
記住我
At the University Hospital of Marburg, from January 2021 to September 2022, 18 patients with refractory CS complicating myocardial infarction were treated with both VA-ECMO and Impella CP left ventricular microaxial pump. In 10 patients, who survived the acute phase of CS, in a stabilized hemodynamic situation, changes in hemodynamics and vascular resistance were documented during different flow settings of biventricular mechanical circulatory support. This was to define the most optimal flow balances of VA-ECMO and Impella (Fig. 1).
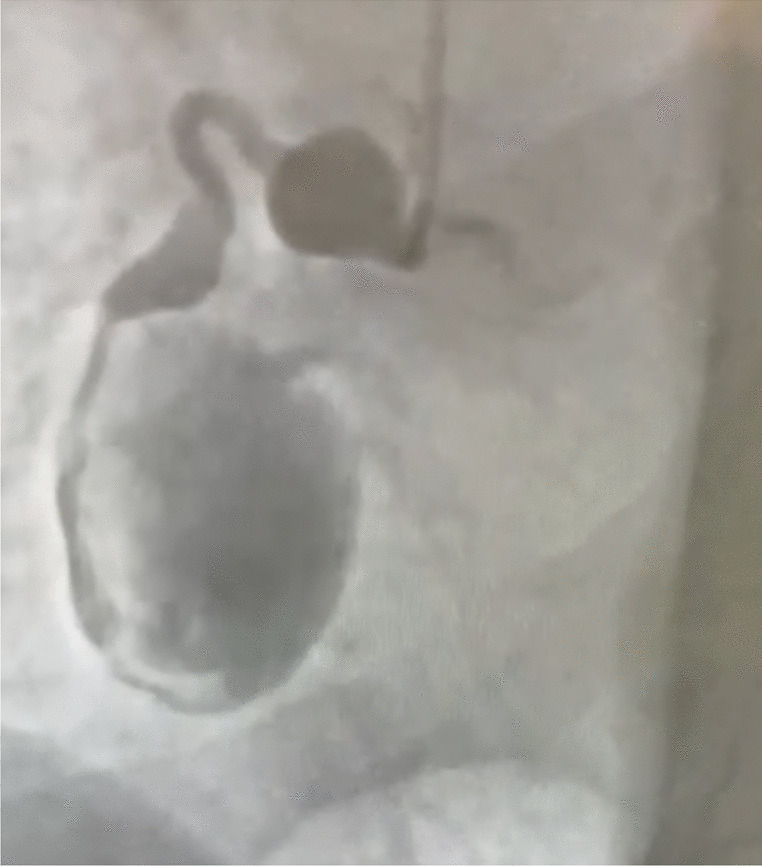
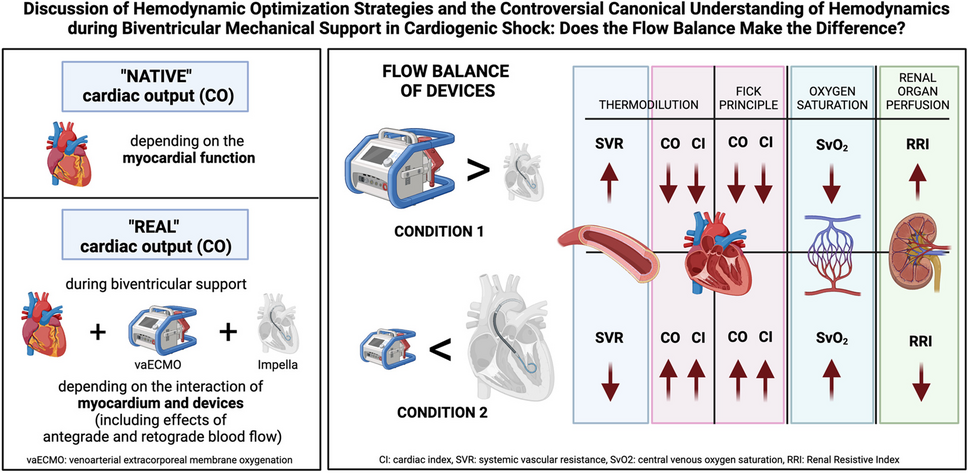
Fig. 1
Measurements of hemodynamic parameters according to a standardized protocol during ECMELLA therapy. The parameters documented for each measurement were the BP, MAP, catecholamine doses, RRI (right/left, 3 times), CI, CO, and SVR. AMI, acute myocardial infarction; BP, blood pressure; CS, cardiogenic shock; CO, cardiac output; CI, cardiac index; MAP, mean arterial pressure; SVR, systemic vascular resistance; RRI, renal resistive index
The presence of CS at the time point of device implantation was defined as systolic blood pressure below 90 mmHg over a period longer than 30 min or the need for vasopressor therapy to maintain systolic blood pressure higher than 90 mmHg. At least one or a combination of the following conditions had to be documented: impaired mental function, oliguria with urine output < 30 ml/h, cold and wet skin, and lactate in blood serum (> 2.0 mmol/l) [15].
In two patients, VA-ECMO was implanted as the first therapeutic strategy due to a mixed hemodynamic and respiratory failure on admission day. In these patients, the Impella was implanted on day 2 of therapy due to a left ventricular dilatation and further worsening of the hemodynamic situation. In another two patients, Impella implantation took place on admission and a day later, the VA-ECMO was implanted due to respiratory and hemodynamic insufficiency. The remaining six patients received the Impella and the VA-ECMO simultaneously. In all patients, a pulmonary artery catheter (PAC) was implanted in the cath lab according to the established shock algorithms.
Invasive hemodynamic parametersDifferent techniques for hemodynamic measurements were used to maintain the most optimal accuracy of the data. To evaluate hemodynamic changes, measurements of cardiac output (CO), cardiac index (CI), and systemic vascular resistance (SVR) first were performed based on the thermodilution principle by invasive pulmonary artery catheterization. To validate the results, CO and CI were additionally calculated by the Fick principle (CO = VO2/AVDO2). VO2 describes the estimated oxygen intake, and AVDO2 is the difference between arterial oxygen concentration and mixed venous oxygen saturation (SvO2). During the measurements which were conducted in a very short period of time (approximately 3 h), no changes of ventilator settings took place including the FiO2. O2 concentration of the VA-ECMO was constantly set at 50% and no significant alterations of paO2 (measured via right radial artery to avoid overestimated O2 measurements due to the “watershed phenomenon” of VA-ECMO support) were documented [16]. VO2 was estimated considering the body surface area (BSA), age, and sex of the patients using the following formulas: VO2-male = BSA × (161 − age × 0.54), VO2-female = BSA × (147.5 − age × 0.47). These formulas for estimating oxygen uptake apply to spontaneously breathing patients. The fact that the O2 concentration (mechanical ventilation and VA-ECMO) and paO2 remained unchanged suggests that the oxygen uptake of the patients also remained without significant changes during the measurements.
It should be emphasized again, that the goal of hemodynamic measurement during biventricular support was not to calculate the “native” CO, but the “real” CO and hemodynamic situation depending on the communication and interaction of the entire system of the patient and the machines.
Mixed venous oxygen saturation (SvO2)To confirm the results of the hemodynamics measurements in the best possible way, SvO2 as a parameter representing cardiac output was taken via pulmonary artery catheterization during each condition of flow change of the devices. SvO2 reflects the balance between global oxygen delivery (DO2) and oxygen consumption (VO2).
Renal resistive index (RRI)The RRI was routinely determined in all CS patients as an established indicator for the occurrence and reversibility of acute kidney injury (AKI) [17,18,19,20]. RRI was determined by intrarenal artery Doppler measurements (peak systolic velocity minus the end-diastolic velocity divided by the peak systolic velocity). Although many concomitant factors like sex, age, diabetes, peripheral and coronary artery disease, and vasculature stiffness as well as the application of vasopressors alter RRI, it correlates with renal vascular resistance and thus renal organ perfusion. RRI values between 0.6 and 0.7 constitute the normal range [21].
An elevated RRI (≥ 0.7) relates to an enhanced risk of acute kidney injury (AKI) and mortality. RRI levels higher than 0.8 are associated with an increased risk of need for renal replacement therapy (RRT) and chronic renal insufficiency in critically ill patients [22,23,24,25]. Our previous data indicate that the Impella improves RRI, indicating improved renal organ perfusion while increasing laminar blood flow [8, 26].
In every patient, the RRI was routinely obtained for both kidneys. RRI values between the left and right kidney showed a mean difference of 0.008 ± 0.01 (p = 0.16). There was no patient with a difference of more than 0.05.
Study protocolAt baseline, before starting the measurements, all the patients showed stable hemodynamics. The MAD was about 87.55 ± 15.85 mmHg in the overall cohort, with accordingly very limited need for vasoconstrictor therapy (norepinephrine). The targeted MAD was between 60 and 70 mmHg.
As depicted in Fig. 1, all patients underwent the following procedure: A first measurement of hemodynamics and vascular resistances, including the RRI, occurred at a baseline output level (BL) of 2.59 ± 0.27 l/min of the VA-ECMO and 2.08 ± 0.32 l/min of the Impella. After 60 min, another “safety measurement” was performed at the same support level of the devices. The therapeutic regime remained without any changes during this period. This was to verify and ensure stable hemodynamics of the patients before variation of the output of the VA-ECMO and Impella took place to individually optimize the therapeutic strategy. Next, the VA-ECMO output was increased by a mean of 0.7 l/min (± 0.18 l/min) and the Impella performance level was reduced by a mean of 0.7 l/min (± 0.21 l/min). Thirty minutes later, the third measurement took place on this support level of the devices (condition 1). The following measurement, 30 min later, was on baseline settings again in order to get back to the starting conditions of the measurements. After that, the VA-ECMO output was decreased by a mean of 0.7 l/min (± 0.23 l/min) below baseline level and the Impella output was enhanced by a mean of 0.7 l/min (± 0.20 l/min) above baseline level (condition 2). Another 30 min later, the fifth measurement took place during this second condition (Fig. 1).
In order to be able to compare the flow settings of the MCS devices as validly as possible, we aimed for an equal variation of the performance levels of Impella and VA-ECMO. As known, the maximum performance of VA-ECMO and Impella is dependent and very often limited by several factors, such as hypovolemia or right ventricular dysfunction. During the protocol, a flow variation of a mean of 0.7 l/min of each, the VA-ECMO and Impella, meaning a total difference of ≈1.4 l/min between the devices could be safely implemented without disturbing the smooth function of both MCS devices. Furthermore, the duration of each flow setting and measurement at the end of each condition with 30 min on steady state was to ensure that hemodynamic changes could occur. The fact that the chosen time period was sufficient could be validated in the context of recurrent baseline measurements, which showed comparable results without significant differences between the measurements.
During the measurements, dosages of catecholamines and fluids, setting of invasive mechanical ventilation (pressure-controlled), and right and left ventricular ejection fraction remained without any changes. Furthermore, the heart rate, the mean arterial pressure, and central venous pressure of the patients did not show any noteworthy alterations while changing the flow levels of the devices.
Clinical data/parametersFurther treatment-relevant variables were documented as follows: respirator parameters of mechanically ventilated patients, volume substitution throughout the measurements, heart rate, arterial blood pressure including systolic, diastolic mean arterial pressure, and catecholamine dosages. In addition, routine blood parameters including GFR and the need for renal replacement therapy (RRT) were registered.
Statistical analysisData were presented as absolute variables and percentages for categorical variables and as mean with ± standard deviation for continuous variables. The Shapiro–Wilk and the Pearson tests were implemented for examining for normal distribution and subsequently, univariate ANOVA was conducted to evaluate for differences among the various conditions. The calculation of intraobserver variability was based on the ICC and its 95% CI.
For visualization, all analyses were performed with SPSS 27 (IBM, New York, NY) and GraphPad Prism 7.0 (GraphPad Software, San Diego, CA). A p-value less than 0.05 was considered statistically significant.
留言 (0)