
記住我





A 46-year-old Filipino gentleman presented to the emergency department with a decreased vision for one month. He also reported three months history of tremors and palpitations. There was no history of headache, weakness, numbness, altered level of consciousness, unintentional weight loss, chronic diarrhea, insomnia, shortness of breath, neck swelling or pain. The patient was diagnosed with hypertension five months ago and took atenolol 50 mg once daily for management. There was no family history of thyroid or autoimmune diseases. The patient did not smoke or drink alcohol.
On physical examination, the patient had high blood pressure (176/86) with a normal heart rate, respiratory rate, temperature and oxygen saturation. He had mild bilateral hand tremors. Neurological examination revealed bitemporal hemianopia. He had a firm, diffuse, non-tender thyroid swelling. There was no proptosis, lid retraction, lid lag, muscle weakness, thyroid bruit, or skin changes. The patient had a pale left-sided optic disc on the fundus examination. The cardiac, respiratory and gastrointestinal examination was normal.
Laboratory examination showed a normal complete blood count and renal and liver function tests. Serum TSH was 3.35 (reference range 0.3–4.2) mIU/L, FT3 was 19.7 (3.7–6.4) pmol/L, and FT4 was 68.9 (11-23.3) pmol/L. Repeated thyroid function tests (TFT) showed similar results. The serum TSH receptor antibody was positive (11.5 mIU/L; Cut-off ≥ 1.75 mIU/L). Serum sex hormone binding globulin (SHBG) was high (126 nmol/L; reference range: 18.3–54.1 nmol/L). The rest of the pituitary hormonal profile was normal.
A thyroid ultrasound showed enlarged inhomogeneous echogenicity and increased vascularity, indicating diffuse thyroid disease. MRI of the pituitary gland showed a large sellar/suprasellar mass of intermediate T1 signal and a mixture of hypo and hyperintense signal in T2 with moderate enhancement. Optic chiasm was elevated and bowed over the superior border. The anterior carotid artery was displaced superiorly with no encasement, and the tumor was contacting the left cavernous internal carotid artery (ICA) (Fig. 2).
Fig. 2
Sagittal and coronal views of Magnetic Resonance Imaging (MRI) of the pituitary gland at the initial presentation showing large enhancing sellar and suprasellar mass lesion (a), compressed and elevated optic chiasm (b), and tumor contacting cavernous portion of the internal carotid artery (c) and sphenoid sinus (d)
The patient was diagnosed with TSHoma with possibly co-existing Grave’s disease (due to the presence of positive TSH receptor antibody and diffuse thyroid enlargement). Octreotide, subcutaneous 100 mcg twice a day, was started. Repeat TFTs showed a decrease in TSH level to 0.45 mIU/L (> 50% reduction) and a decrease in FT4 to 50.9 pmol/L. At this point, carbimazole 20 mg twice daily was added, further decreasing FT4 to 39.9 pmol/L. Due to a lack of availability, the TRH stimulation test was not performed. The patient underwent navigation-assisted trans-nasal, trans-sphenoidal endoscopic resection of pituitary macroadenoma. Repeat MRI pituitary 48 h post-operation showed a solid residual enhancement measuring 28 × 24.5 × 19.5 mm (Fig. 3).
Fig. 3
Post-operative Magnetic Resonance Imaging (MRI) of the pituitary (post-contrast) gland showing debulking of the tumor (arrows)
The histopathology revealed marked perivascular and interstitial fibrosis. Immunohistochemistry (IHC) staining was negative for Adrenocorticotrophic hormone (ACTH), Prolactin, Growth Hormone (GH), Follicle Stimulating Hormone (FSH), Thyroid Stimulating Hormone (TSH) and Luteinizing Hormone (LH), and positive for synaptophysin. (Fig. 4).
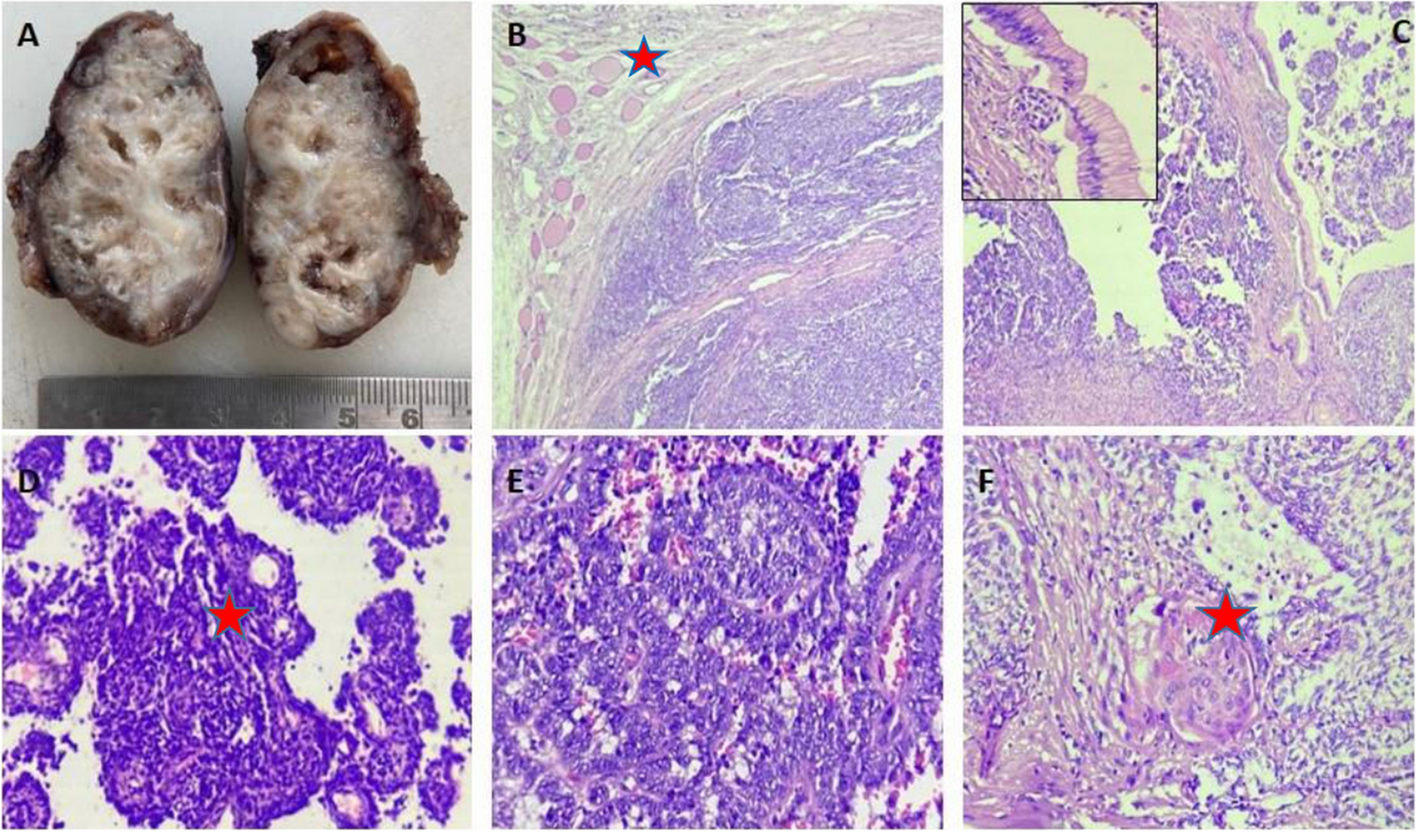
Fig. 4
Histopathology and immunohistochemistry of the resected pituitary tissue specimen. Sections show fragments of neuroendocrine tumor in a background of abundant fibrin deposition and hyalinized small blood vessels (black arrow fibrin) (A). The tumor cells are monomorphic with round nuclei and vesicular chromatin. No necrosis or mitotic figures seen (Black arrow hyalinized blood vessel, white arrow tumor cells) (B). By immunohistochemistry, tumor cells are strongly positive for synaptophysin (C), chromogranin (D) and cytokeratin CK AE1/AE3 (E) confirming the neuroendocrine origin of the neoplasm. Meanwhile, all other hormonal markers including TSH are negative (F)
Given the unexpected histopathological finding, the alpha subunit pituitary tumor marker level was sent and was positive (0.6 ng/ml, cut off for normal is </= 0.5 ng/ml), supporting the diagnosis of TSH secreting pituitary adenoma. An NM Ga68 DOTATATE whole-body PET CT (somatostatin receptor scintigraphy) showed significant uptake in the pituitary macroadenoma (Fig. 5). A positiveGa68 DOTATATE is suggestive of functioning pituitary tissue in the adenoma [13].
Fig. 5
Sagittal and coronal views of 68-Gallium DOTA peptide Positron Emission Tomography (Ga68 DOTATATE PET CT) of the pituitary gland with the arrow showing significant uptake corresponding to pituitary macroadenoma
The patient had a nuclear scan of the thyroid gland (192 MBq Tc 99 m pertechnetate), demonstrating features suggestive of GD (diffusely increased homogeneous uptake and thyroid uptake was 36%).
On follow-up, the patient had persistent visual field defect but noticed much improvement in right eye vision and mild improvement in left eye vision. A follow-up pituitary MRI showed a stable residual tumor size. The optic chiasma was still compressed and elevated more on the left side. The patient was offered a second surgery, but he refused and opted for medical management. He is now on octreotide intramuscular injection of 20 mg every four weeks and carbimazole 10 mg once daily with the latest TFTs in the normal range. His latest MRI pituitary performed one year after the surgery shows regression in the size of the residual pituitary adenoma measuring 24 × 22 × 19 mm (Fig. 6).
Fig. 6
Follow-up Magnetic Resonance Imaging (MRI) of pituitary gland 1-year post operatively showing regression in lesion size. The optic chiasm is decompressed (arrow)
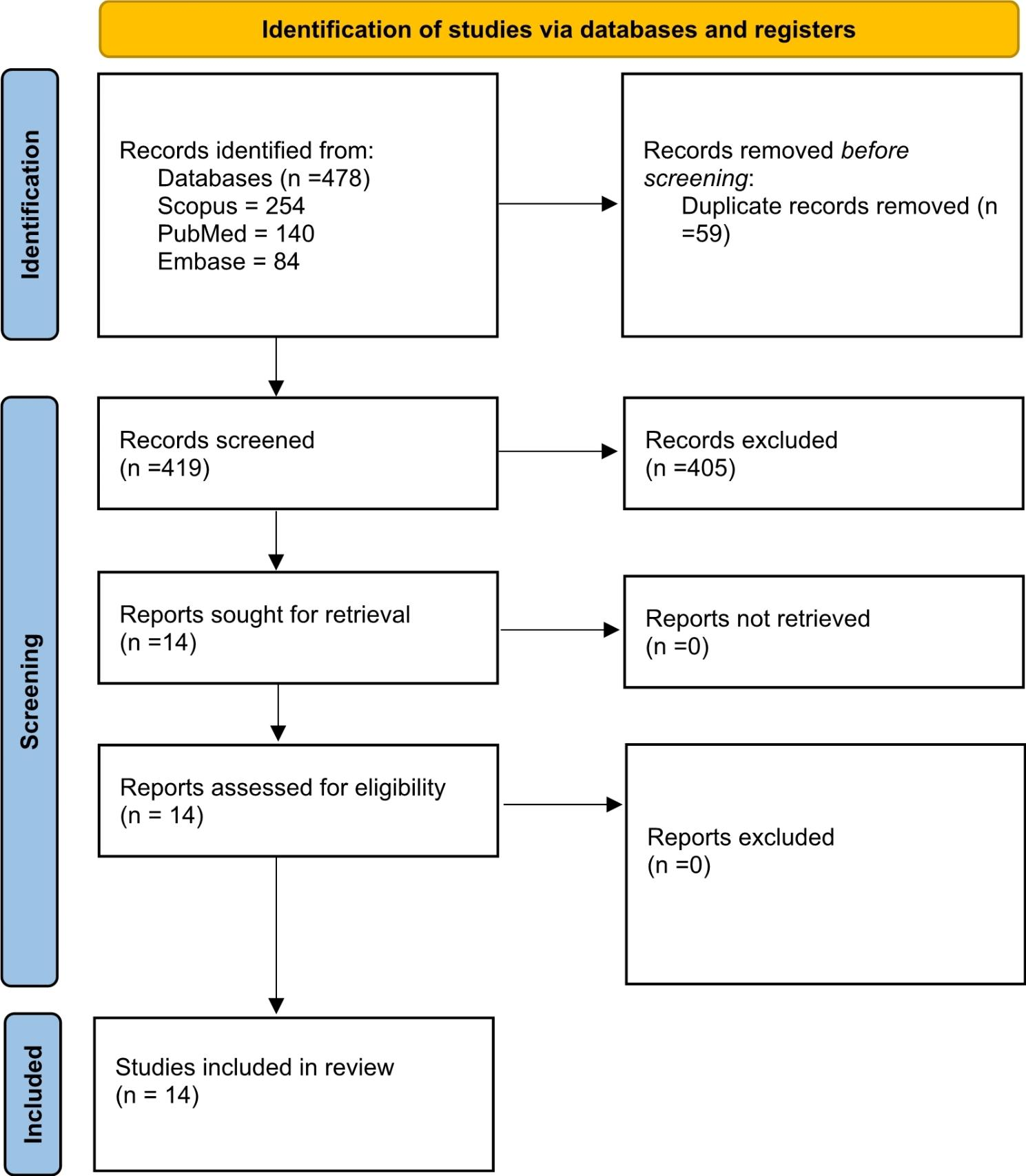
Systematic review resultsFourteen case reports fulfilled the eligibility criteria [8,9,10, 14,15,16,17,18,19,20,21,22,23,24]. Table 1 summarizes the clinical details of the added cases.
Table 1 Clinical characteristics and outcomes of patients included in the studyTable 2 summarizes the demographic, clinical/laboratory characteristics, and outcomes of patients with TSHoma and GD. A total of 16 patients (including the current case) were included in the systematic review.
Table 2 Demographic, clinical/laboratory characteristics, and outcomes of patients with TSHoma and GDBaseline characteristics of the study populationThe mean age at diagnosis was 41 ± 13.6 years. 12 (75%) patients were females, and 4 (25%) were males.
Clinical features of the study populationEight (50%) patients had palpitations, 7 (43.7%) had goiter and tremors, 6 (37.5%) had weight loss and heat intolerance, 4 (25%) had increased sweating and exophthalmos, 3 (18.7%) had visual field defect, and 1 (6.2%) had a headache at presentation. Eight (50%) patients had co-existing GD and TSHoma at presentation, and 4 (25%) patients had GD diagnosed at initial presentation, followed by the development of TSHoma. 4 (25%) had TSHoma at the initial diagnosis complicated by GD development. In patients diagnosed with GD at first presentation, the mean duration between the development of TSHoma subsequently was 34.75 +/- 16.2 months. Similarly, the mean duration between the development of TSHoma and GD in patients initially presenting with TSHoma was 23 +/- 18.4 months.
Biochemical and radiological data of the included patientsThe median (IQR) initial TSH of the study population was 1.95 (0.12–5.5) mIU/L, the median (IQR) free T3 was11.7 (7.6–19.7) pmol/L, and the median (IQR) free T4 level was 47.6 (33.5–64.4) pmol/L. 10 (76.9%) patients had positive TSH receptor antibody levels, 4 (57.1%) had positive anti-thyroglobulin antibodies, 4 (57.1%) had positive anti-thyroid peroxidase (TPO) antibodies, and 2 (66.6%) had positive thyroid stimulating immunoglobulin (TSI). Three patients had sex hormone binding globulin (SHBG) levels done, and they were raised in all of them. Alpha TSH/TSH ratio was reported in 4 patients, and it was high (> 1) in 3 (75%) patients. A test to assess TSH suppression after octreotide administration was performed in 4 patients and showed TSH suppression in all. Thyrotropin-releasing hormone (TRH) stimulation was reported in eight patients, with abnormal results in 7(87.5%) patients. Of 8 patients with thyroid uptake scans done, diffuse uptake was noted in 7 (87.5%). The mean size of the pituitary tumor was 1.4 ± 0.67 cm. 11 (84.6%) out of 13 cases with reported pituitary tumor size had macroadenoma, and 2 (15.4%) had microadenoma.
Treatment of patients with TSHoma and GDPituitary surgery was performed in 12 (75%) patients. 10 patients had immunostaining for thyrotrophs performed, and it was positive in 8 (80%) patients. At the last follow-up, 4 (25%) patients had complete resolution of symptoms after pituitary surgery, 3 (18.7%) were on maintenance treatment for GD, 1 (6.25%) on beta-blockers and 1 (6.25%) on somatostatin analog.
Subgroup analysis of patients with concomitant TSHoma and GDTable 3 summarizes the characteristics of patients with simultaneous TSHoma and GD at initial presentation. The mean (SD) age at diagnosis was 47.25 +/- 8.6 years. 6 (75%) patients were female. Palpitation, heat intolerance, tremors, and exophthalmos were the most common symptoms (50%), followed by visual field defect (25%) and goiter (25%). Mean (SD) TSH was 4.3 +/- 3.3 mIU/L, median (IQR) free T3 was 19.9 (6.6–19.7) pmol/Land mean (SD) free T4 was 45.5 +/- 13.6 pmol/L. TSH receptor antibody was positive in 6 (85.7%) patients. 7 (87.5%) had macroadenoma and 1 (12.5%) had microadenoma. The mean size of the pituitary tumor was 1.6 +/- 0.8 cm. 2 (25%) patients had complete resolution of symptoms after pituitary surgery, 2 (25%) required maintenance treatment for GD, while 1 (12.5%) required maintenance somatostatin analog treatment.
Table 3 Demographic characteristics, clinical characteristics and outcomes of patients with simultaneous presentation with TSHoma and GD
留言 (0)