
Remember me






Breast cancer represents the most prevalent malignant neoplasm and remains the foremost cause of mortality associated with cancer in women.1 Breast cancer encompasses 2 primary histological types: the most prevalent form is invasive ductal carcinoma (IDC, accounting for 80% of breast cancers), followed by invasive lobular carcinoma (ILC, accounting for 10%–15% of breast cancers).2,3 In comparison to IDC, ILC exhibits distinct oncological biological characteristics in terms of pathological features, clinical behavior, and metastasis patterns that significantly impact diagnosis and treatment strategies.3–7 The loss of E-cadherin, a cell-cell adhesion molecule, represents the primary characteristic and diagnostic marker for ILCs.8,9 The nonadherent cancer cells in ILCs exhibit augmented migratory and invasive potential as evidenced by their infiltrative diffusion pattern observed within various anatomical sites, including breast tissue, serosal surfaces, meninges, gastrointestinal tract, and ovaries.10,11 Due to distinctive molecular mechanisms and clinical characteristics, ILC poses a greater challenge compared with IDC in imaging detection, which encompasses mammography, ultrasound, MRI, bone scans, and 18F-FDG PET/CT.12–17 Therefore, it is imperative to develop better imaging schemes for the assessment of local infiltration and distant metastasis in ILC.
The receptor expression of ILC and IDC also differs. Compared with IDC (74%), ILC exhibits a consistently high rate of estrogen receptor (ER) positivity (95%),3,11,18 suggesting the potential for improved diagnostic efficacy of ER-targeted PET tracers in ILC patients. 16α-18F-fluoro-17b-fluoroestradiol (18F-FES), a radiolabeled form of estradiol, has recently gained recognition from pharmaceutical regulatory agencies in Europe and the United States as a potent PET probe that enables noninvasive, whole-body evaluation of ER expression in metastatic breast cancer patients.19,20 Several studies have demonstrated the reliability of 18F-FES in detecting ER distribution in breast cancer patients, exhibiting a high concordance between ER status determined by immunohistochemical methods and 18F-FES uptake measured via PET.21–24 Although extensive research has been conducted on the application value of 18F-FES in metastatic breast cancer, the majority of cases primarily involve IDC, leaving limited corresponding studies available for patients with ILC. The retrospective review conducted by Ulaner et al25 on multiple 18F-FES PET/CT prospective trials demonstrated the superior diagnostic efficacy of 18F-FES PET/CT compared with 18F-FDG PET/CT. However, it is important to note that the sample size of this study was extremely limited, including only 7 patients.25 Other case reports suggest that 18F-FES PET/CT can offer clinical decision-making guidance for ILC patients in comparison to conventional radiological imaging or 18F-FDG PET/CT.26 Therefore, the comprehension of the practical application value of 18F-FES PET/CT in ILC remains limited, and there is a lack of conclusive data derived from relatively large-scale cohort studies.
The primary objective of this study was to evaluate and compare the diagnostic performance of 18F-FES and 18F-FDG PET/CT in patients with metastatic ILC. The secondary objective was to evaluate the impact of 18F-FES PET/CT on treatment decision-making in patients with metastatic ILC.
MATERIALS AND METHODS PatientsWe conducted a retrospective screening of patients with metastatic invasive lobular breast cancer who underwent both 18F-FES and 18F-FDG PET/CT scans from 2010 to 2023 at Fudan University Shanghai Cancer Center. The patients were enrolled through one of the following protocols: (1) as a component of clinical trials that employed 18F-FES PET/CT in patients with breast cancer (NCT03507088, NCT04992156, NCT05392985, and NCT05797987); (2) as a diagnostic tool for patients presenting with clinical dilemmas or determining the ER status of metastatic lesions. The additional inclusion criteria were as follows: (1) female patients with ER-positive primary tumors; (2) aged ≥18 years; (3) 18F-FES and 18F-FDG PET/CT scans conducted within 1 month; and (4) no changes in treatment plan between the 2 PET/CT scans. The exclusion criteria were as follows: (1) disease in conjunction with other histological subtypes of breast cancer; (2) coexistence of additional primary malignancies. The study was approved for clinical investigation by the institutional review boards and ethics committee of Fudan University Shanghai Cancer Center in accordance with the Declaration of Helsinki and relevant guidelines. The requirement for obtaining informed consent was waived due to the retrospective nature of the study.
PET/CT ImagingThe synthesis and quality control of 18F-FDG and 18F-FES were conducted at our center, following the procedures outlined in our previous research.27 PET/CT scans were performed on a United Imaging μMI 780 PET/CT scanner (Shanghai, China), a Siemens Biograph 16 HR PET/CT scanner, or an mCT Flow PET/CT scanner (Knoxville, TN). Scans were acquired according to the guidelines of the European Association of Nuclear Medicine, and reconstructions of scans and quantification were performed according to the European Association of Nuclear Medicine Research Limited criteria.28,29
For 18F-FDG PET/CT imaging, patients were instructed to fast for at least 6 hours and maintain blood glucose levels below 10 mmol/L at the time of tracer injection (mean dose, 3.7 MBq/kg). Patients with medical comorbidities, such as diabetes, chronic infections, or chronic inflammatory conditions, were excluded to optimize the sensitivity and specificity of 18F-FDG PET/CT imaging.
For 18F-FES PET/CT imaging, a dose of approximately 222 MBq of intravenous injection of 18F-FES was administered to the patient within a duration of 1–2 minutes.30 Fasting was not needed; however, patients who were treated with ER antagonists required a flushing period of 6–8 weeks, as these drugs impede tracer binding to the ER and may cause false-negative outcomes in 18F-FES PET examination.19,31 Aromatase inhibitors do not require any washing period.
Image InterpretationPET/CT images were independently reviewed and evaluated by 2 board-certified nuclear medicine physicians, each with over 5 years of experience, utilizing a multimodal computer platform (Syngo; Siemens). Reaching a consensus on the final interpretation of statistical analysis was essential in case of disagreement between 2 readers.
Lesions suggested by 18F-FDG or 18F-FES PET needed to be identified and localized through diagnostic CT, MRI, or bone scintigraphy. In the context of visual analysis, PET-positive lesions were defined as exhibiting focal uptake levels that exceeded those of local background activity rather than being attributed to physiological or inflammatory processes. Volumes of interest were delineated around the regions exhibiting positive lesions on PET scans for semiquantitative analysis, with the aim of detecting the SUVmax. Based on our previous studies, an SUVmax ≥1.8 was defined as 18F-FES positive.30
The organ systems affected by the disease, the quantity of lesions in each organ system, and the SUVmax of lesions were documented for both scans. When there were countless bone metastases, they were categorized into 5 regions: the skull, chest (including sternum, scapula, clavicle, and ribs), limb bones, spine, and pelvis. The lesions with the highest 18F-FDG and 18F-FES SUVmax in each of these 5 regions were recorded.
Statistical AnalysisStatistical analysis was performed using SPSS 20.0 software (SPSS Inc., Chicago, IL), and the data are presented as the median and range. To compare the rates of detecting lesions and differences in lesion uptake (SUVmax) between 18F-FES and 18F-FDG PET/CT, the McNemar test and Wilcoxon test were used, respectively. The presence of statistically significant differences was determined when the 2-sided P values were less than 0.05.
RESULTS PatientsWe conducted a retrospective analysis of 63 metastatic ILC patients who underwent 18F-FES PET/CT scans at our center. Twenty-nine patients who did not undergo synchronized 18F-FDG PET/CT scans were excluded from the study. Nine patients were excluded due to the concurrent presence of other histological subtypes of breast cancer, whereas 5 patients were excluded due to the presence of a second primary malignant tumor. A STARD (Standards for Reporting of Diagnostic Accuracy Studies) diagram illustrating patient selection is presented in Figure 1. All 20 patients were women with ER-positive ILC. The patients’ characteristics are shown in Table 1. For all patients, 18F-FDG and 18F-FES PET/CT scans were performed within 1 month. The median time between the 2 scans was 6.5 days (range, 1–30 days).
 FIGURE 1:
FIGURE 1: STARD diagram for patients screened in this study.
TABLE 1 - Patient Demographics and Disease Characteristics Characteristics N = 20 % Age, median (range), y 52 (45–76) Menopausal status Premenopausal 2 10.0 Postmenopausal 18 90.0 Previous treatment lines 0 16 80.0 1 1 5.0 2 2 10.0 ≥3 1 5.0 Prior ET for metastatic disease None 16 80.0 Yes 4 20.0 Prior CT for metastatic disease None 17 85.0 Yes 3 15.0 Therapy type following PET/CT* Endocrine therapy 14 70.0 Chemotherapy 3 15.0 18F-FDG PET All positive 9 45.0 All negative 2 10.0 Mixed 9 45.0 18F-FES PET All positive 12 60.0 All negative 4 20.0 Mixed 4 20.0*Patients were lost to follow-up, and there was no record of treatment plans after PET/CT (N = 3).
All enrolled patients had at least 1 metastasis. The details of these lesions are shown in Table 2. Eight organs or structures were found to be tumor involved in these 20 patients. Among them, bone (80%, 16/20) was the most common site in a patient-based analysis, followed by lymph node (45%, 9/20) and muscle and chest wall (10%, 2/20) metastasis.
TABLE 2 - Disease Involvement: Comparison Between 18F-FDG and 18F-FES Total No. of Patients With Tumor Involvement No. of Lesions Organs/Sites Patient/Lesion 18F-FDG 18F-FES 18F-FDG 18F-FES Lung 1/2 1 1 1 2 Liver 1/1 1 na 1 na Chest wall 2/2 2 1 2 1 Pleura 1/1 1 0 1 0 Muscle 2/5 2 1 5 1 Ovary 1/1 0 1 0 1 Lymph node 9/52 7 5 47 32 Skeletona 16/53 15 13 37 43*The anatomical area involved in skeletal lesions, not the total number of lesions.
na, not available.
Due to diffuse or multiple metastases in bone, these lesions were uncountable and not analyzed in a lesion-based analysis. A total of 65 nonbone metastatic lesions in the other 7 involved organs and structures were detected. Among them, the top 3 common metastases were lymph nodes (80.0%, 52/65), muscle (7.7%, 5/65), and lung and chest wall (3.1%, 2/65).
In the analysis of bone metastasis, a total of 16 patients were identified with bone metastases, distributed in 53 skeletal anatomical regions, with the spine (28.3%, 15/53) and pelvis (26.4%, 14/53) exhibiting the highest prevalence.
18F-FES PET/CTDue to the ER heterogeneity of recurrent/metastatic ILCs, 18F-FES exhibits different manifestations among these patients. Twelve (69.0%, 12/20) patients demonstrated all 18F-FES–avid lesions, 4 (20.0%, 4/20) had 18F-FES–negative lesions only, and the other 4 (20.0%, 4/20) patients had both 18F-FES–avid and 18F-FES–negative lesions. Therefore, approximately half (40%, 8/20) of the recurrent/metastatic ILC patients in our study showed ER heterogeneity, with four of them having received prior treatment for metastatic breast cancer. Conversely, all 12 patients exhibiting 18F-FES–positive lesions were ones in whom recurrence/metastasis was being detected for the first time. A total of 37 18F-FES–avid nonbone lesions were detected, with a median SUVmax value of 5.1 (range, 2.5–15.9). Additionally, 43 skeletal anatomical regions were involved, with a median SUVmax value of 6.3 (range, 1.9–23.1).
18F-FDG PET/CT18F-FDG PET/CT detected all metastatic lesions in 9 (45.0%, 9/20) patients but missed partial lesions in 9 (45.0%, 9/20) patients, and no 18F-FDG–avid metastatic lesions were observed in 2 patients. Hence, the detection rate of 18F-FDG PET/CT was not satisfactory in more than half (55.0%, 11/20) of the patients, with 2 of them having received prior treatment for metastatic breast cancer. A total of 57 nonbone lesions were 18F-FDG–avid, with a median SUVmax of 5.7 (range, 2.6–17.7). Moreover, 37 skeletal anatomical regions were involved, with a median SUVmax value of 6.0 (range, 2.4–13.2).
Comparison of 18F-FES and 18F-FDG PET/CTIn a patient-based analysis, all 20 recurrent/metastatic ILC patients exhibited at least 1 18F-FES or 18F-FDG–avid lesion. 18F-FES and 18F-FDG–avid lesions were detected in 16 and 18 patients, respectively. The detection rate in these 2 scans was not obviously different (P = 0.376).
In 13 patients with nonbone lesions, 18F-FDG detected more lesions than 18F-FES in 5 patients, whereas 18F-FES showed priority in 4 patients (P = 0.637, Fig. 2). In a lesion-based analysis, 18F-FDG detected more nonbone lesions than 18F-FES PET/CT (57 vs 37, P < 0.001). Due to liver physiological uptake, 1 liver lesion was unable to be diagnosed by 18F-FES PET/CT. However, ER heterogeneity was the most common cause of 18F-FES negativity. There was still a significant difference between the 2 scans, even if we excluded liver metastases from the analysis (56 vs 37, P < 0.001). However, the SUVmax values of 18F-FES–avid lesions in nonbone sites were comparable to those of 18F-FDG–avid lesions (6.0 ± 3.1 vs 6.2 ± 3.0, P = 0.437, Fig. 3).
 FIGURE 2:
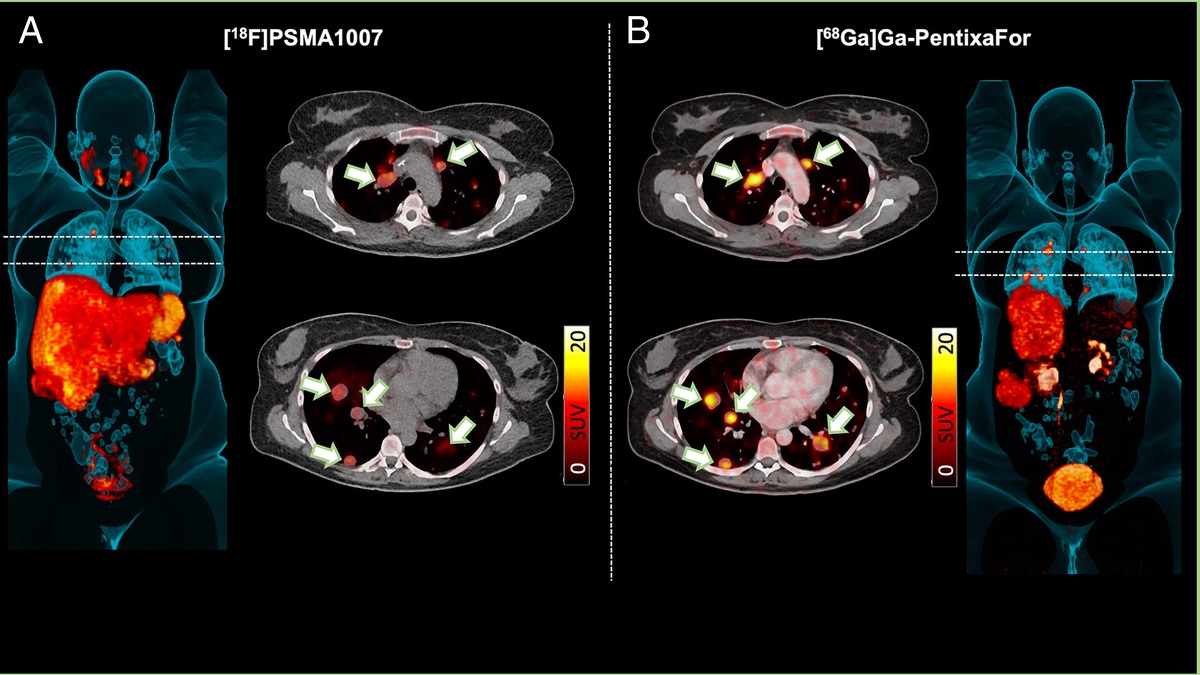
FIGURE 2: Representative 18F-FDG and 18F-FES images of nonbone metastases. A, A 46-y-old woman with ER+/HER2− ILC showed that 18F-FDG was superior to 18F-FES in nonbone metastatic lesions; upper: axial CT, 18F-FDG PET, and fused 18F-FDG PET/CT demonstrating 18F-FDG–avid retroperitoneal lymph node (blue arrow; SUVmax, 11.1); neck, supraclavicular, axillary, mediastinal, abdominal, and pelvic lymph node metastases have also been detected (18F-FDG PET MIP); below: axial CT, 18F-FES PET, and fused 18F-FES PET/CT demonstrating non–18F-FES–avid retroperitoneal lymph node (white arrow), and 18F-FES PET MIP image did not shown any positive lesions. B, A 58-y-old woman with ER+/HER2- ILC showed that 18F-FES was superior to 18F-FDG in nonbone metastatic lesions; upper: axial CT, 18F-FDG PET, and fused 18F-FDG PET/CT demonstrating non–18F-FDG–avid left ovarian metastasis (yellow arrow); below: axial CT, 18F-FES PET, and fused 18F-FES PET/CT demonstrating 18F-FES–avid left ovarian metastasis (red arrow; SUVmax, 9.3).
 FIGURE 3:
FIGURE 3: Quantitative analysis was performed to compare 18F-FDG and 18F-FES PET in nonbone and bone lesions (mean ± SD). BL, bone lesions; N-BL, nonbone lesions.
Given that bone was the most common site of metastasis, we conducted a comprehensive analysis focusing on this aspect. Among the 16 patients with bone metastasis, 10 individuals (62.5%, 10/16) showed all 18F-FES–avid lesions, whereas 3 patients (18.75%, 3/16) demonstrated complete absence of 18F-FES uptake, and the other 3 patients (18.75%, 3/16) presented 18F-FES heterogeneity. Six patients showed bone metastases with all 18F-FDG–avid, 9 patients had both 18F-FDG–avid and nonavid bone metastases, and the other 1 patient displayed diffuse osteogenic metastases, all of which were 18F-FDG nonavid. The SUVmax values of 18F-FES–avid bone lesions in the skeleton regions exhibited relatively higher levels than those of 18F-FDG–avid lesions (8.3 ± 5.7 vs 6.7 ± 2.4, Fig. 3). However, no statistically significant difference was observed (P = 0.881).
In a patient-based analysis, 18F-FES PET/CT detection demonstrated superiority in 9 cases, whereas 18F-FDG PET/CT was advantageous in 4 cases (P = 0.050, Fig. 4). In a regional analysis of bone metastasis, a total of 53 skeleton regions were tumor involved (spine 15, pelvis 14, thoracic cage 10, skull 8, limb 6). Among them, 18F-FES detected 43 involved regions (spine 11, pelvis 12, thoracic cage 8, skull 7, limb 5), whereas 18F-FDG found 37 involved regions (spine 12, pelvis 12, thoracic cage 7, skull 1, limb 5). Interestingly, 18F-FES PET/CT showed remarkable superiority in detecting skull lesions (7 vs 1, P = 0.003), whereas the results of the 2 scans in other regions were comparable (P > 0.05).
 FIGURE 4:
FIGURE 4: Representative 18F-FDG and 18F-FES PET/CT images of bone metastases. A, Nine ILC patients showed that 18F-FES exhibited superior performance compared with 18F-FDG in bone metastatic lesions (red arrow). B. Four ILC patients showed that 18F-FDG was superior to 18F-FES in bone metastatic lesions (blue arrow).
Impact of 18F-FES PET/CT on Treatment ChoiceThe treatment choices for 17 patients were analyzed, excluding 3 patients who did not seek medical attention at our center after their PET/CT scans. The systematic treatment types after PET/CT are presented in Table 3. As subsequent treatment, all 12 patients (100%) with only 18F-FES–positive lesions were administered either endocrine therapy or a combination therapy involving CDK4/6 inhibitors. Among the patients, 2 exhibited both positive and negative lesions for 18F-FES, one underwent either endocrine therapy or a combination therapy involving CDK4/6 inhibitors, and the other received chemotherapy alone. Among the 3 18F-FES–negative patients, 2 underwent chemotherapy, whereas one presented with bone oligometastasis and received endocrine therapy with radiation therapy for the management of bone lesions. Relevant treatment plans for all patients prior to and subsequent to PET/CT scanning can be reviewed in the Supplementary Table (https://links.lww.com/CNM/A458).
TABLE 3 - Subsequent Systemic Treatments After 18F-FES PET/CT Types of Treatment FES + (n = 12) FES +/− (n = 2) FES − (n = 3) Endocrine therapy 12 (100%) 1 (50.0%) 1 (33.3%) Chemotherapy 0 1 (50.0%) 2 (66.7%)Values are n with percentage in parentheses.
The utilization of PET with 18F-FDG has been demonstrated to hold significant value in the systemic staging of patients afflicted with advanced or metastatic breast cancer.32,33 However, it is sometimes perceived that the diagnostic efficacy of 18F-FDG in ILC may be inferior to that in IDC.16,34 The low affinity of ILC for 18F-FDG may be attributed to factors such as the relatively sparse cell density, absence of tumor-infiltrating lymphocytes, or lack of Glut-1 transporter expression in ILC.16,18,35 In comparison to IDC, ILC displays a higher proportion of hormone receptor expression, particularly with its nearly universal (95%) ER positivity. This enhances the potential utility of ER-targeted PET (18F-FES) tracers in ILC patients. Several studies have demonstrated the superior performance of PET/CT with 18F-FES compared with 18F-FDG in patients with ILC.25,26,36
Ulaner et al25 conducted a retrospective evaluation of metastatic breast cancer patients enrolled in 6 prospective trials at the Memorial Sloan Kettering Cancer Center. Among these patients, 7 with ILC underwent both 18F-FES PET/CT and 18F-FDG PET/CT within a 5-week period and were included in the retrospective analysis. The 18F-FES PET/CT scan detected a total of 254 lesions, whereas the 18F-FDG PET/CT scan identified 111 lesions. In 5 out of 7 patients, 18F-FES PET/CT demonstrated superior lesion detection capabilities and exhibited a more favorable tumor-to-background ratio. However, this study is not without limitations. First, the sample size was relatively small, comprising only 7 patients with ILC. Second, the detection of metastatic lesions was confined to skeletal sites. Although both IDC and ILC commonly metastasize to the bones, lymph nodes, and liver, there is no significant difference in the extent of bone involvement between ILC and IDC.37 The infiltrative spread patterns of ILC make it more likely to metastasize to the peritoneum, retroperitoneum, hollow viscera (including the gastrointestinal and urogenital tracts), and pia mater compared with IDC.5,38,39
In our retrospective analysis, we evaluated and compared the diagnostic performance of 18F-FES and 18F-FDG PET/CT in a cohort of 20 patients with metastatic ILC. To the best of our knowledge, this study represents the largest investigation of its kind concerning ILCs. Our analysis encompassed not only bone metastases but also infiltrating soft tissue metastases involving the lymph nodes, chest wall, pleura, muscles, lungs, liver, and ovaries. The skeleton is the primary site for metastasis in breast cancer, with a high prevalence. However, 18F-FDG PET/CT tends to underestimate the presence of osteogenic bone metastasis. In our study, we identified 16 cases of bone metastasis, with 9 demonstrating superior diagnostic advantages of 18F-FES PET/CT and 4 exhibiting superiority of 18F-FDG PET/CT, consistent with the findings reported by Ulaner et al.25 Furthermore, 18F-FES PET/CT exhibits superior diagnostic efficacy for skull metastasis compared with 18F-FDG PET/CT (7 vs 1), potentially due to the high physiological uptake of 18F-FDG in the brain, which can obscure diagnosis of the skull. However, it is disappointing that when assessed in terms of patient cohorts (13 vs 15) or anatomical regions (43 vs 37), 18F-FES PET/CT did not demonstrate significant superiority in the diagnostic accuracy for detecting bone metastases compared with 18F-FDG PET/CT. In contrast, 18F-FDG PET/CT was superior to 18F-FES PET/CT in the assessment of nonbone lesions based on lesion analysis (57 vs 37, P < 0.001), whereas no significant difference was observed between the 2 techniques in patient-based statistics. As widely acknowledged, the primary limitation of 18F-FES PET/CT lies in its inability to detect liver lesions due to the physiological excretion of 18F-FES through the hepatobiliary system. Even after excluding 1 liver metastasis, PET/CT continued to outperform 18F-FES PET/CT in detecting the number of nonbone lesions. In fact, given the potential for ER-positive primary breast cancer patients to transition into ER-negative metastatic lesions,4,40 it is unsurprising that 18F-FDG PET/CT examination outperformed 18F-FES PET/CT examination in detecting the extent of organ involvement per patient.40 It is noteworthy that among the 8 patients exhibiting heterogeneous uptake or all negative 18F-FES PET/CT scans, half (50.0%, 4/8) of the patients had received systemic treatment for metastatic lesions (data not shown; refer to the Supplementary Table, https://links.lww.com/CNM/A458). In their subgroup analysis of patients with metastatic lobular carcinoma who had not received systematic treatment, Bottoni et al demonstrated that 18FES PET/CT provided a better diagnostic advantage for lymph node and bone metastasis than 18F-FDG PET/CT.20 Therefore, when utilizing 18F-FES PET/CT for the diagnosis of metastatic ILC, it is imperative to consider the alterations in ER status induced by systemic therapy, and the concurrent utilization of 18F-FDG PET/CT can enhance the diagnostic efficacy within this patient cohort.
Although the diagnostic efficacy of 18F-FES PET/CT may not necessarily surpass that of 18F-FDG PET/CT, it can still offer valuable insights into the status of ER, thereby serving as a useful reference for subsequent treatment decisions in patients. In the subsequent treatments, our retrospective review revealed that patients with only 18F-FES–positive lesions fully received endocrine therapy–based regimens, whereas the majority of patients with only 18F-FES–negative lesions were administered chemotherapy. The proportion of patients with 18F-FES heterogeneity who received endocrine therapy or chemotherapy was essentially equivalent. Therefore, in comparison to conventional radiological imaging and 18F-FDG PET, 18F-FES PET not only serves as a valuable tool for disease detection but also effectively reflects the ER status of the lesion, thereby providing crucial guidance for clinical decision-making and subsequent treatment strategies.27,41,42
Our study has several limitations. First, the sample size in this study is relatively small, and there exists a certain degree of heterogeneity in terms of disease characteristics, except for primary ILCs with ER positivity. Given the relative rarity of ILC as a subtype of breast cancer and the limited accessibility to both 18F-FES and 18F-FDG dual PET imaging in the same patient, our analysis is constrained by a restricted number of available patients. Nevertheless, it is worth noting that this research group represents the largest cohort in this specific field to date. The second limitation of this study is that the research samples were exclusively obtained from a single institution, and the study population consisted solely of individuals from an Asian background. It should be acknowledged that the disease characteristics of ILC may exhibit variations across different ethnic groups.43 Third, we assessed the involvement of specific anatomical regions within the bone rather than quantifying the total number of bone metastases. Given that 18F-FES PET/CT exhibits superior sensitivity in detecting bone metastases compared with 18F-FDG PET/CT,20,44 evaluating the skeletal distribution of segments may underestimate the detection capability of 18F-FES PET/CT for identifying the burden of bone metastasis. However, it is important to note that with the exception of oligometastasis and symptomatic metastases, the number of detected bone lesions does not substantially impact patient treatment management. Moreover, it should be acknowledged that biases may exist in the overall statistical approach to metastatic bone lesions. In this regard, aggregating bone anatomical segments with bone lesions offers a more convenient and reproducible approach.45 Finally, histopathological confirmation was not obtained for all patients diagnosed with metastatic recurrence, and it cannot be ensured that every lesion exhibiting high PET uptake was indeed a metastatic lesion. However, in our retrospective review, it was determined through additional conventional imaging modalities and clinical follow-up that the findings obtained from 18F-FES and 18F-FDG PET/CT scans represented characteristic manifestations of metastatic diseases.
CONCLUSIONSIn conclusion, our research findings demonstrate the clinical utility and reliability of 18F-FES PET/CT scanning in the detection of ILC recurrence and metastasis, particularly in challenging lesions such as osteogenic and skull metastases that exhibit limited detectability or low 18F-FDG affinity. However, the detection of nonbone lesions is comparable to or exhibits certain limitations in comparison with 18F-FDG PET/CT. Considering the potential alterations in ER status among patients with metastatic ILC, the combined utilization of 18F-FES and 18F-FDG PET/CT imaging modalities may be deemed the preferred option for assessing these individuals. Furthermore, the findings of 18F-FES effectively demonstrate the expression of ER in the lesions, thereby offering potential guidance for treatment decision-making in patients with metastatic breast cancer.
REFERENCES 1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. 2. Desmedt C, Zoppoli G, Gundem G, et al. Genomic characterization of primary invasive lobular breast cancer. J Clin Oncol. 2016;34:1872–1881. 3. McCart Reed AE, Kutasovic JR, Lakhani SR, et al. Invasive lobular carcinoma of the breast: morphology, biomarkers and 'omics. Breast Cancer Res. 2015;17:12. 4. Trillo P, Sandoval J, Trapani D, et al. Evolution of biological features of invasive lobular breast cancer: comparison between primary tumour and metastases. Eur J Cancer. 2023;185:119–130. 5. Inoue M, Nakagomi H, Nakada H, et al. Specific sites of metastases in invasive lobular carcinoma: a retrospective cohort study of metastatic breast cancer. Breast Cancer. 2017;24:667–672. 6. Zengel B, Yararbas U, Duran A, et al. Comparison of the clinicopathological features of invasi
Comments (0)