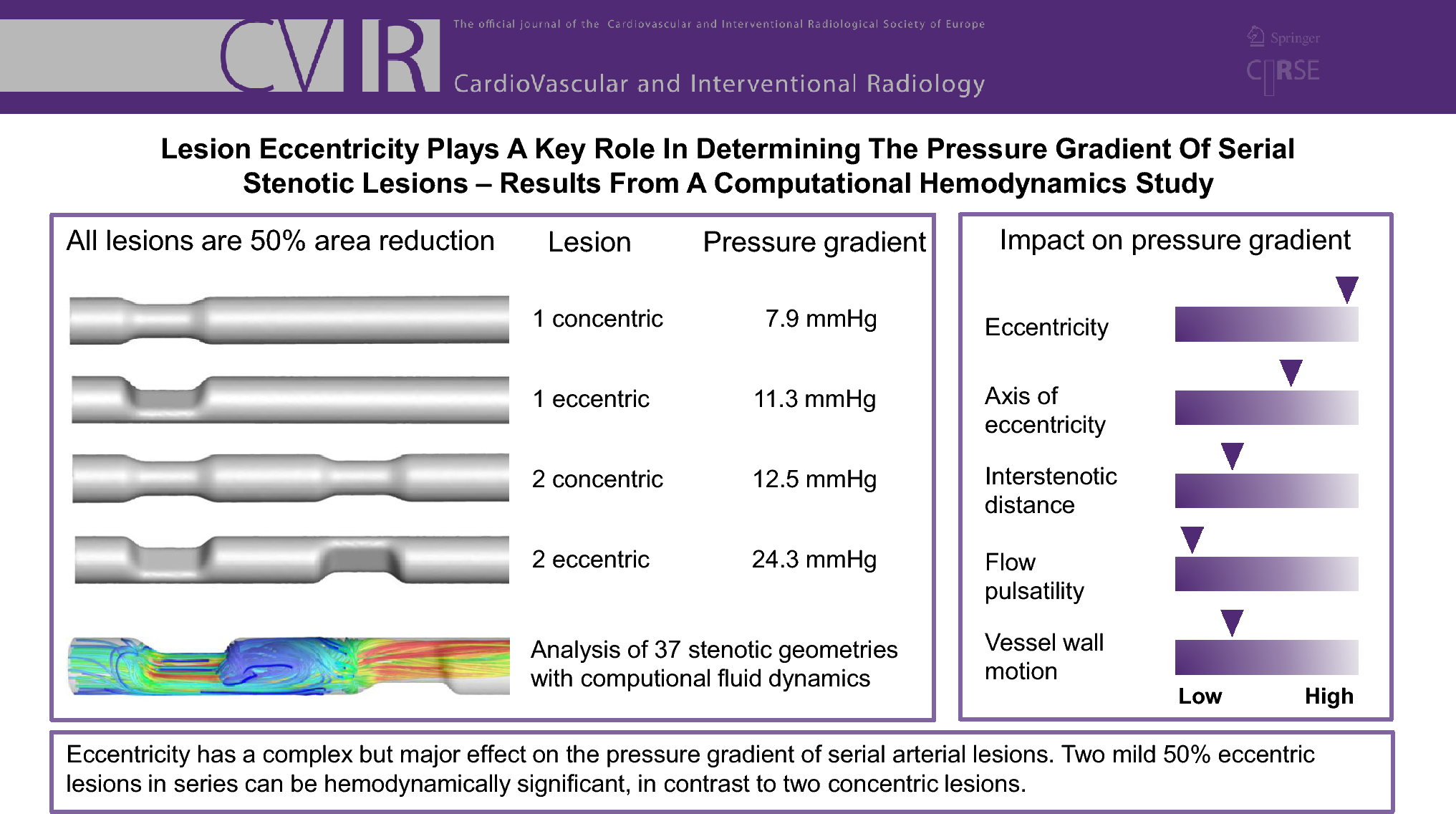
The decision whether to treat two subclinical stenoses is difficult in clinical practice, as it is unclear what the threshold for combined hemodynamic significance is. Traditional measures like the percentual diameter or area reduction or the Doppler peak systolic velocity ratio do not reflect the additive effect but only assess the severity of the most severe stenosis [3]. This simulation study demonstrated that eccentricity is a key element in the hemodynamic significance of both single and serial 50%-area lesions. Two unfavorably arranged semicircular eccentric lesions demonstrated a gradient of 24 mmHg, relative to 12 mmHg for two concentric lesions of equal area reduction. Furthermore, for two eccentric lesions, the combined pressure gradient at high flow rates was often found to exceed the sum of its two isolated lesions, highlighting the adverse impact of eccentricity in serial lesions. In symptomatic patients with one or more subcritical (e.g., < 75% area) eccentric lesions, this suggests that treatment of the lesion(s) may improve symptoms.
The role of eccentricity was complex and flow rate-dependent. This has also been demonstrated for single stenotic lesions, where eccentricity did not increase the pressure gradient for low flow rates (Reynolds number 10–1000) [9], but with two-fold increases for moderate flow rates (Reynolds number > 1000) [10]. In this study, the impact of eccentricity also increased for higher flow rates, which can explain the 22.7% discordance between resting gradient and hyperemic gradient classification of serial lesions [12]. For two lesions that involved the most eccentric E2 lesion, the combined pressure gradient exceeded the sum of its two isolated lesions for a high flow rate, which was never the case for a moderate flow rate. This observation indicates that moderate serial eccentric lesions may combine to hemodynamic significance in exercise conditions. This could have important consequences for symptomatic patients with mild serial eccentric lesions on anatomic or duplex ultrasound evaluation [4], which may currently not be referred for treatment or for a physiologic evaluation. Eccentric lesions are very common in both the femoral (64%) [19] and the coronary arteries (45.6%) [20]. For clinical evaluation of stenotic disease, it is therefore important to appreciate the increased likelihood of hemodynamic significance of two mild lesions when they have an eccentric shape. In these cases, diagnostic thresholds are not possible with duplex ultrasound and are hard to make with CTA, and depending on the localization, an exercise ankle-brachial index or invasive pressure measurement might be needed.
Two other geometric effects that were investigated were the interstenotic distance and the relative rotation of the eccentric lesions. For most cases, an increase in the interstenotic distance was associated with increase in the pressure gradient, with some exceptions, notably for cases with a distal E2 stenosis. These exceptions conflict with previous studies where an increase in interstenotic distance was exclusively associated with an increase in the pressure gradient [5, 11]. This discrepancy is likely explained by the importance of the inflow profile into the distal stenosis. In the E2 cases, the proximal stenosis led to inflow disturbances into the distal stenosis that increased outflow disturbances and the pressure loss of the distal stenosis. This hemodynamic interaction is similar to a previous observation [5] that a proximal 75% concentric stenosis with a distal 50% concentric stenosis caused a higher pressure gradient compared to a reverse configuration. The effects of interstenotic distance were usually below 10%, however, and without a clear trend making the impact of minor relevance for clinical practice for peripheral arteries. For coronary arteries, serial stenotic lesions with an interstenotic distance below three reference vessel diameters are treated as a single lesion in the SYNTAX I and II scores [21], which may underestimate the significance of these lesions when used for individual risk prediction. Particularly when of eccentric shape, such lesions are likely better assessed with invasive or computational physiologic evaluation.
With respect to the relative rotation of eccentric lesions, a consistent trend was present for the baseline flow where a 90° rotation caused 10–20% higher pressure gradients than for a 0° or 180° rotation. For the high flow rate, this trend was still present but less consistent. In clinical practice, the adverse 90° rotational configuration of serial eccentric lesions is difficult to assess with angiography but can be assessed on pre-operative CTA for lesions with an uncertain indication for intervention.
A two-fold increase in flow rate led to a roughly three-fold increase in the pressure gradient across the serial stenotic models. The high flow rate was considered representative of the peak flow rate during systole or the mean flow rate during exercise and led to a hemodynamically significant pressure gradient of over 20 mmHg [22] for eight of the 34 models. The three-fold increase is in line with the theoretical relation of the pressure gradient to the sum of a viscous pressure—linearly related with flow rate—and an inertial pressure loss that scales with the square of the flow rate [8].
Flow pulsatility with a single harmonic oscillation did not significantly alter the pressure gradient for non-compliant walls. The addition of wall deformability led to high-frequent flutter in the CMM method with a significantly increased energy loss. In the comparably more realistic ALE, this behavior was absent, and the flow field largely resembled the rigid wall simulations, with an increase in the pressure gradient of about 10%. An exception was formed by the E2–E2 model, in which a lumen straightening was present during systole, limiting flow recirculation and decreasing the pressure gradient. This behavior is likely unrealistic in diseased peripheral arteries, and the application of higher elasticity of external tissue support would limit vessel displacement.
In the ALE method, a thick wall, the nonlinearized kinematics, and external tissue support including viscous energy loss were modeled. These factors, absent in the presently applied CMM method [14], more realistically represent a bounded vessel wall and likely stabilized the fluid–structure interaction from the growth of the spurious oscillations. In calcified lesions, the wall motion will be decreased [23], limiting the observed effects of the simulated healthy vessel wall. For lipid-filled plaques [23] and vessel diseases that structurally weaken the vessel wall, such as fibromuscular dysplasia, the effects of wall motion may be amplified, and perhaps oscillatory fluid–structure interaction modes can be present. For multifocal fibromuscular dysplasia with a typical string-of-beads appearance, such an effect may contribute to the unexpectedly high pressure gradients that have been described in a few patient cases [24, 25].
The effects described in this study were observed for computational models of 6-mm arteries. They can reasonably be generalized to similarly shaped 50%-area stenoses in arteries of other diameters if similar velocities are present (spatiotemporal mean velocity of 53 cm/s for resting flow). This is because in the present Reynolds numbers (Re = 1000), inertial effects dominate (inertial effect accounts for > 70% of pressure gradient for a 50% stenosis at a Reynolds number of 1000), in which case the pressure gradient is mostly influenced by the stenotic area reduction and flow velocity, and less so by the Reynolds number [8]. Other factors such as systemic blood pressure have no direct effect on the pressure gradient but can have an impact through changes in the flow velocity.
Study Limitations
An important limitation for translating the results to clinical practice of this study is that only three smooth stenotic shapes were assessed. Stenotic morphology in patients is highly variable, and especially calcified plaques are characterized by surface irregularity. For assessing flow mechanics in the variety of stenotic shapes in patients, image-based computational fluid dynamic simulations are an attractive and validated method for coronary lesions [26]. For peripheral arteries, computational fluid dynamic simulations of a patient’s geometry can furthermore be informed with a patient’s temporal flow profile obtained from duplex ultrasound [27]. Calcified plaques are difficult to quantify accurately using non-invasive imaging and may require intra-vascular ultrasonic or optical imaging [28] for accurate simulations. It would be of interest to investigate whether the observed adverse effect of eccentricity also holds for other stenotic degrees and whether a correlation between eccentricity index [20] and pressure gradient is present in patients.
Further simplifications of this study were the single harmonic flow waveform and the assumption of a Newtonian fluid model. For the infrarenal aorta and its peripheral arteries, the biphasic or triphasic flow will likely lead to more complex flow phenomena, although the mean pressure gradient may not be strongly affected. The inclusion of power-law viscosity model was previously shown to minimally alter the pressure gradient in serial stenotic lesions [11].



留言 (0)