This study was a single-institution review of outcomes from manual cold capping. The majority (65–80% or more) of those who undergo chemotherapy can expect some degree of chemotherapy-induced alopecia (CIA) [1,2,3]. Chemotherapy attacks rapidly dividing cells in the body, including the hair follicles [4]. CIA is often ranked among the most distressing side effects, with potentially significant impact on quality of life and overall wellness during the cancer journey [5, 6]. Some patients have refused chemotherapy because of the CIA [7, 8]. Many methods to save hair have been tested, but scalp cooling has been the most effective in reducing CIA [7]. Scalp cooling is a non-medicinal approach to minimize CIA, whereby ice packs or cooling caps are placed on the scalp for up to an hour before, during, and up to 7 h after each chemotherapy session, depending on the chemotherapy regimen and cooling system [9]. The cold results in local vasoconstriction, which potentially minimizes the amount of cytotoxic drug that reaches the cells of the hair follicles [9, 10].
Scalp cooling has been shown to prevent or minimize CIA with generally mild side effects, although the effectiveness may vary depending on myriad factors including application system, patient-level factors, and assessment tools used [11,12,13,14,15,16,17]. Commercially available scalp cooling systems in the USA include machine-based systems such as Paxman Scalp Cooling system [18] and the DigniCap system [19] or manual systems such as Arctic Caps [20], Chemo Cold Caps [21], and Penguin [10]. In machine-based systems, the caps are attached to a dedicated refrigeration system and one or two patients can be independently treated at a time, with cooling times of 30 min prior to infusion, during the infusion and up to 90–120 min following infusion [18, 19].
For manual cold capping systems, patients rent or buy a set of caps that are frozen in a biofreezer at the infusion center or in personal freezers using dry ice [22]. Because the caps are not connected to a cooling system, they must be changed periodically; however, patients also have increased freedom/mobility compared to machine-based systems, given that post-infusion capping lasts for up to 7 h [22]. Given the potential benefits of manual capping, we explored manual options for use at our institution and selected Penguin Cold Caps, London, UK. Penguin Caps contain a proprietary gel that maintains cold temperatures for long periods of time and do not require connection to refrigeration systems [10]. As such, patients use a set of three caps and do not have to change the caps as frequently during a session [10]. For our institutional cold capping protocol, all patients start wearing the cold cap 50 min prior to starting each chemotherapy infusion and continue to wear the cap for the entirety of each infusion. Caps are not worn between infusions. The length of time that the patient wears the cold cap after the end of each chemotherapy infusion session ranges from 3 to 7 h, depending on the chemotherapy regimen. This 3–7-h range is in contrast to machine-based capping protocols, which have post-infusion cooling times of 90–120 min. The post-infusion cooling time for manual systems may be substantially longer than machine-based systems. However, the patients continue the cold capping at home once the chemotherapy is complete, which has benefits of freeing chair space in the infusion center, keeping patients in the infusion center for less time, and allowing more patients to utilize cold capping.
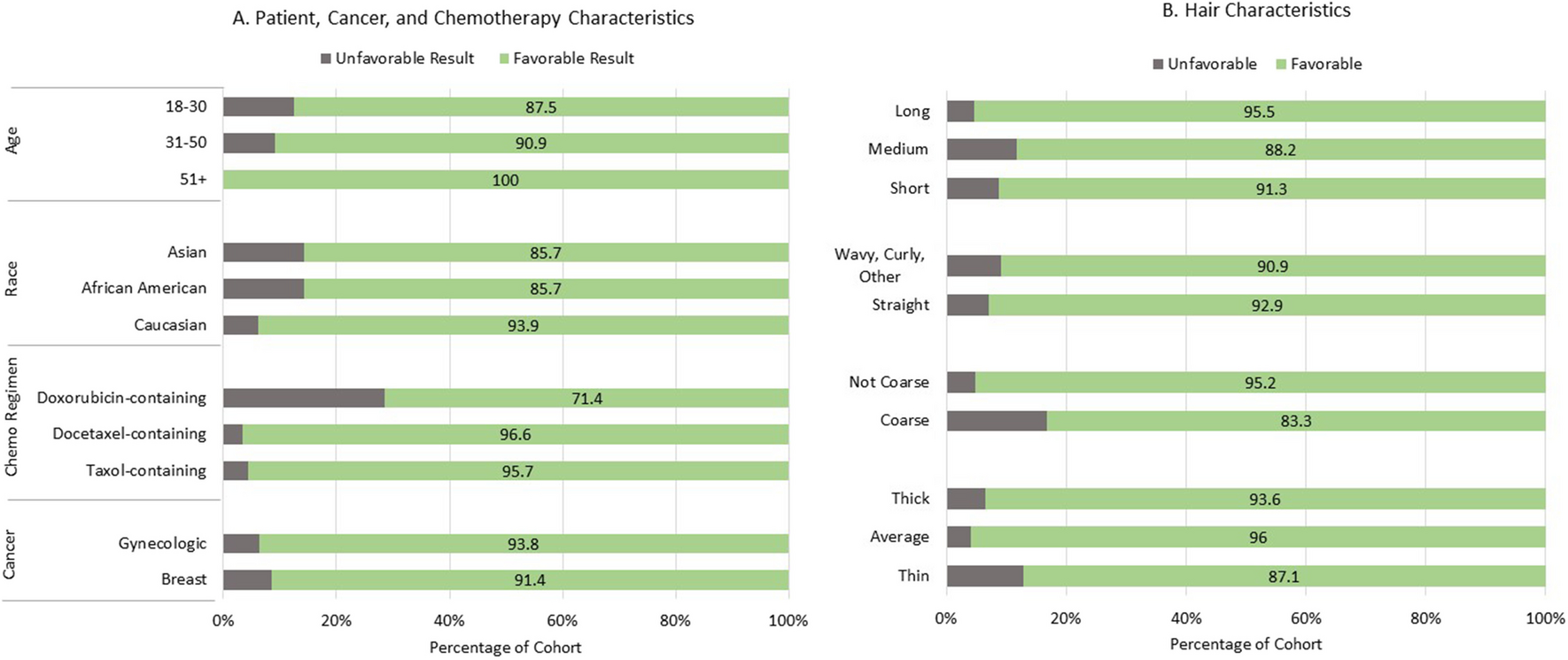
Use of Penguin Caps has an overall 20–90% success rate, defined as hair loss < 50%, across several trials evaluating success in breast cancer [9, 11, 22, 23] and 79% success in a limited evaluation in cancer types [23]. The range of success rate is due, in part to measures of success (patient-reported vs. objective measures) and regimens used, with better success in non-anthracycline-based, shorter regimens [23]. It is also unclear from literature how much effectiveness varies based on patient characteristics such as hair type.
As such, the purpose of this retrospective, descriptive study was to evaluate data that are routinely recorded during the cold capping process to determine tolerability and subjective effectiveness of cold capping in minimizing CIA. We further sought to determine whether CIA varies according to chemotherapy regimens or patient/hair characteristics prior to starting chemotherapy/capping, including race, ethnicity, and hair thickness, coarseness, length, and type (e.g., straight vs. curly).


留言 (0)