Pulmonary embolism (PE) is a significant cause of morbidity and mortality worldwide. While national and international guidelines for diagnosing and managing PE have been well-established, implementing a specialized pulmonary embolism response team (PERT) remains a matter of debate [3]. Another example of a specialized disease response team is the heart team with increasing acceptance worldwide for the multidisciplinary management of patients with cardiovascular disease [11]. PERT aims to provide rapid diagnosis and treatment of PE, including advanced imaging, risk stratification, and selection of appropriate therapy. PERT has been shown to reduce mortality rates and hospital length of stay, making it an essential addition to any healthcare system [12, 13]. However, the impact of PERT on the outcome of PE remains unclear due to the fact that prospective studies with clear outcomes are still missing [6, 14].
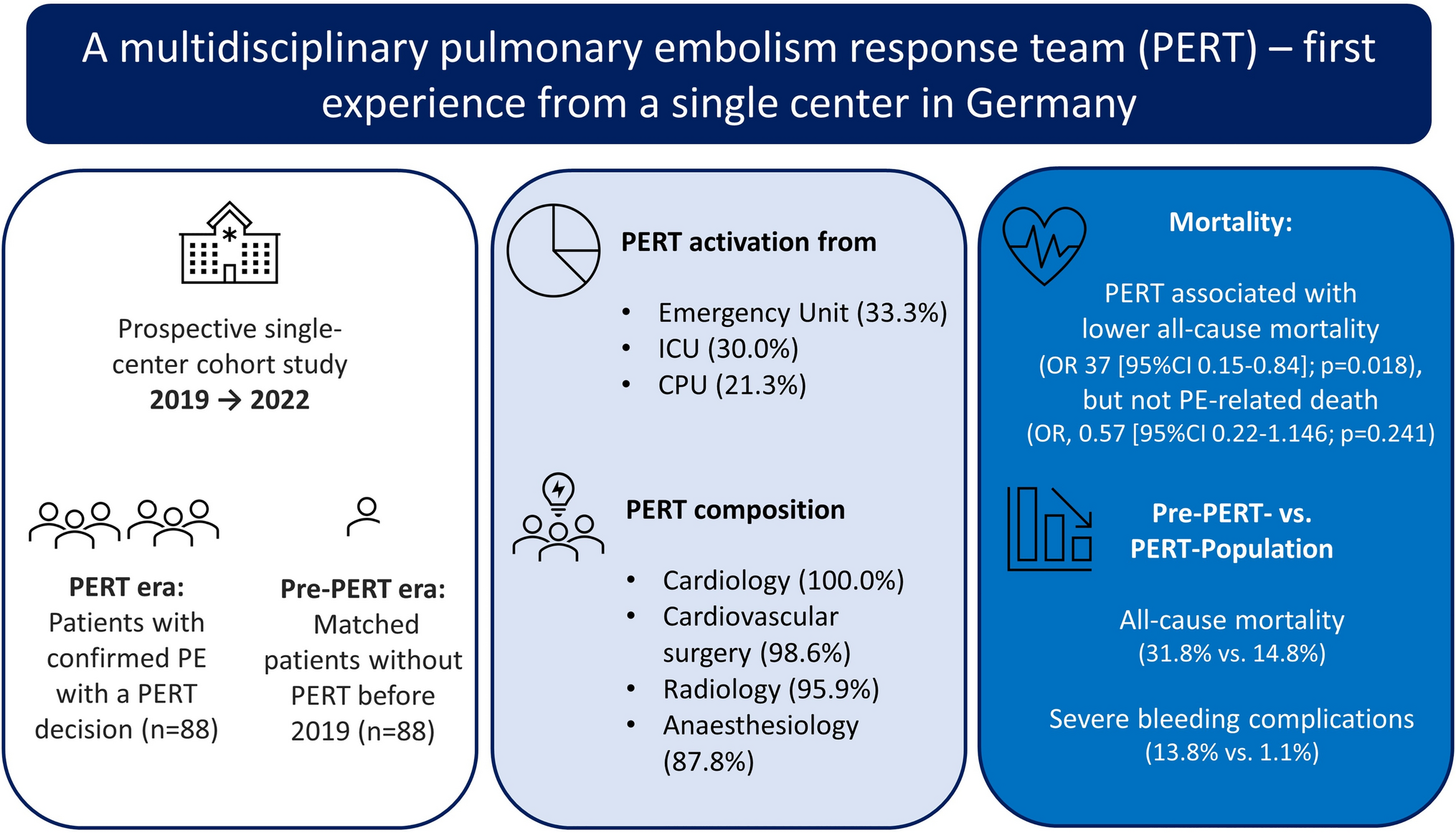
Even if the ESC underlines the importance of set-up, a multidisciplinary team and a program for managing high- and intermediate–high-risk PE with a class IIa recommendation, reports from Europe are only limited to two single-centre experiences from Poland and France [15, 16]. The current study is the first report demonstrating data and knowledge from implementing a PERT in a German center. In line with a recent meta-analysis, the composition of PERT in Germany is equally distributed with cardiologists and cardiac/vascular surgeons in almost all PERT cases, followed by a radiologist and anesthesiologists or intensivist [6]. The commonly applied risk stratifications used in the PERT era showed the expected results. Non-survivors had higher lactate levels, lower hemoglobin, and higher sPESI score and showed more severe ESC algorithm 2019 classes.
When comparing the PERT era with the pre-PERT era at our institution, the most important finding is an overall reduction of in-hospital mortality in the PERT era.
Several explanations for this reduction in mortality can be discussed. The higher incidence of bleeding history in the pre-PERT collective combined with the lower median hemoglobin levels might have influenced the therapeutic decisions made by the attending physicians. Although the major bleeding as a cause of death as well as shock parameters and blood pressure did not differ considerably between both groups, a significant higher rate of catecholamine use in the pre-PERT era was observed. In this context, a trend toward percutaneous thrombectomy and surgical embolectomy could be a possible explanation to avoid thrombolysis associated bleeding complications [17]. In contrast, the rate of CT:RV/LV ratio > 1 was significantly higher in PERT era. The lower rate of embolectomy could be explained by the hypothesis, that in the pre-PERT era, decisions were often made by a single discipline. Thus, the decisions may favor well-known treatment strategies of the single discipline, in which the patient was primary admitted, whereas in a multidisciplinary team, the indication and the type of reperfusion are discussed more intensively.
In the Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry (EMPEROR), 2% of PE overall and 9% of PE with high-risk PE were treated with systemic thrombolysis [18], which is in line with results in our center with 8% of all patients with PE and a PERT protocol. Since PERT is implemented in several countries and hospitals, the overuse of invasive techniques was a main matter of concern [4]. Several single-center studies from the United States found no significant reduction in mortality, but at the same time a trend toward more intensified therapies [19,20,21]. This was not the case in our cohort, more patients in the pre-PERT era received advanced reperfusion therapies as systemic full-dose thrombolysis or surgical embolectomy than patients in the PERT era, which could potentially explain the higher rate of bleeding complications in the pre-PERT era. Additionally, we found that these advanced reperfusion therapies were performed in low-risk and intermediate–low-risk patients with PE significantly more frequently in the pre-PERT era than in the PERT era. Presumably, in a multidisciplinary approach, a team includes endovascular interventionalists, surgeons, and non-invasive physicians, who weigh up advantages and disadvantages and guiding the optimal treatment according to risk stratification evidence. Previously, a single-center study from the United States showed that a dedicated PERT results in the efficient delivery of care and excellent outcomes, which is in line with our findings showing a rapid time to initiate treatment in 25 min after the multidisciplinary discussion [22]. According to the local standard operating procedure, all patients were treated with unfractionated heparin (UFH) during the initial phase. The UFH dosage was given to patient individual and was not recorded in this study. Additionally, the long-term anticoagulation regimes were not part of our study protocol and thus not documented.
A further aspect that must be considered is that our data demonstrated a higher rate of pneumonia and sepsis in patients with acute PE in the pre-PERT era than patients treated in the PERT era. This finding emphasizes that the team approach promotes consensus and provides a unified, reasoned plan for the individual patient, improving efficiency over the traditional practice of independently consulting numerous subspecialty physicians. In this context, although the prognostic value of right ventricular dilation in computed tomography is established to guide risk-adjusted management strategy for acute PE, it is known that additional information about the tricuspid annular plane systolic excursion in echocardiography can identify patients at higher risk for an adverse outcome compared to single parameters of RV enlargement [23]. Before the implementation of PERT in Mainz, only a minority of patients received echocardiography, indicating on the one hand that further aspects of RV dysfunction were not included in the decision-making process, and on the other hand, suggesting that the consultation of a cardiologist has probably not taken place in every case.
The present study has limitations that need consideration: first, our data are limited to a single center including the resources of its electronic medical records. Second, some pre- to post-PERT implementation changes may be partially explained by different cohorts picked from ICD codes, which were tried to balance by propensity score matching. If systemic thrombolysis failed or is contraindicated, alternative reperfusion strategy was recommended with surgical thrombectomy in line with the 2014 ESC guidelines on pulmonary embolism. In the meantime, the 2019 ESC guidelines on pulmonary embolism expand the recommendations toward catheter-directed treatment (CDT) like catheter-based thrombectomy or catheter-directed low-dose thrombolysis as an alternative [7, 8]. Following the paradigm shift, further studies might elucidate the role of CDT in different indications. The role of PERT becomes even more important in relation to technical improvements and updated guidelines regarding CDT strategies. These new technologies offer additional therapeutic options while bringing along their own risk–benefit relations. This should be discussed in a PERT to identify patients with the highest expected benefits and to prevent an intention-to-intervene bias.
In conclusion, implementing PERT was associated with less-invasive therapeutic strategies such as systemic thrombolysis or surgical embolectomy, presumably followed by reduced bleeding complications, and decreased all-cause and PE-related mortality. With its ability to cross disciplines and quickly mobilize resources for decompensating patients, a multidisciplinary team can be seen as crucial for managing patients with complex and higher-risk PE.

留言 (0)