The existing literature extensively covers the various impacts of ionizing radiation such as DNA damage, malignancy, cataracts, dermatologic changes, and delayed wound healing [2,3,4,5,6, 21]. Despite this research evidence, there remains a significant gap in our understanding of the full health effects of chronic low-level radiation exposure [7, 8]. One area of specific concern is the potential damage to the hands of surgeons due to prolonged exposure to significant doses of ionizing radiation during procedures involving fluoroscopic-guided imaging. Urologists, who frequently use fluoroscopy to perform essential procedures, are particularly at risk for repeated low-level radiation exposure. Consequently, it becomes imperative to acknowledge the potential harm associated with all levels of ionizing radiation and take every possible protective measure to reduce exposure to as low as reasonably achievable (ALARA) [22]. In addition to posing a significant risk of joint, vascular, and skin pathologies, any adverse effects on a surgeon’s hand can significantly impact their ability to provide effective care and perform surgical procedures safely. To address these concerns and minimize potential harm, the ICRP guidelines suggest not exceeding 20 mSv of average radiation exposure per year over a 5-year period and an annual limit of 50 mSv. Additionally, the ICRP advises maintaining an annual radiation dose limit of 500 mSv to the skin and extremities [19].
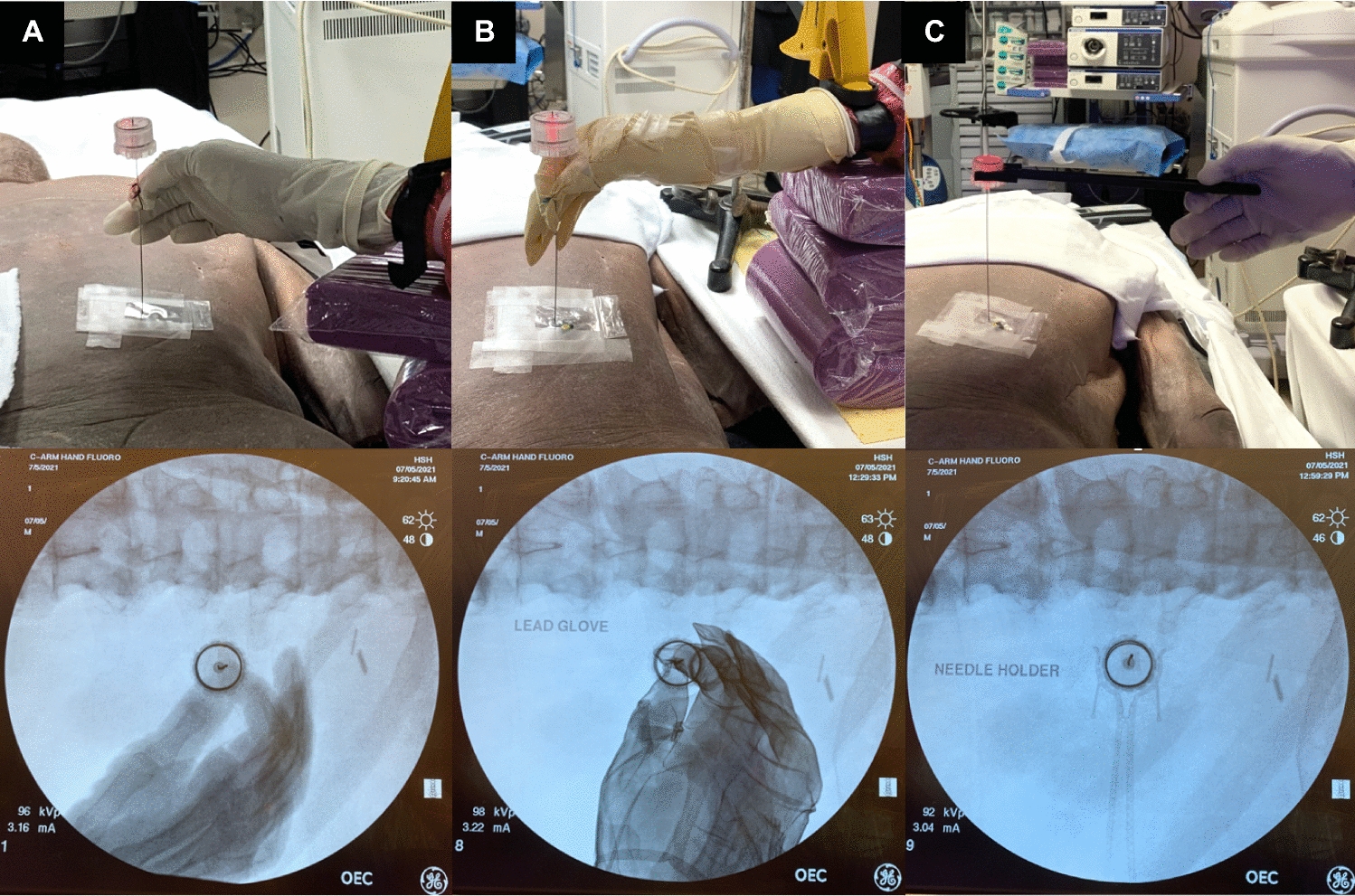
Our study aimed to investigate the efficacy of radiation-attenuating gloves and a novel needle-holder in reducing ionizing radiation exposure to the surgeon’s hands during urological procedures. Using a cadaver model, we evaluated different techniques to reduce radiation exposure during simulated percutaneous renal access and observed significant exposure reductions to the surgeon’s hand. The use of a radiation-attenuating glove resulted in a 37% reduction, while employing a needle holder led to a 65% reduction in the mean equivalent dose to the surgeon’s hand (Table 1). The 37% radiation reduction for the radiation-attenuating glove at 95.2 kVp is comparable to the manufacturer specifications of 33% reduction at 100 kVp [20]. The decreased radiation dose associated with the radiation-attenuating glove may be attributed to the material’s high attenuation coefficient which reduces penetrating radiation. Similar reductions in exposure have been reported in orthopedics, where radiation-attenuating gloves were found to decrease exposure by 61% in an anthropomorphic model [21]. However, it is worth noting that their study used a mini-C arm with lower kVp and mA settings, unlike the GE OEC 9900 system at AEC settings used in our research. On the other hand, the needle holder further reduced exposure, likely by enabling the surgeon to remove their hand from the direct radiation beam. Notably, there is currently a lack of studies investigating the radiation-reducing effects of a needle holder during percutaneous renal access.
Simulated PCNL access demonstrated a mean radiation dose of 3.92 mSv to the hand without protection. Recent studies have reported similar hand radiation exposure during PCNL of 0.36–4.36 mSv [9, 23]. This wide range of hand exposure could be attributed to variations in fluoroscopy use, settings, and surgeon experience. Using the ICRP guidelines, approximately 127 PCNLs may be performed annually using surgical gloves without exceeding the dose limit for extremities. This number increases to 201 with radiation-attenuating gloves and 364 with the needle holder.
Custom-made needle holders have been specifically designed for the conventional “bullseye” technique in percutaneous renal access [24, 25]. As demonstrated in our study, these needle holders can potentially reduce radiation exposure to both the surgeon's hand and patient when constructed from a low radiation density material. However, literature on specialized needle holders for PCNL access is sparse. In contrast, the practice of utilizing needle holders has been extensively studied and more commonly employed in fields that frequently rely on fluoroscopic-guided imaging, such as interventional radiology. Studies investigating the use of improvised metal and custom-made plastic needle holders during fluoroscopic-guided interventions demonstrated significantly reduced radiation exposure to the user’s hand [26, 27]. In the field of endourology, the utilization of specialized needle holders is not yet widespread, requiring further research to determine their efficacy and safety.
Considerable research has been dedicated to reducing radiation exposure during fluoroscopic procedures in the operating room [1]. Implementation of simple yet effective measures, such as appropriate shielding, can lead to a significant reduction of up to 70-fold in radiation exposure [1]. Similarly, operating the fluoroscopy machine at lower power settings is another effective strategy [1]. However, adoption of these practices is not universal. A survey among endourologists revealed that lead aprons were worn in 99.3% of cases, thyroid shields in 98.7%, and radiation-attenuating gloves in only 9.7% [28]. The underuse of radiation-attenuating gloves is most likely multifactorial in nature, potentially due to cost, unacquaintance, inconvenience, or believing further protection is unnecessary due to current occupational dose limit guidelines. For fluoroscopy settings, the AEC setting remains the most commonly used mode due to its ability to obtain optimal quality images [29]. However, low dose modes and pulsed fluoroscopy are sufficient for many procedures [1].
The radiation reduction techniques explored in this study had implications not only for the surgeon but also for the patient. While the use of a radiation-attenuating glove reduced radiation exposure to the surgeon's hand by 37%, it resulted in a 3% increase in dose to the patient's dorsal surface (Table 1). In contrast, utilizing the needle holder reduced exposure for both the surgeon's hand by 65% and the patient's dorsal surface by 14%. The use of radiation-attenuating gloves may offer protection for the surgeon, but at the cost of increasing the dose to the patient. This is likely due to the effect of introducing hyperdense objects, such as radiation-attenuating gloves, into the path of the fluoroscopy beam. This has been shown to increase the radiation produced by the machine when it is operating in the AEC setting [14]. On the other hand, the needle holder is made from a low-density material and has a slim contour, which may have allowed the fluoroscopy machine to generate a lower radiation dose. This is supported by the findings regarding radiation dose, kVp, and mAs generated by the fluoroscopy machine in our study, which were found to be higher for the radiation-attenuating glove compared to the needle holder (Table 3).
Limitations of our study include the use of a cadaver model for simulated percutaneous renal access which cannot entirely replicate all aspects of the working environment encountered in a live PCNL. Nonetheless, this approach provided a controlled testing environment that allowed for accurate comparisons of radiation reduction techniques without resultant undue radiation exposure to human subjects. An additional limitation of our study is that it was designed to compare three different methods of holding the needle during fluoroscopic-guided access and did not include a comparison of ultrasound-guided access. We also used the AEC setting and a preset fluoroscopy time for simulated renal access. While the AEC setting is the most commonly used fluoroscopy setting, low-dose settings and pulsed fluoroscopy are also used in practice [1, 29]. The preset fluoroscopy time of 5 min in our study will not be representative of all practices and institutions. Finally, it is important to note that this needle holder and radiation-attenuating glove were only tested in a prone PCNL model, where the surgeon’s hand receives direct radiation exposure. In triangulation and supine PCNL the surgeon’s hand is less likely to encounter direct radiation exposure, and subsequently, these were not tested in our model. Despite these limitations, to our knowledge, this is the first study to assess and compare hand radiation reduction techniques during percutaneous renal access for PCNL in a controlled cadaver model.

留言 (0)