Lipman et al., 2019); however, there are no established evidence-based protocols for care of heatstroke patients once they arrive in the ED. Because early recognition and rapid cooling of a patient experiencing a heat illness is time sensitive to prevent multisystem organ failure or death, Rublee et al. (2021) conducted their systematic review to create an algorithm for care that could be easily incorporated into electronic medical record systems with a goal of triggering clinician alerts, similar to what are in place the care of patients presenting with signs of stroke, sepsis, or myocardial infarction, to expedite care and reduce a patient's risk of death.
Rublee et al.'s (2021) review consisted of examining key journals, PubMed and Embase databases, and bibliographies for all articles related to heatstroke defined as elevated core body temperature, altered mental status, elevated ambient temperatures, and/or exertion. Studies that described treatment strategies and outcomes were also included (Rublee et al., 2021). Quantitative research articles, case studies, and qualitative studies published as consensus recommendations by major health organizations including United States Occupational Safety and Health Administration, the World Health Organization, non-peer-reviewed prehospital articles, expert opinion articles, and EMS and military reports were included in the analysis. Because two different databases and a wide range of articles and materials were included in the search strategy, the review did not qualify as a PRISMA systematic review or meet the requirements for a meta-analysis (Rublee et al., 2021).
The review excluded studies that were not published in English, articles that described heatstroke pathophysiology but did not include treatments, and articles that were not full text. All articles were reviewed by two, independent, blinded, physician investigators to ensure interrater reliability for adherence to inclusion/exclusion criteria and agreement on Grading of Recommendations Assessment, Development, and Evaluation scoring of evidence quality (Rublee et al., 2021). Data were examined for treatment themes by setting (prehospital, ED, and intensive care unit [ICU]), population (adult versus pediatric including diverse geographic settings), care management (recognition, cooling, treatment, and systems), cooling method, patient outcome, and type of heatstroke (exertional, occupational, and classic).
ResultsOf the 183 articles initially identified in the search, only 63 articles met inclusion criteria and were included in the analysis (Rublee et al., 2021). None of the studies were ranked as high quality, 25 were ranked as low quality, and 25 as moderate quality. The analysis yielded three major themes for guiding treatment: (1) recognition, (2) rapid cooling, and (3) supportive care (Rublee et al., 2021).
Recognition was defined as considering the diagnosis, having awareness of weather conditions, measuring core body temperatures, and initiating cooling interventions (Rublee et al., 2021). Cooling interventions included removal from the hot environment, application of cold packs/ice, fanning and evaporative cooling methods, ice or cold water immersion, fluid resuscitation, internal or endovascular cooling techniques (gastric/bladder/or rectal), and extracorporeal membrane oxygenation cooling (Rublee et al., 2021).
Rapid cooling methods ranged from ice water or cold water immersion to intravascular cooling catheters and evaporative cooling for intubated or obtunded patients (Rublee et al., 2021). The authors discussed that although cold water immersion is the gold standard with a Grade 1A recommendation by the Wilderness Medicine Society (Lipman et al., 2019) their analysis found no definitive approach to cooling identified as superior (Rublee et al., 2021).
Supportive care focused on laboratory findings predictive of adverse outcomes, and airway, breathing, and circulation resuscitation guidelines (Rublee et al., 2021). Electrolyte abnormalities found to be associated with heatstroke risk of death included either elevated or low sodium, potassium, phosphorous, and calcium, an aspartate aminotransferase more than 1,000 units, elevated lactate, and elevated troponin l, and creatinine levels (Rublee et al., 2021). Delayed cooling was also a risk. The authors also noted that at-risk populations include older adults who present most often with classic heatstroke, and outdoor workers, intermediate-skill level runners, and military personnel who are all more likely to present with exertional heatstroke (Rublee et al., 2021). The authors found no articles describing integrated system-level approaches that expedite treatment by triggering early recognition of heatstroke from the prehospital setting through EMS transfer to care in the ED.
Limitations/StrengthsThe authors cited that their study's strengths included an extensive review of all available literature on heatstroke encompassing 64 years (Rublee et al., 2021). They also stressed that their search strategy that incorporated qualitative, quantitative, case report, and consensus recommendations yielded a broad analysis of important factors associated with heatstroke outcomes (Rublee et al., 2021). Another strength was that the articles reviewed spanned different geographic regions, populations, as well as care settings (Rublee et al., 2021). A major limitation of their review was that most studies included were graded as having a low to moderate quality of evidence using GRADE criteria scoring (Rublee et al., 2021).
ConclusionsThe authors discussed that their review found significant, system-level gaps in the care of heatstroke victims in the ED that contribute to adverse outcomes (Rublee et al., 2021). The major risk factor identified was delayed cooling that leads to pathophysiologic metabolic alterations resulting in multiorgan system failure, severe sequelae, or death. Recognition of heat illness requires obtaining core body temperatures early to trigger cooling interventions, ideally, within the first 30 min (Rublee et al., 2021). The authors also emphasize that cooling should begin in the prehospital setting and continue during transfer using whatever methods are available (Rublee et al., 2021). Once in the ED, support of airway, breathing, and circulation with prompt initiation of cooling measures should begin within 10 min and continue until the patient's core temperature reaches 39° C within a goal of 30 min. Cooling measures should be stopped at 39° C, and core temperatures should then be continuously monitored to ensure continued improvement and to prevent overcorrection and development of hypothermia (Rublee et al., 2021).
Cold or ice water immersion has been found to be the most effective cooling modality rapidly reducing organ and tissue temperatures while improving tissue perfusion by vasoconstricting peripheral and skin vessels to improving hemodynamic stability (Douma et al., 2020; Rublee et al., 2021). Shivering should be controlled by administering benzodiazepines because shivering promotes heat retention. IV hydration using chilled fluids is also recommended (Rublee et al., 2021). Urinary output is best measured with insertion of a Foley catheter, and insertion of a three-way catheter can also be used for cold water bladder irrigation if aggressive internal cooling is needed (Rublee et al., 2021).
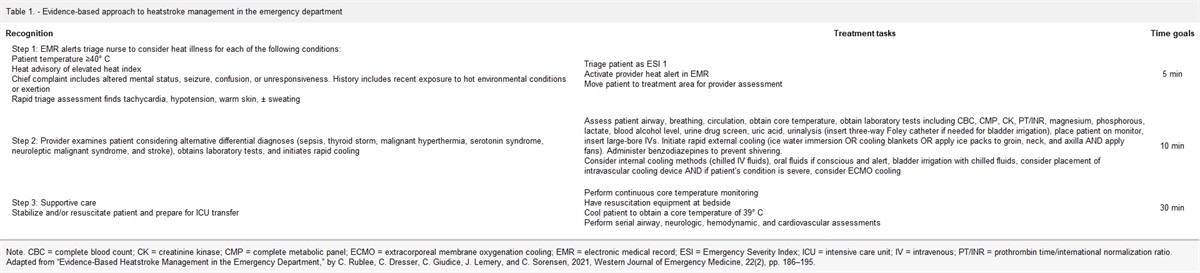
ED workup should include a CBC, CMP, CK, troponin l, prothrombin time/international normalized ratio (PT/INR), urinalysis, lactate, and uric acid, to monitor for muscle, organ and tissue damage, and a blood alcohol level and urine drug screen to rule out other causes of altered mental status. For patients suspected of having a cerebrovascular accident, cooling must precede imaging (Rublee et al., 2021). Based on their review and analysis, Rublee et al. (2021) developed a heat alert process and treatment algorithm as summarized in Table 1 that incorporates the themes of recognition, rapid cooling, and supportive care processes.
Table 1. - Evidence-based approach to heatstroke management in the emergency department Recognition Treatment tasks Time goals Step 1: EMR alerts triage nurse to consider heat illness for each of the following conditions:Note. CBC = complete blood count; CK = creatinine kinase; CMP = complete metabolic panel; ECMO = extracorporeal membrane oxygenation cooling; EMR = electronic medical record; ESI = Emergency Severity Index; ICU = intensive care unit; IV = intravenous; PT/INR = prothrombin time/international normalization ratio. Adapted from “Evidence-Based Heatstroke Management in the Emergency Department,” by C. Rublee, C. Dresser, C. Giudice, J. Lemery, and C. Sorensen, 2021, Western Journal of Emergency Medicine, 22(2), pp. 186–195.
As ED providers it is imperative that they maintain situational awareness of environmental conditions to recognize a potentially life-threatening heat illness in patients presenting to the ED. According to the CDC's Heat and Health Tracker site, https://ephtracking.cdc.gov/Applications/heatTracker/, the number of heat-related ED visits surged in June and July of 2023 in Texas, Arkansas, Louisiana, New Mexico, and Oklahoma during record-breaking heat waves. Record high visit rates also occurred in the Northeast, Upper Midwest, and Rocky Mountains during April, and in Idaho and the Pacific Northwest during April and May.
Populations at greatest risk include older adults, young children and infants, individuals who lack adequate housing or air conditioning, and individuals with disabilities and psychiatric conditions (Rublee et al., 2021). Risk factors also include obesity, preexisting cardiovascular and respiratory diseases, use of methamphetamines and cocaine, and use of any medication that can interfere with thermoregulation. At-risk medications are included in Table 2.
Table 2. - Medications that can interfere with normal temperature regulation Alcohol Calcium channel blockers Amphetamines Selective serotonin reuptake inhibitors Anticholinergics Thyroid medications Antihistamines Clopidogrel Antipsychotics Neuroleptics Benzodiazepines Phenothiazines Diuretics Antidopaminergic medications β-blockers AntidepressantsHeat illnesses range on a continuum from minor conditions such as heat edema and heat cramps, to more serious conditions, such as heat syncope and heat exhaustion, to life-threatening heatstroke, which can rapidly progress. Athletes, outdoor workers, and agricultural workers are more likely to experience exertional heatstroke that occurs when muscular activity increases core temperatures while exposed to elevated ambient temperatures. Older adults and children are more likely to experience classic heatstroke that occurs when normal physiologic temperature regulation mechanisms become overcome when exposed to elevated ambient temperatures (Lipman et al., 2019; Roberts et al., 2023). As Rublee et al. (2021) emphasize the most important step in preventing minor heat illness from progressing to heatstroke is recognizing it, obtaining and monitoring core temperatures, initiating rapid cooling, and continuing cooling methods while providing supportive care until the core temperature reaches 39 °C. Signs and symptoms of heatstroke are summarized in Table 3.
Table 3. - Sign/symptoms of heatstroke and heat exhaustion Persistent mental status changes Confusion Irritability Hot, pale/flushed skin ± Sweating Weakness Ataxia Delirium Personality changes-combativeness/aggression Seizure Coma Vomiting Tachycardia Hypotension Weak pulse Stool incontinence Core temperature > 40° C or 104° F Decorticate/decerebrate posturing Note. Adapted from LoVecchio (2020) and “ACSM Expert Consensus Statement on Exertional Heat Illness: Recognition, Management and Return to Activity,” by W. Roberts, L. Armstrong, M. Sawka, S. Yeargin, Y. Heled, and F. O'Connor, 2023,. Current Sports Medicine Reports, 22(4), pp. 134–149.Part of the challenge in rapid identification of a patient experiencing heatstroke or heat exhaustion is that the symptoms are nonspecific and common in other serious medical conditions, which complicates the diagnostic process. Table 4 lists a variety of medical conditions that may mimic heatstroke that providers must consider and rule out as part of the diagnostic workup.
Table 4. - Differential diagnosis of heatstroke Sepsis Meningitis Encephalitis Malaria Typhoid Tetanus Thyroid storm Pheochromocytoma Diabetic ketoacidosis Cerebrovascular accident Hyponatremia Infection Seizure/status epilepticus Anticholinergic toxidrome Sympathomimetic overdose Salicylate overdose Serotonin syndrome Malignant hyperthermia Neuroleptic malignant syndrome Alcohol and benzodiazepine withdrawalNote. Table created by Dian Evans.
Rublee et al.'s (2021) algorithm, despite the recommendations based on low- to moderate-quality evidence, provides a useful, unified approach to care with time-sensitive goals that can help to expedite ED care. Interestingly, Rublee et al. (2021), along with the authors of the Wilderness Medicine Society's clinical practice guidelines (Lipman et al., 2019) and the American College of Sports Medicine's expert consensus statement on exertional heatstroke management (Roberts et al., 2023), and the authors of 2020 systematic review and meta-analysis (Douma et al., 2020), all comment that most of the research comparing specific cooling techniques have been conducted on healthy volunteers subjected to heat stress conditions that may not be the same when used with actual patients in prehospital or ED settings. However, the universal recommendation among all researchers and clinicians is to start cooling as rapidly as possible by removing the patient from a hot environment, exposing the skin, immersing in cold/ice water, if available, or applying whole body ice or chemical cold packs to the cheeks, palms, soles of feet (Lipman et al., 2019) or groin, axilla, and neck (Roberts et al., 2023). Fans and air conditioning should be used to circulate air to promote evaporation. Supportive care with IV hydration is used to maintain hemodynamic stability or to treat rhabdomyolysis while addressing airway, breathing, and circulation. Resuscitation should not interrupt cooling (Helman, 2022). Cooling measures should also not be stopped during patient transport and must continue until the patient's core temperature reaches 39 °C to prevent the patient from developing shock, multisystem organ failure, or disseminated intravascular coagulopathy, or intestinal ischemia (Lipman et al., 2019; Roberts et al., 2023; Rublee et al., 2021).
ED providers can use the National Oceanic and Atmospheric Administration's heat index calculator (https://www.wpc.ncep.noaa.gov/html/heatindex.shtml) to monitor weather conditions and consult the National Weather Service's heat index chart (https://www.weather.gov/safety/heat-index) to be aware of excessive heat conditions that expose vulnerable and healthy persons to conditions that can predispose to the development of classic or exertional heatstroke.
CASE REVISITEDWhile the initial assessment was underway, 2 L of oxygen was initialed by nasal canula, and a rectal temperature was taken showing a core temperature of 41 °C. The patient was immediately placed in a body bag filled with ice water covering his torso and lower extremities for more aggressive rapid cooling. Chilled IV crystalloid boluses replaced his initial fluid bolus. Two milligrams of IV lorazepam was given to control his shivering and for his increasing agitation once rapid cooling was initiated. Repeat rectal temperatures were taken every 5 min. His core temperature decreased to 39 °C within 20 min as he became more alert and began to complain of discomfort. At this point he was removed from the body bag with continued core temperature and vital sign monitoring.
When his spouse arrived at the ED, she stated that he took a high blood pressure pill called hydrochlorothiazide. She reported that he would usually have a couple of beers at night after work, and he never used tobacco products or recreational drugs. Diuretic medications and alcohol can both interfere with thermoregulation during excessive heat conditions.
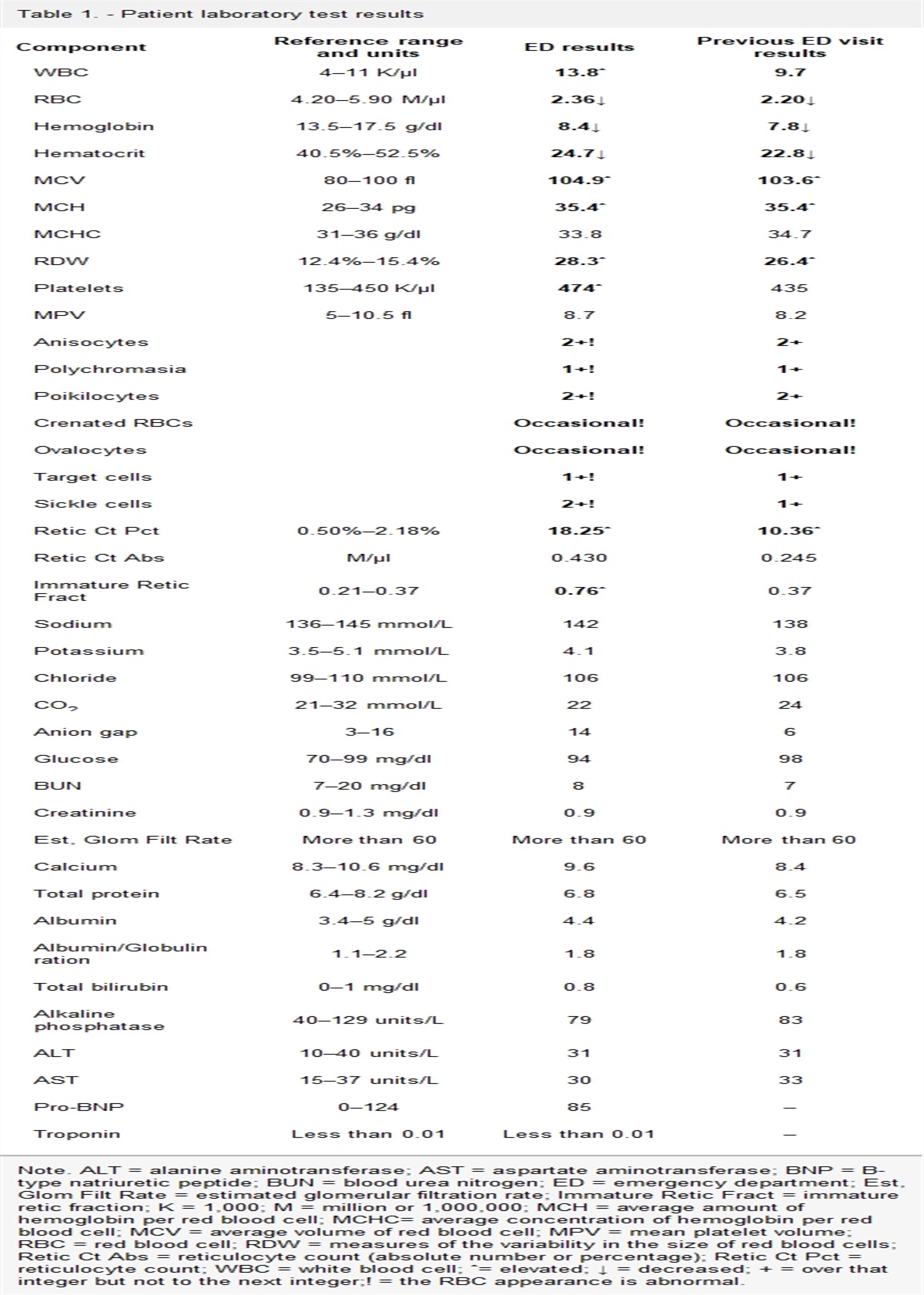
His laboratory tests were notable for: arterial blood gas revealed a pH of 7.25 (normal 7.35–7.45). PaCO2 was 25 (normal 35–45 mmHg), HCO3 was 17 (normal 22–28 mEq/L), and PaO2 was 28 (normal 38–44). CMP results included sodium at 152 (normal 135–145 mEq/L), potassium at 2.9 mEq/L, creatinine 1.46 mg/dL (normal is 0.6–1.2 mg/dL), alanine aminotransferase (ALT) at 70 U/L (normal 0–40 U/L), and aspartate aminotransferase (AST) at 56 U/L (normal 0–35 U/L). The patient's white blood cell count was 19 109/L, hemoglobin 22 g/dl, and hematocrit 60%. The metabolic acidosis combined with the elevated electrolytes and creatinine are all likely due to dehydration from sweating. The high sensitivity troponin was 18, and while within the normal range, it was high. This elevation is likely due to demand ischemia secondary to the elevated respiration rate and heart rate. CK level was 7,500 U/L (normal 20–300 U/L). This, in conjunction with the tea-colored urine, demonstrated rhabdomyolysis. Once the urinalysis resulted, the patient was found to have proteinuria and elevated red blood cells. The ESR and CRP were also elevated, which is often seen as part of the coagulation cascade and system inflammatory response during a heatstroke.
The patient was admitted to the ICU for further intensive management including hydration, cooling, potassium repletion, continued temperature, neurologic, organ system, and hemodynamic monitoring, and treatment of rhabdomyolysis. His admission diagnoses included acute exertional heatstroke, hypokalemia, transaminitis, metabolic acidosis, and rhabdomyolysis. He was transferred to the ICU from the ED 70 min post-arrival with an improved Glasgow Coma Scale of 12. Discharge vital signs showed a rectal temperature of 39 °C, blood pressure of 110/70, heart rate of 105, and a respiratory rate of 22. Three days later he was discharged from the hospital in good condition with primary care follow-up to monitor for possible late-occurring organ system sequelae and for return-to-work restrictions.
CONCLUSIONEarly recognition and rapid treatment of heat illness requires time-sensitive and aggressive management. ED providers must maintain awareness of weather patterns that can predispose vulnerable, or even healthy persons, to heat stress, and consider heat illness when assessing a patient with altered mental status during high temperature days. Situational awareness can trigger early recognition and management of heat illness that can shift a patient's heat stress trajectory and save their life.
Nurse practitioners can do much to educate patients and the public about the risk of heat illnesses including advising on how to stay aware of weather conditions, use heat index charts to plan physical activity, gradually acclimatize when preparing to work or exercise in excessively hot temperatures, and of the importance in taking work breaks to cool off and hydrate.
Reviewing and understanding heat illness pathophysiology and the mechanisms of heat gain/loss is important so that providers and responders can improvise when initiating cooling methods. This is particularly important when resources are limited or when they have to respond out of a hospital or controlled setting. The articles by Douma et al. (2020),Roberts et al. (2023), and Lipman et al. (2019) each include excellent discussions of heat pathophysiology and heat/gain principles that can inform and guide management in atypical settings.
Comments (0)