This study qualitatively evaluated the acceptability and effectiveness of a breast cancer RT video designed to educate and facilitate informed consent during the initial RO consultation. The video modality provides an approach to standardising depth and quality of the plethora of information that EBC patients encounter. Reception was largely positive with regard to ease of engagement with the video, its ability to improve understanding of RT and increase feelings of preparedness. The multi-modal incorporation of visual, auditory and written stimuli within the video appealed to participants, allowing the portrayal of abstract concepts such as radiation. To accommodate the low health literacy noted in 60% of Australian adults, the video was tailored to an eighth-grade level [17]. The video also balanced comprehensiveness and succinctness, with its duration within the typical range documented in the literature of 16–25 min, and being shorter than the standard RO verbal consultation of up to 40 min, amongst the practice of the RO authors.
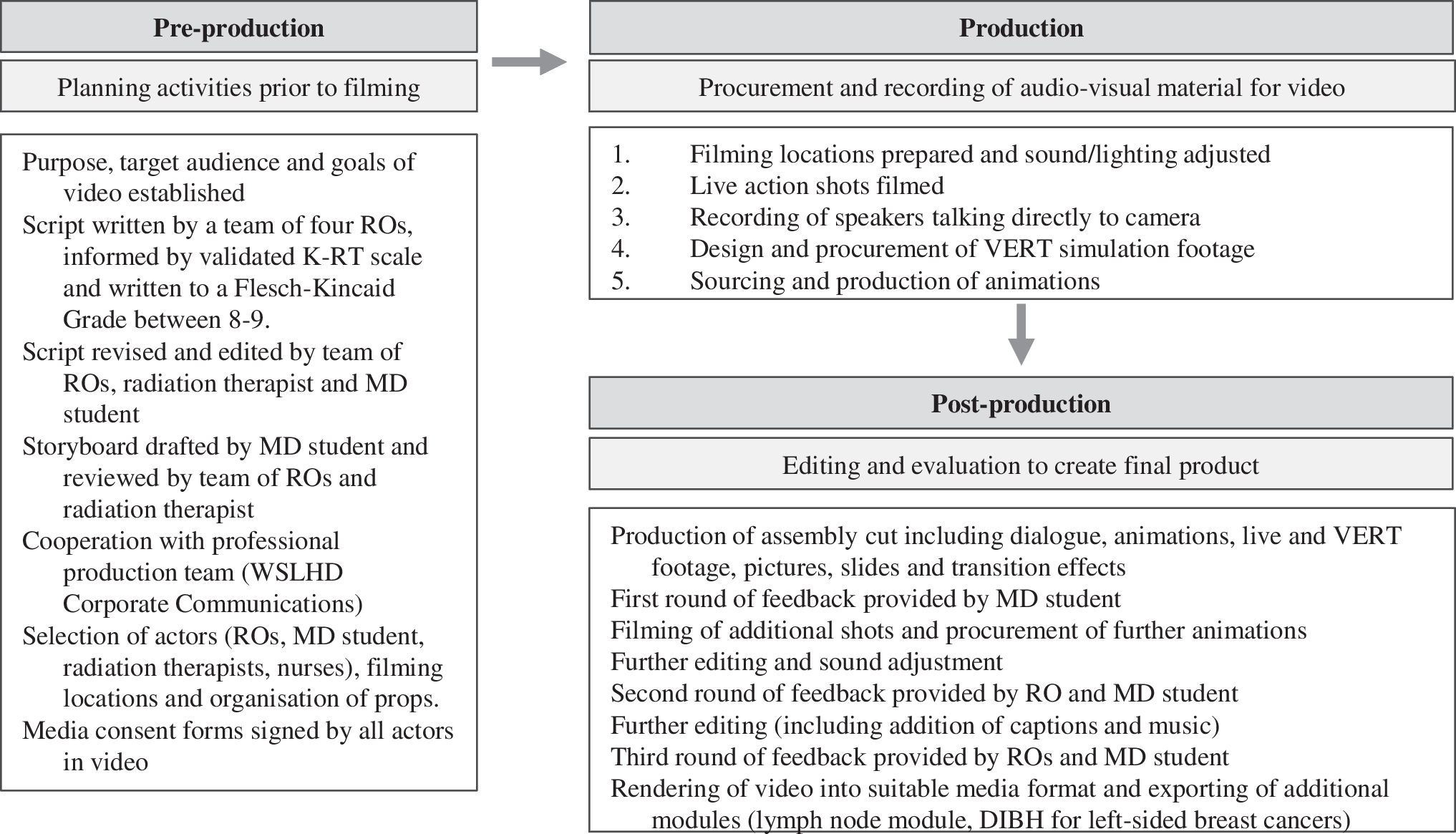
The positive reception to this video is consistent with the growing body of evidence supporting video education in breast cancer RT education literature. Several recent studies have demonstrated educational videos to be a superior form of breast cancer RT education, leading to substantial improvements in patient self-reported knowledge [7, 8, 13], post-consult anxiety [7, 8, 13, 14], heightened confidence in providers [7] and better decision-making [7]. However, of these studies, only one single-arm study of 20 participants targeted the initial RO consult and reported the 7.5-min video to be a feasible intervention that decreased patient-reported anxiety [14]. Our study is the first to incorporate VERT simulations into a breast cancer RT educational video that is intended to be viewed by patients during an initial RO consultation. VERT-based education sessions have reliably demonstrated improvement of RT knowledge in EBC patients [18].
Although the majority of feedback was positive in nature, the discussions generated several insightful suggestions prompting the team to consider minor enhancements to optimise the video. These include subtitling the video to improve understandability, translating versions, and creating alternative versions with accessibility information for other WSLHD hospitals. Other suggestions were difficult to action, such as addressing the effect of COVID-19 on RT treatment despite being valid and pertinent, as policies and procedures are frequently changing. As such, it would be optimal to seek specific advice based on contemporary local policy. Similarly, patient-specific questions on follow-up imaging after RT completion or statistical recurrence risk data would be better suited to discussion with the RO after viewing the video.
There were challenges and limitations encountered in this study, some of which are inherent to focus group methodology. One potential limitation is that of volunteer bias, wherein volunteers may be systematically different to the general breast cancer population [19]. This may have further been compounded by the inclusion criteria for English proficiency. However, this study captured women across a range of ages, educational levels and linguistic backgrounds. Similarly, the phenomenon of group bias arises in focus groups, wherein participants may opt to maintain group consensus rather than present their true opinion. Overall, the focus group methodology was conducive to the aim of gathering preliminary feedback on the newly created video. Although a face-to-face format would have been preferred due to non-verbal communication and visual cues [20], Zoom emerged as a non-inferior alternative during COVID-19 [21]. The pandemic also saw delays in participant recruitment, which limited this study to three focus groups. The smaller groups not only facilitated equal discussion opportunities among participants, but are substantiated by previous work demonstrating 80% of discussion themes are discoverable within two to three focus groups [22]. Another challenge was creating a video specific enough to educate and answer patient questions but general enough to maintain relevance to most patients. Hence, two additional video modules were created to be integrated into the core video for specific patient groups with lymph node involvement or left-sided cancers.
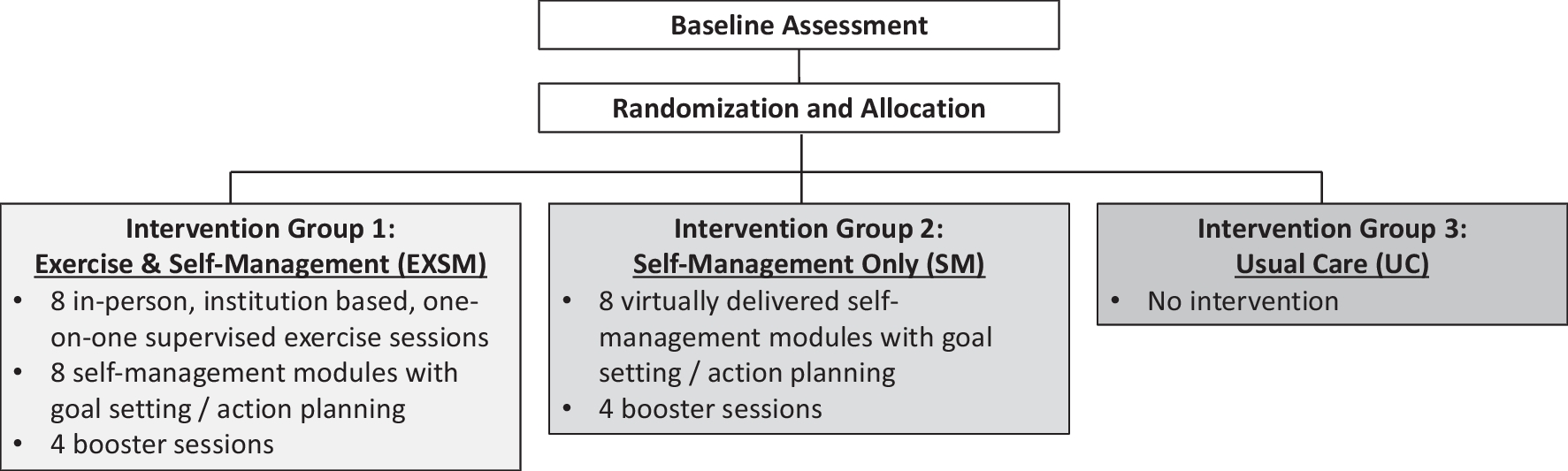
In the future, the video will be further evaluated within an ethics-approved biphasic quasi-experimental pilot trial. The trial will assess knowledge of RT and evaluate levels of anxiety and distress in EBC patients, who will receive at the initial RO consultation either standard education, or have part of the standard education replaced by this video in addition to the residual standard education and individual patient-specific information. If benefit from video education is demonstrated in the pilot trial over standard practice, this research has the potential to enhance standard EBC RT education at the initial RO consultation. Multimedia-based interventions are cost-effective [23], time-efficient [24] and allow the delivery of high-quality education remotely. Further efforts will be required to extend the generalisability of this video to include patients from culturally and linguistically diverse backgrounds, and other health areas.


留言 (0)