
記住我

The searches were last undertaken on 23rd July 2023. The Medline search identified 9091 references, and 142 full-text articles were retrieved and reviewed. The search of the Cochrane Central Register of Controlled Trials identified 1352 references, with 12 deemed relevant (one not identified in Medline search). Similarly, the search of the Cochrane Database of Systematic Reviews identified 45 references, with one deemed relevant (not identified in the Medline search). Ten additional articles were identified from the reference lists of the retrieved articles/Cochrane systematic review.
The sub-group proposes 12 expert opinion statements (Table 3).
Table 3 Expert opinion statements regarding clinically assisted hydration in patients with advanced cancerExpert opinion statements 1.All patients with advanced cancer should be regularly assessed regarding hydration/dehydration.
All patients with advanced cancer should be regularly assessed to ensure that they are hydrated (and not dehydrated). Assessment involves taking a history (to determine presence/absence of thirst, fluid/food intake, and fluid losses), performing an examination (to look for signs of dehydration, see Table 2), and undertaking appropriate investigations (to look for indicators of dehydration, see Table 2) [24]. In patients with reduced fluid intake or increased fluid losses, it is important to determine the underlying cause(s) and whether there is any potential for reversibility (see statement 3).
Although clearly related, patients require separate assessments for the need for CAH and the need for clinically assisted nutrition [16]. The MASCC Palliative Care Study Group has published an analogous guidance on the use of clinically assisted nutrition in patients with advanced cancer [39]. Anorexia/reduced food intake may be associated with dehydration (due to reduced fluid intake).
2.Patients should be practically supported to maintain oral intake.
Many patients with advanced cancer, especially patients in the terminal phase, require support to maintain their fluid/food intake due to general frailty and/or specific problems (e.g. dysphagia, low mood). Support ranges from encouraging drinking, making drinks, assisting drinking (e.g. repositioning patient, holding cup), use of “drinking aids” (e.g. drinking straws, beakers), and input from a speech and language therapist (where appropriate). It should be noted that there is “no convincing evidence” to support the use of fluid “thickeners” in patients with dysphagia [40].
3.Reversible causes of decreased fluid intake, or increased fluid loss, should be treated.
Patients with advanced cancer may develop a number of problems, which result in reduced fluid intake (e.g. oral pain, dysphagia), increased fluid loss (e.g. diarrhoea), or both (e.g. vomiting): these “hydration impact symptoms/problems” may be related to the cancer, the cancer treatment, or co-morbid conditions. Many of these problems are potentially reversible, and appropriate treatment may or may not negate the need for ongoing CAH (although some patients will require CAH in the short term). It is also important to review the patient’s medication and consider reducing/stopping drugs which may be adding to fluid losses (e.g. diuretics, laxatives).
4.Decisions relating to clinically assisted hydration should be made by an appropriately constituted multidisciplinary healthcare team together with the patient and their family.
The decision whether or not to initiate CAH, and how to provide CAH, depends on a number of factors (Box 2), and so requires input from the oncology team, the supportive care/palliative care team, other specialist teams/services (e.g. gastroenterology, interventional radiology), and the patient and their family.
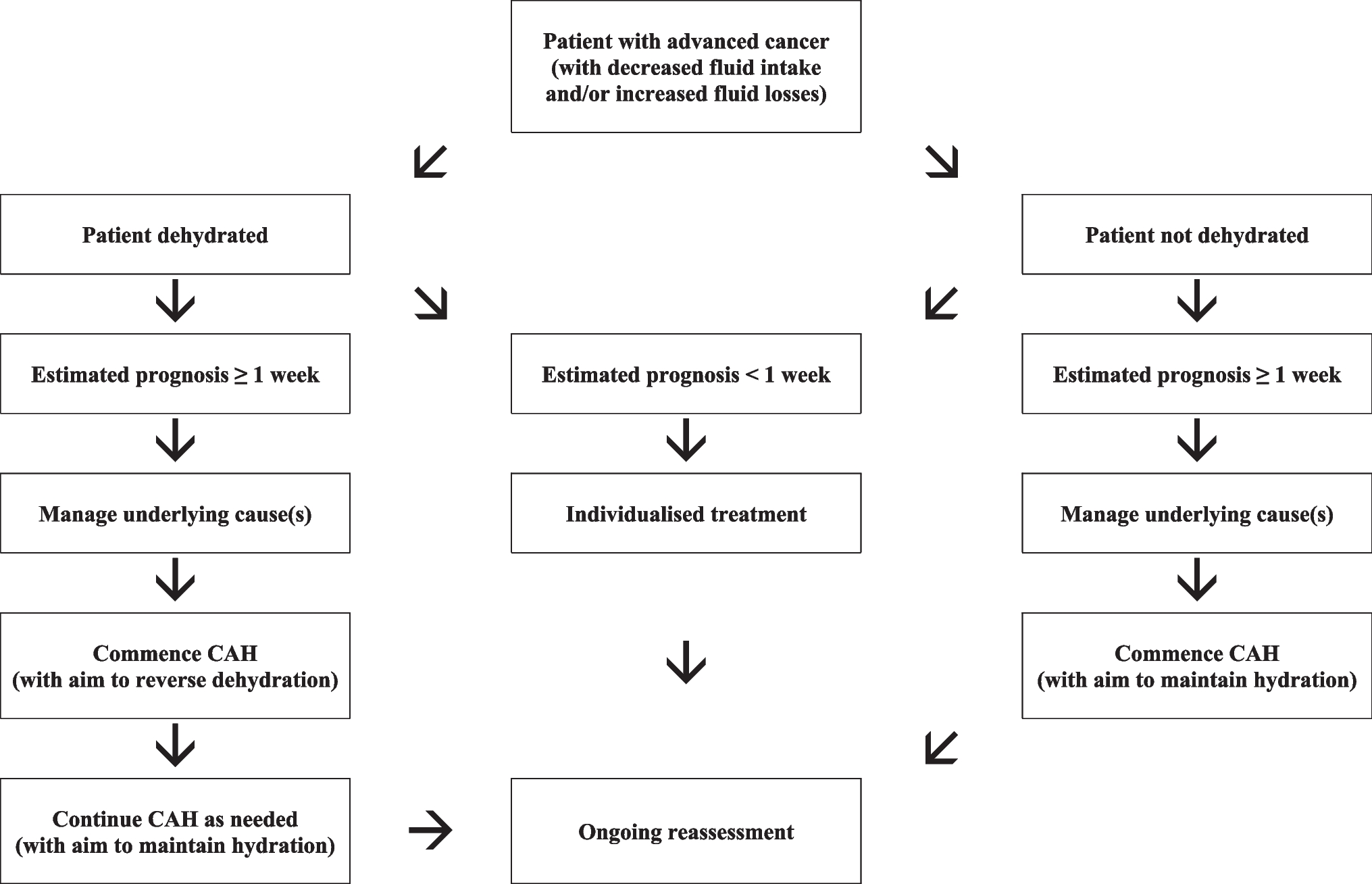
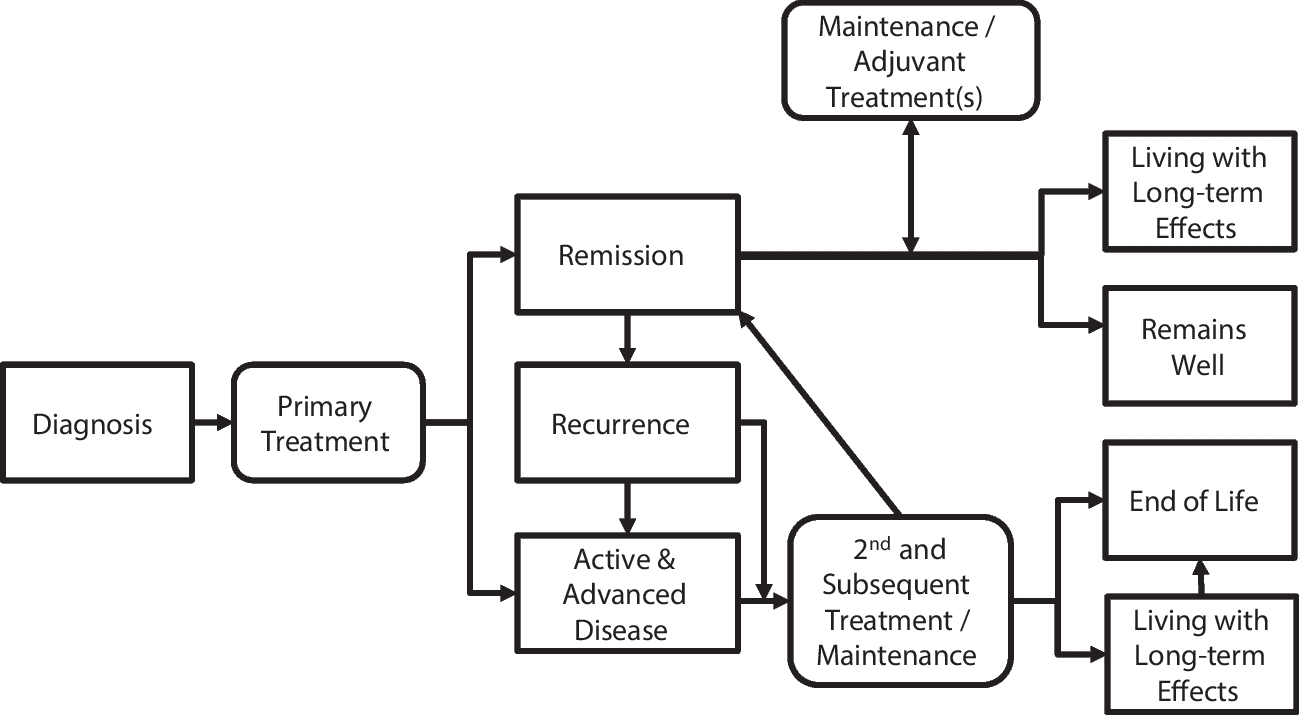
In patients with a prognosis of weeks to months, the decision to initiate CAH is usually not difficult or controversial, and the main issue relates to the route of administration. However, in patients with a prognosis of days, the decision is often much less straightforward (for the already outlined reasons). Importantly, such decisions must be individualised, and a “blanket” policy of everyone receiving CAH, or nobody receiving CAH, is neither clinically, ethically, nor socially justifiable (Fig. 1).
Fig. 1
Decision algorithm for CAH in patients with advanced cancer
Box 2 Clinical considerations relating to provision of CAH in patients with advanced cancer 5.Clinically assisted hydration should be considered in patients at risk of dying from dehydration before dying from their cancer
The primary indication for CAH in this cohort of patients is the prevention of premature death from dehydration (as opposed to inevitable death from the cancer) (11: Druml et al., 2016). As discussed, the evidence suggests that healthy individuals with no fluid/food intake will die from dehydration within a few days in temperate climates. Thus, our suggestion is that cancer patients with insufficient fluid intake, and an estimated prognosis of ≥ 1 week, should always be considered for CAH. Moreover, our suggestion is that in cases of uncertainty, a trial of CAH should be considered, with precise criteria for continuation/discontinuation (see statement 7) [11].
In patients with an expected prognosis of < 1 week, indications for CAH include “symptom control” (e.g. relief of thirst, management of opioid toxicity) and amelioration of patient and family carer distress relating to withholding/withdrawing CAH. In the latter scenario, there must obviously be no contraindications to the initiation/continuation of CAH.
6.Protocols/processes should exist to deal with conflicts over the initiation (or withdrawal) of clinically assisted hydration.
The provision of CAH is often an emotive subject for patients and their families (particularly in the terminal phase) [6, 7]. As discussed, CAH is a medical treatment, and patients (and/or their families) do not have the right to demand the treatment. In cases of conflict, it is recommended obtaining a second opinion from a suitably qualified healthcare professional: other options such as involvement of a clinical ethics committee or involvement of the legal system are not generally required in this cohort of patients [11].
7.Patients receiving clinically assisted hydration should have a “hydration” care plan which defines the agreed objectives of treatment and the agreed conditions for withdrawal of treatment.
Patients receiving CAH should have a “hydration” care plan which includes the rationale for treatment, the specifics of treatment (e.g. method of CAH), details about ongoing follow-up, details about ongoing reassessment, the indications for continuation of treatment, the indications for discontinuation of treatment, and contact details for relevant healthcare professionals [11].
8.Patients should be given fluids via the most appropriate route (for that patient).
As discussed, CAH can be administered via the enteral, intravenous (IV), or subcutaneous (SC: hypodermoclysis) routes [14]. Enteral administration may be via feeding tubes within the stomach and small intestine or catheters within the rectum (PR: proctoclysis). The choice of route depends on a number of factors, including availability/suitability of the various routes, access to specialist teams/services (e.g. gastroenterology, interventional radiology), current/future place of care, access to relevant supports (e.g. community nurses, family carers), and particularly patient preference.
The IV route is the usual route for administering CAH in the hospital setting, and should always be considered in patients with indwelling intravenous catheters. In other patients, the intravenous route may be indicated (as opposed to the SC route) when large volumes of fluid are required, electrolyte disturbances need correcting, there are skin integrity problems, or there are coagulation problems [41].
The SC route is a well-established route for administering CAH in a variety of settings (e.g. home, hospice) [42,43,44]. Hypodermoclysis has been repeatedly reported to be effective and generally well tolerated [41]. The main advantages (versus IV route) include ease of usage (requiring minimal training), lower incidence of serious adverse effects (e.g. infection, fluid overload), and lower direct and indirect costs [41].
Various regimens have been used to administer subcutaneous fluids [41, 45]. Non-metal cannulas (22–24 G) are generally recommended and should be changed every 24–48 h to prevent infection/inflammation (or sooner if required): cannulas should be inserted in areas with adequate subcutaneous tissue, and usual sites include the lower lateral abdomen, the upper lateral chest, the scapula, and the upper legs (and to a lesser extent the upper arms). Subcutaneous fluids can be given intermittently or continuously (depending on the volume required): they are generally administered using gravity (rather than with infusion devices), since this technique is simple, effective (with adequate precision), and well tolerated. Different fluids have been used (e.g. 0.9% sodium chloride, 0.18% sodium chloride/4% glucose, 5% glucose), and the choice of fluid depends on the specific clinical situation. Giving sets should be changed every 24 h to prevent infection. Asymptomatic swelling is often seen at the site of the cannula due to the volume being infused, and this is not in itself a reason to re-site the cannula or terminate the infusion.
Early reports of the use of hypodermoclysis within palliative care settings included the use of hyaluronidase to facilitate distribution of the fluid within the connective tissues (and so absorption of fluid into the systemic circulation) [43, 44]. A review of the literature concluded that hyaluronidase is not indicated in most cases [41]. Furthermore, hyaluronidase is relatively expensive (and often difficult to acquire) and has been linked to additional adverse effects (e.g. allergic reactions, fluid overload).
The PR route is an option for administering CAH when other routes are not available/suitable. Proctoclysis has been reported to be effective and generally well tolerated (although there is much less data on this route of administration) [46, 47].
9.Patients who are dehydrated should be given sufficient fluids to reverse the dehydration.
If a patient is dehydrated, and the decision is made to commence clinically assisted hydration, then the goal of treatment should be to reverse dehydration in a timely manner: the volume of fluid, type of fluid (including electrolytes), and rate of infusion should be individualised. Important factors to consider are the degree of dehydration, ongoing fluid losses (i.e. homeostatic, pathological), and relevant co-morbidities (e.g. diabetes mellitus, cardiac problems, renal disease). Routine biochemical testing should be used to guide fluid and electrolyte replacement (except in patients in the terminal phase). Once the patient is rehydrated, an assessment must be made regarding the necessity for ongoing/ “maintenance” treatment (see statement 10).
10.Patients who are not dehydrated should be given sufficient fluids to maintain hydration/prevent dehydration.
If a patient is not dehydrated, and the decision is made to commence clinically assisted hydration, then the goal of treatment should be to maintain hydration: the principles of management in hydrated patients are similar to those in dehydrated patients (although smaller volumes of fluid are generally necessary).
In general, the volume of fluid provided needs to fully match the ongoing fluid losses (i.e. homeostatic, pathological) in order to prevent the occurrence of dehydration. NICE has developed guidance on CAH for adult hospital patients [35]: they recommend 25–30 ml/kg/day of water (with electrolytes/glucose) for maintenance, with lesser volumes (20–25 ml/kg/day) for older persons, and those with frailty, cardiac failure, renal impairment, and malnutrition. The latter guidance is appropriate for many patients with advanced cancer, who have a prognosis of weeks to months, and where the goal of CAH is to maintain hydration (and prevent death due to dehydration).
In the terminal phase, it may be appropriate to use smaller volumes of fluid for “symptom control”, e.g. relief of thirst and management of opioid toxicity: in such cases, the volume of fluid should be titrated to achieve the desired outcome, and this requires an individualised approach.
11.Clinically assisted hydration should be available in all settings, including the home setting.
The provision of CAH for patients with advanced cancer is feasible (and safe) in the home/similar settings, and so a planned discharge from hospital should not be a major factor in the decision to withhold/withdraw relevant treatments. Furthermore, it has the potential for significant cost savings (versus ongoing care in hospital/hospice settings) [48].
CAH has been given subcutaneously (hypodermoclysis) [42, 49,50,51], intravenously [52], via nasogastric tube/gastrostomy, and rectally (proctoclysis) [46, 47], in the home and similar settings. Importantly, non-professional carers (family) have been able to administer the CAH in these settings (when appropriate and with relevant training) [46, 47, 50, 51].
12.All patients receiving clinically assisted hydration should be regularly reassessed.
All patients receiving CAH should be regularly reassessed with regard to the continuation, amendment, or discontinuation of the relevant treatment [11]. The objectives of reassessment are to (a) ensure the CAH is meeting the patient’s hydration requirements (i.e. that the patient is not under- or over-hydrated), (b) ensure the CAH is well tolerated, (c) ensure the CAH remains acceptable to the patient, and (d) ensure the CAH remains appropriate/consistent with the “goals of care”.
Patients receiving long-term CAH, and especially patients with ongoing GI fluid losses (i.e. vomiting, diarrhoea, high output stomas, small bowel fistulas), require regular biochemical monitoring to guide fluid and electrolyte replacement. Patients in the terminal phase do not require regular biochemical monitoring.
留言 (0)