
記住我

Stroke is a common and frequently occurring condition in middle-aged and elderly people. Its high disability rate and mortality place a heavy burden on society and families. Dysphagia is a common issue related to stroke, and its incidence varies from 29% to 81%.[1] Post-stroke dysphagia (PSD), with 2024 ICD-10-CM Diagnosis Code I69.391 (dysphagia following cerebral infarction), is related to the decline of oral, pharyngeal, and esophageal functioning, in addition to other serious problems, such as airway obstruction, aspiration, aspiration pneumonia, dehydration, malnutrition, sepsis, and death; it can also lead to social isolation, affect the patient quality of life, and may lead to the delay of rehabilitation and increase the economic burden.[2] Therefore, it is very important to effectively accelerate the recovery of swallowing function to reduce these risks.
Swallowing rehabilitation behavioral therapy, based on the principle of neuroplasticity, for example, oropharyngeal strengthening, and exercises that target range of motion, is a frequently used therapeutic approach.[3,4]
Traditional Chinese acupuncture therapy is also widely used in stroke rehabilitation treatment and can significantly improve the swallowing function and other stroke sequelae[5] of patients in the treatment of PSD. For example, the acupuncture method of “refreshing the brain and opening the orifices” is the principle for treating the sequelae of stroke, as proposed by Academician Shi Xuemin, and is a mature acupuncture method that is broadly used in clinics, with the literature reporting that the short and long-term curative effects of this approach show obvious advantages over rehabilitation training.[6] Yu et al conducted a randomized controlled trial to treat post-stroke dysphagia. The results confirmed that acupuncture, in conjunction with neuromuscular electrical stimulation (NMES) and rehabilitation training, enhances the therapeutic effects on post-stroke dysphagia during the recovery phase, improving patients’ swallowing function and quality of life.[7] But its therapeutic mechanism is still unclear.
The purpose of the present study was to analyze changes in the swallowing function of patients with PSD after intensive pharyngeal exercise, as well as swallowing exercise combined with electro-acupuncture, and to explore its mechanism through changes in electromyography and cerebral blood flow. The details are reported as follows.
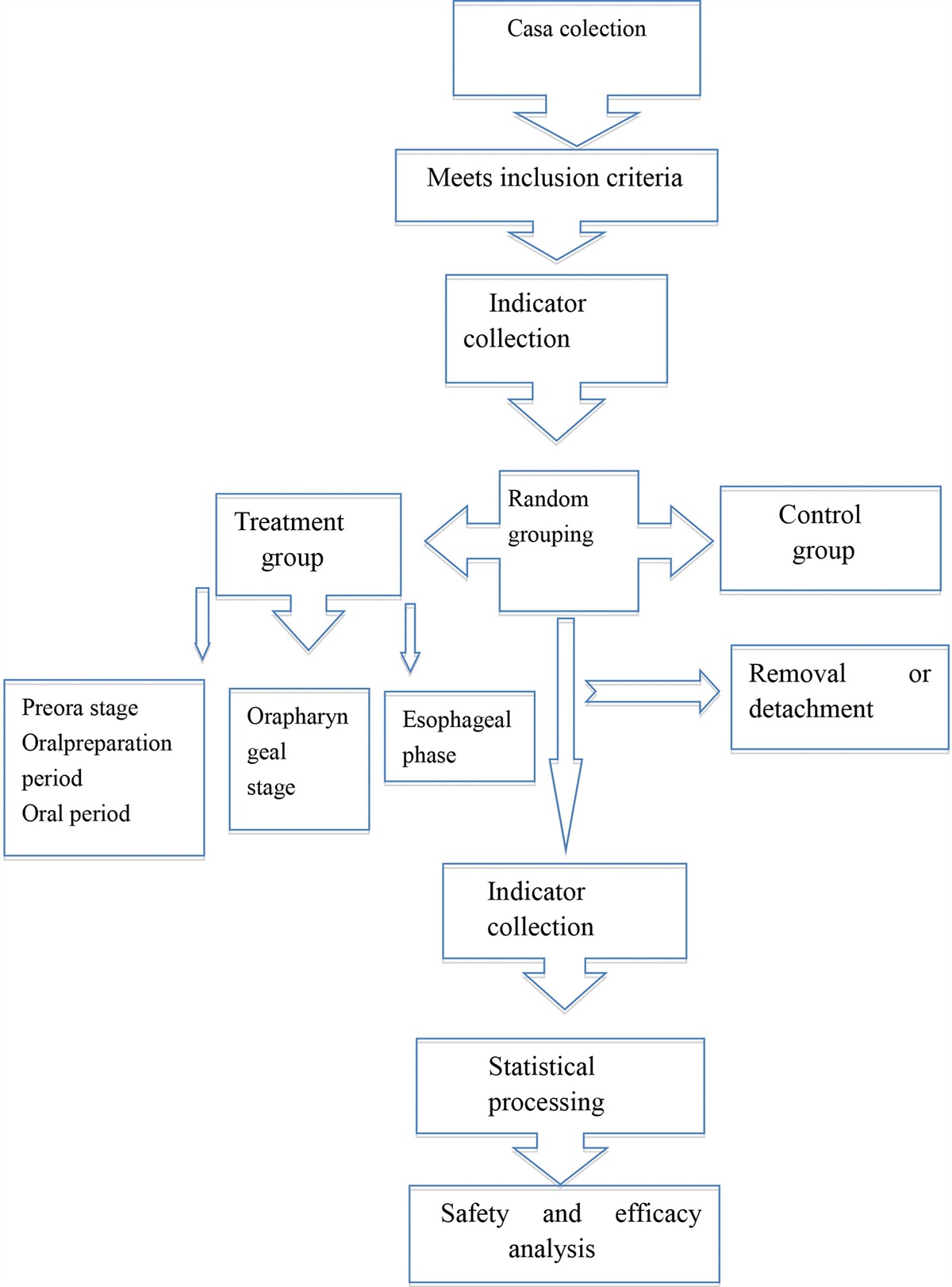
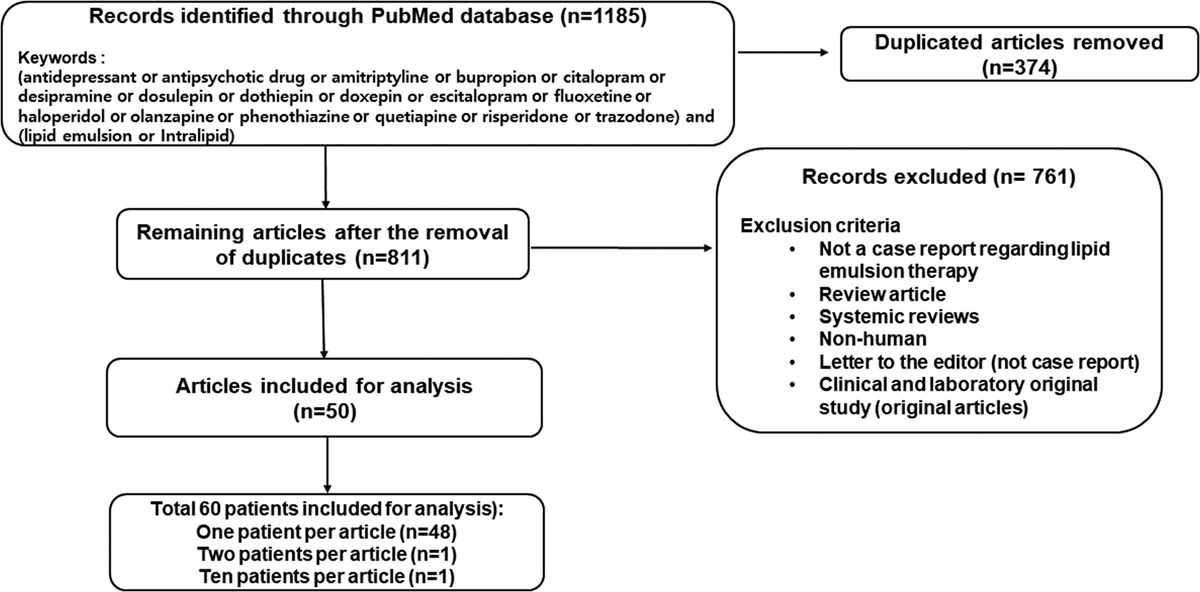
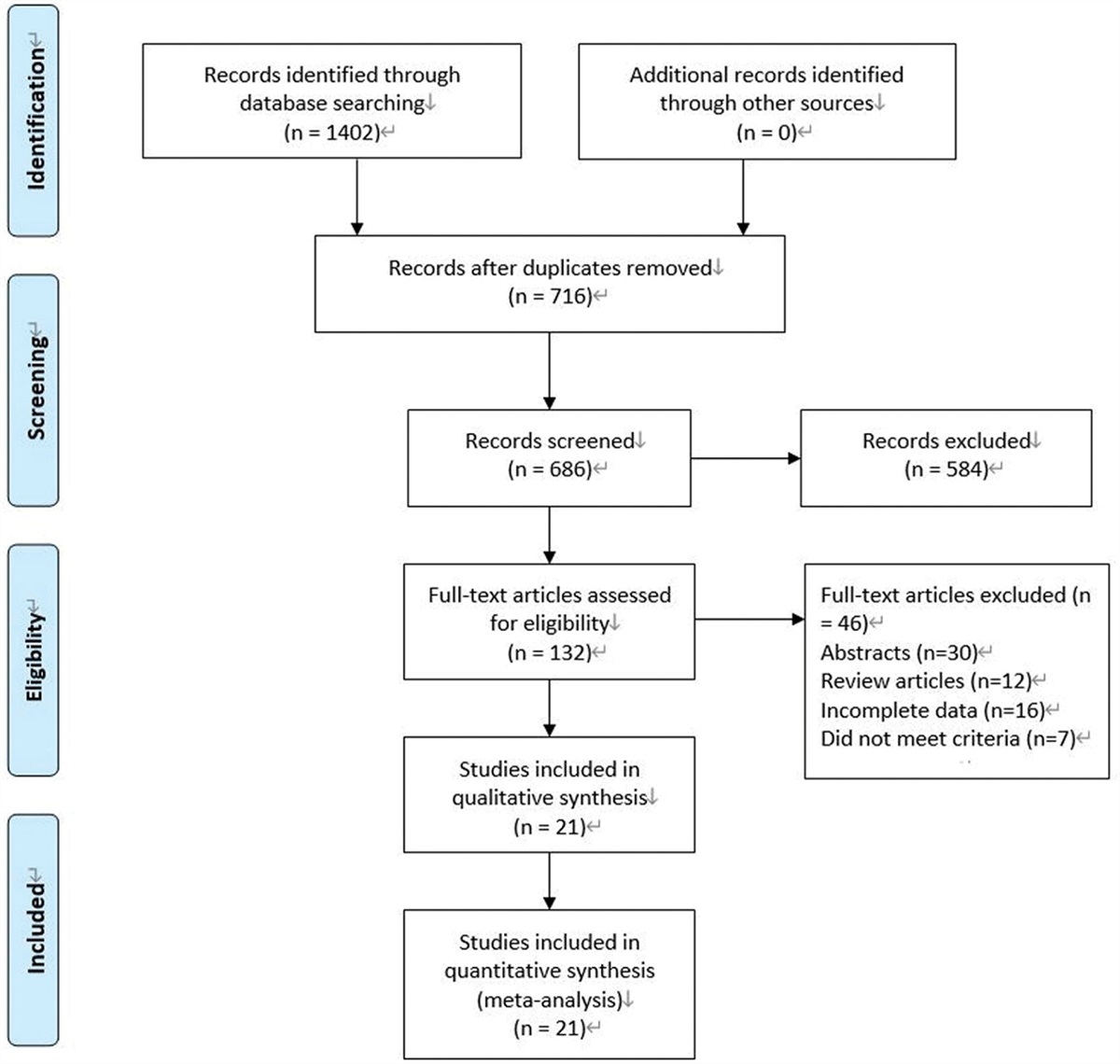
2. Methods 2.1. Data and methods 2.1.1. General information.A total of 120 PSD patients who had been admitted to the Wuhan Hospital of Traditional Chinese Medicine from May 2020 to May 2021 were enrolled in this randomized controlled trial. A number was assigned to each patient, based on their visiting order time. Each patient was provided with information regarding to the study, and then signed the informed consent. Random numbers were generated by non-participants using SPSS22.0 software, and the random numbers and grouping information were packed into sealed, opaque envelopes. The envelopes were extracted in sequence according to the order of treatment, and the patients were divided into experimental group and control group according to the ratio of 1:1, with 60 cases in each group. The assessors were blinded to the treatment allocation of the participants to reduce potential bias. The research flowchart is shown in Figure 1.
 Figure 1.:
Figure 1.: The research flowchart.
The formula for sample size calculation is: N = Z²*σ²/d², where Z represents the confidence interval, n is the sample size, d is the margin of error, and σ represents the standard deviation.
The screening, diagnosis and treatment of dysphagia were accomplished through multidisciplinary collaboration. Screening for dysphagia is done by a professional nurse. The severity of dysphagia or to guide the management of dysphagia and acupuncture treatment is performed by rehabilitation therapists and Chinese medicine acupuncturists. Instrumental assessment of swallowing function was performed by a radiologist in collaboration with a speech therapist or physician in charge. All doctors, nurses and medical personnel involved in dysphagia examination received formal training.
2.1.2. Inclusion criteria.Patients met the diagnostic criteria put forth in the Chinese Expert Consensus on Evaluation and Treatment of Dysphagia (2017)[8]: a. Patients diagnosed as dysphagia by swallowing evaluation and have the main symptoms of dysphagia and cough after drinking water; b. the water swallowing test rating is 3 to 5. Patients were in the recovery period of stroke and the (stroke) onset time ranged within 2 weeks to 3 months. Patients were in a stable condition and were conscious. Patients could maintain a sitting position for at least 30 minutes. Patients could cooperate to complete relevant rehabilitation training and examination items. Patients were aged ≥ 18 years. All of the patients and their families provided signed informed consent for inclusion in the study.
2.1.3. Exclusion criteria.Patients who were complicated with malignant tumors and/or other serious underlying diseases and who were unable to cooperate in the completion of the research. Patients who were complicated with a previous history of swallowing dysfunction. Patients with dysphagia caused by muscle weakness, drugs, or other diseases. Patients who were complicated with other procedures, such as throat surgery, infection, or trauma. Patients who were complicated with neurological or cognitive impairment caused by diabetes and/or other diseases.
2.1.4. Drop-out criteria.Serious complications occurred during treatment, and the treatment plan required adjustment. The patient voluntarily asked to withdraw from the study. Cases where patient compliance was poor and where patients did not receive intervention in strict accordance with the doctor advice. Patients who were lost to follow-up during treatment.
2.2. Treatment methods 2.2.1. Routine treatment.The patients in both groups were given routine cerebrovascular disease treatment and underwent swallowing rehabilitation exercises.
2.2.2. Swallowing muscle training.Both groups of patients used active or passive methods to train swallowing muscle function, in which the active training content included exaggerated chewing or mumps movement, resistance blowing movement, and rolling the tongue upward or moving it laterally. Passive training mainly included Mendelsohn training, Shaker training, and deep breathing training. Respiratory muscle exercises lasted 30 minutes each time, once a day, 5 times a week for 4 weeks.
The cold stimulation training method proceeded as follows: a long cotton swab wrapped in gauze was dipped into normal saline and frozen. The patient took a sitting or semi-lying position and the frozen cotton swab was used to stimulate the root of the tongue, soft palate, and throat wall in turn. Concurrently, fingers rapidly rubbed the skin covering the thyroid cartilage and the mandibular margin, and the patient was instructed to perform an empty swallow. The training time for this exercise was 20 minutes each time, once a day, 5 times a week, all completed on an empty stomach, for 4 weeks in total.
2.2.3. Acupuncture treatment.The experimental group received acupuncture treatment according to the “Sharpening mind and inducing consciousness” acupoint compatibility scheme.[9] Based on traditional Chinese medicine theory and the national standard (Nomenclature and location of Meridian points, GB12346-90), the acupoints used in this study included bilateral fengchi (GB20), shuigou (DU26), lianquan (RN23), neiguan (PC6), sanyinjiao (SP6), yifeng (SJ17), jinjin (EX-HN12), and yuye (EX-HN13) (Fig. 2).
 Figure 2.:
Figure 2.: Map of acupuncture points on different body parts.
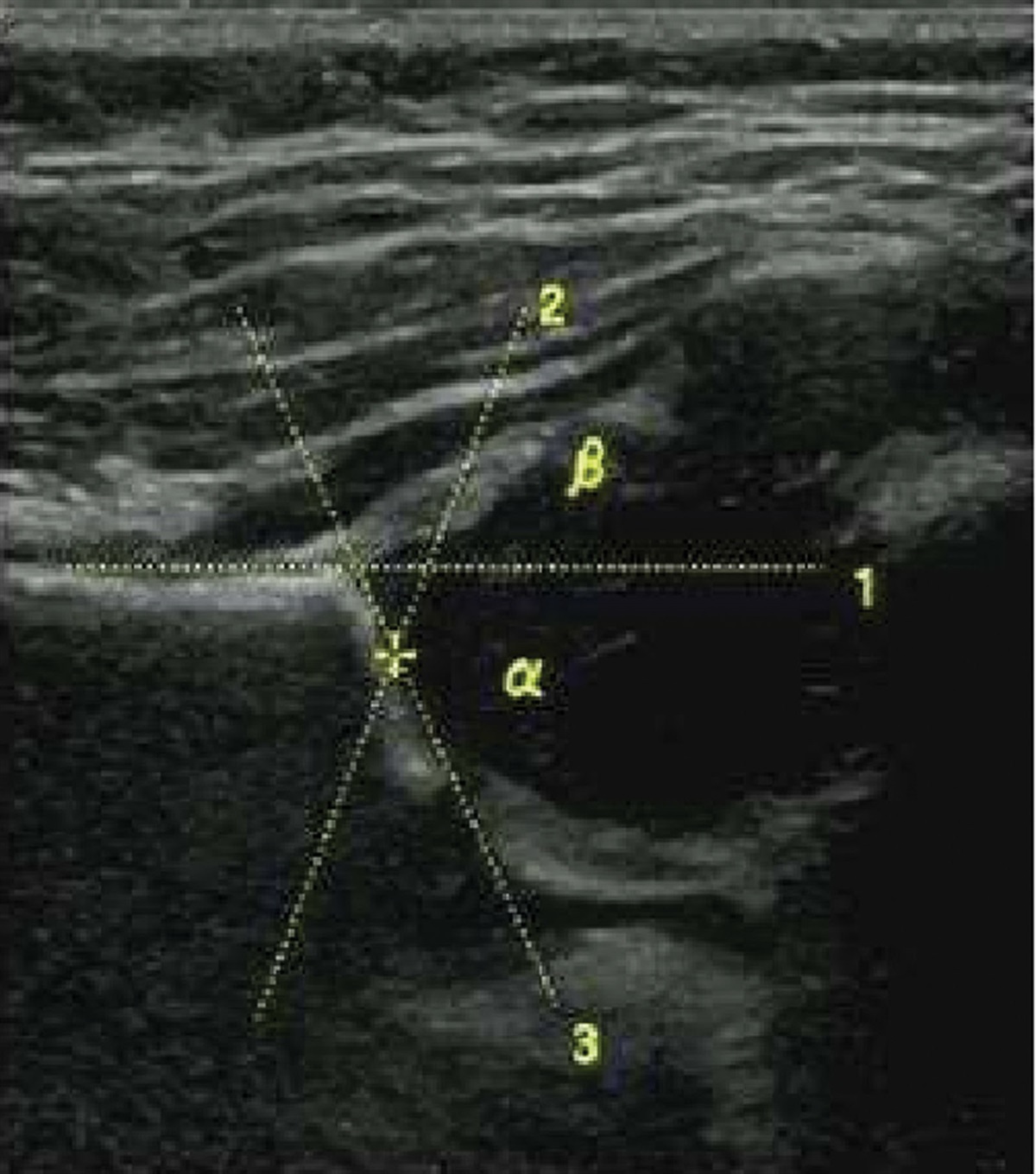
The procedural methods of the acupuncture treatment were as follows. The bilateral fengchi acupoints were stabbed 2.5 to 4 mm toward the tip of the nose, and bilateral yifeng acupoints were obliquely stabbed 2.5 to 4 mm to the root of the tongue. Both acupoints were treated with twisting–twirling reinforcing manipulation for 1 minute at a frequency of 120 to 160 times/min, and the angle of each time was <90° until the sensation of numbness spread to the front of the tongue and the throat. Fengchi acupoint is connected to the electro-acupuncture instrument, with continuous wave and frequency of 2Hz (Fig. 3). The shuigou acupoint, which is located one-third above renzhonggou, was obliquely stabbed with a needle tip in an upward direction at 0.7 to 1.7 mm deep; the needle body was twisted for 1 cycle, and the bird-pecking technique was applied until the surface of the patient eye became moist. For the lianquan point, the needle was directly inserted until it was oriented 1.7 to 2.7 mm toward the root of the tongue, and the twisting method was applied at 100 times/min for 15 seconds. The neiguan point was directly punctured for 1.7 to 3.3 mm, and the twisting–whirling–lifting–inserting reducing method was applied for 1 minute. The sanyinjiao was penetrated with a needle, 3.3 to 4.9 mm obliquely and at a 45° angle from the posterior edge of the tibia; the lifting–inserting reinforcing method was used until the patient experienced 3 minor twitches in the lower limbs. The jinjin and yuye points were pricked until bleeding (1–2 mL) occurred. In the acupuncture treatment, the neiguan and shuigou points were stimulated once every 3 days, pricking and bleeding were completed at the jinjin and yuye points once every 2 days, and other acupoints were stimulated once a day. The needle was kept for 30 minutes each stimulation, and the course of treatment was 4 weeks.
 Figure 3.:
Figure 3.: Fengchi acupoint.
The acupuncture needles used in the above procedures were all 0.25 × 40 mm disposable sterile stainless steel needles (Suzhou Medical Appliance Factory Co., Ltd.). The acupuncture operation was performed in accordance with the Reporting Practice for Interventions in Acupuncture Clinical Trial (Standards for Reporting Interventions in Clinical Trials of Acupuncture, STRICTA).
2.3. Observation indexes Swallowing function: A video fluoroscopic swallowing study (VFSS), the most commonly used method to examine swallowing function and considered the “gold standard” for the detection and diagnosis of swallowing disorders,[8] was conducted to evaluate the swallowing function of the patients in the 2 groups before and after treatment. All of the examinations after treatment were completed the same day after the treatment. Method: Semiliquid food (10 mL) containing 60% barium sulfate was prepared. The patient was asked to sit down and swallow the liquid, during which the swallowing process was observed using an ICONOS R200 X-ray machine (Siemens, Germany). The severity of symptoms in the oral phase (0–3 points), throat phase (0–3 points), and aspiration (0–4 points) were evaluated, respectively. The total score was 0 to 10 points, where a score of 10 indicated normal swallowing, a score of 7 to 9 indicated a mild abnormality, 4 to 6 points indicated a moderate abnormality, and a score of 0 to 3 points indicated a severe abnormality. The method for judging the curative effect was as follows[10]: after treatment, a VFSS score of 10 points indicated a cured condition, an increase in the VFSS score ≥ 2 points and not reaching the normal level was considered to have been excellently effective, and an increase ≥ 1 point and not reaching the normal level was considered effective; no increase or a decrease was considered an effective outcome. The total effective rate = (recovered cases + excellent cases + effective cases)/ total cases × 100%. Standard swallowing function score: The standard swallowing assessment (SSA) scale was used to evaluate the 2 patient groups before and after treatment.[11] The assessment content included 3 parts as follows: 8 to 23 points were given in the preliminary evaluation, including the state of consciousness, breathing mode, and pharyngeal reflex; 5 to 11 points were given for drinking 5 mL of water, including cough, choking, or water leakage; 5 to 12 points were given for drinking 60 mL of water, including cough, choking, and swallowing time. The total SSA score was summarized according to the 3 measurement types for a total of 18 to 46 points. A lower score indicated better swallowing function. Brainstem auditory evoked potential (BAEP): The BAEP was tested before and after treatment with the Keypoint full-function myoelectric instrument and supporting software (Alpine Biomed, Denmark). The recorded parameters included the peak latency (PL) of waves III and IV and the inter-peak latency (IPL) between waves III to V and I to V. Cerebral blood flow signal detection: Before and after treatment, the spectrum morphology and blood flow signal of the middle cerebral artery were observed using a video E9 Doppler ultrasound (General Electric, USA) and a 2 MHz probe; the detection indexes included peak systolic velocity (PSV), end-diastolic velocity (EDV), mean velocity (MV), and the pulsatility index (PI). 2.4. Statistical methodsCount data were expressed as a percentage (%) and compared among groups using the chi-square (χ2) test. Independently ranked data were compared between the 2 groups using a Wilcoxon rank-sum test. Measurement data first underwent a normality test using the Kolmogorov–Smirnov method. Normally distributed data were expressed as mean ± standard deviation (x̄± SD). An intergroup comparison was conducted using an independent sample t-test, and an intra-group comparison was conducted among different time points using a paired t-test. The data were analyzed using the SPSS Statistics 22.0 software; P < .05 was considered statistically significant.
3. Results A comparison of the basic data between the 2 groups. During the treatment period, in the observation group, 1 case was lost to follow-up, and 2 cases actively withdrew from the study (a total withdrawal of 3 cases [4.84%]). In the control group, 1 case failed to strictly follow the doctor instruction, 2 cases were lost to follow-up, and 2 cases voluntarily withdrew from the study (a total withdrawal of 5 cases [8.06%]). There were no significant differences in the basic data, such as gender, age, and a history of smoking and drinking between the 2 groups (all P > .05; Table 1). A comparison of the therapeutic effects between the 2 groups. The therapeutic effects were significantly better in the observation group than in the control group (P < .05); the effective rates of the 2 groups were 94.92% and 82.46%, respectively (P < .05; Table 2). A comparison of the SSA scores between the 2 groups before and after treatment. It has been proved that SSA shows high sensitivity and specificity for detection of dysphagia, as well as good agreement with summative clinical judgment of swallow function.[12] Reliability test of SSA in this study: all 120 patients completed 2 SSA assessments. Intra-group reliability: there was A high correlation between the 2 evaluation results of rater A, intraclass correlation efficient (ICC) = 0.82 (P < .01); Intergroup reliability: At the second assessment, there was a high correlation between the results of the 2 raters, ICC = 0.84 (P < .01). Validity test of SSA: the total SSA score of 120 patients (the average SSA score of 2 evaluators at the second assessment) was highly correlated with the total score of VFSS dysphagia, r = -0.88 (P < .01). Intra-group reliability: There was A high correlation between the 2 evaluation results of rater A, ICC = 0.82 (P < .01); Intergroup reliability: at the second assessment, there was a high correlation between the results of the 2 raters, ICC = 0.84 (P < .01). According to the statistical point of view, ICC > 0.8 indicates that the scale has good repeatability test reliability. Following treatment, the preliminary scores of the SSA scale, the scores for drinking 5 ml of water, and the score for drinking 60 ml of water decreased significantly in both groups (P < .05). The scores for drinking 5 ml of water and drinking 60 ml of water in the observation group were lower than those in the control group, and the differences were statistically significant (P < .05; Table 3). A comparison of the BAEP parameters between the 2 groups before and after treatment. After treatment, the PL of waves III and IV, and the IPL between waves III to V and waves I to V in the BAEP were shorter than those before treatment in both groups, and the differences were statistically significant (P < .05). The improvement was more significant in the observation group, and the difference was statistically significant (P < .05, Table 4). A comparison of cerebral blood flow signals between the 2 groups before and after treatment. Following treatment, PSV, EDV, and MV increased significantly in both groups (P < .05); the PI decreased significantly in both groups (P < .05), and in the experimental group, PSV, EDV, and MV were higher than in the control group (P < .05). The PI was lower in the experimental group, and the differences were statistically significant (P < .05; Table 5). Comparison of adverse reactions in 2 groups during treatment. The total incidence of adverse reactions was 7.02 % in control group, and 8.47 % in the experimental group. There was no significant difference between 2 groups (χ2 = 0.403, P = .704), as shown in Table 6. Table 1 - Comparison of basic data between the 2 groups. n Experimental group Control group χ2/t P 59 57 Gender Male 30 31 0.146 .703 Female 29 26 Age 58.47 ± 9.26 57.61 ± 9.83 0.485 .629 Smoking history 24 19 0.670 .413 Drinking history 17 16 0.008 .929 AIS course 39.48 ± 7.92 40.19 ± 8.35 0.470 .639 Lesion sites Cortex 7 9 0.743 .863 Subcortex 20 21 Brainstem 19 17 Others 13 10Compared with the control group,
*P < .05.
SSA = standardized swallowing assessment.
Compared with the same group before treatment,
*P < .05.
BAEP = brainstem auditory evoked potential, IPL = inter-peak latencies, PL = peak latencies.
Compared with the control group after treatment,
*P < .05.
MV = mean velocity, PI = pulse index, EDV = end-diastolic velocity, PSV = peak systolic velocity.
Compared with the same group before treatment,
*P < .05; Compared with the control group,
#P < .05.
Physical therapy, swallowing training, balloon catheter dilation and other means are generally used for the treatment of swallowing disorders after stroke, but these treatments have disadvantages such as high cost, long treatment cycle and poor compliance, which are not good for clinical promotion and application.[13] There are also emerging therapeutic approaches such as transcutaneous and intra-pharyngeal electrical stimulation, pharmacological stimulation of transient receptor potential channels through vanillin subtype agonists and noninvasive brain stimulation techniques, repetitive transcranial magnetic stimulation and transcranial direct current stimulation, which are aimed at restoring swallowing function. However, symptoms of dysphagia persist in as many as 50–60% of patients after treatment, and the efficacy is not satisfactory.[14] In this study, the method of electro-acupuncture combined with swallowing rehabilitation training was used, and the swallowing function of the experimental group was improved by 94%, and the potential mechanism of action was further discussed.
In this study, an acupoint matching theory was derived from the acupuncture method of “refreshing the brain and opening the orifices,” established by Academician Shi Xuemin. This was combined with the principle of selecting acupoints along the meridians and locally, where neiguan, shuigou, and sanyinjiao were the main acupoints, supplemented by fengchi, jinjin, yuye, yifeng, and other acupoints for dysphagia. Additionally, electro-acupuncture stimulation was added to bilateral fengchi to realize the functions of refreshing the brain, opening the orifices, nourishing the liver and kidneys,and benefiting the pharynx.
Post-stroke dysphagia is a functional disorder caused by brain tissue injury. Based on the principle of neural plasticity, rehabilitative medicine can promote the recovery of swallowing function by establishing compensatory neural pathways and reestablishing a correct reflex arc through rehabilitation training. Therefore, the recovery of brain function injury has a significant impact on the improvement of swallowing function.[15] The method of stimulating cortical nerve plasticity by exogenous nerve stimulation to restore swallowing function is the main method of rehabilitation therapy. One approach is to stimulate the peripheral oropharyngeal sensory system by chemical, physical, or electrical stimulation; a second approach directly stimulates the pharyngeal motor cortex, for example, repetitive transcranial magnetic stimulation.[16]
Electro-acupuncture is an extension of acupuncture and is combined with modern electrotherapy using the basics of traditional acupuncture. It is commonly used to treat PSD in clinical treatment and research contexts. Through a comprehensive literature search of the database, Huang et al conducted a randomized controlled trial study to evaluate the impact of electro-acupuncture on PSD; the results showed that in the electro-acupuncture group, the effective rates for the treatment of PSD, the water swallowing test results, VFSS outcomes, the Ichiro Fujishima rating scale, and aspiration pneumonia were better than those in the control group.[17] Anatomically speaking, fengchi is located in the sensory fiber innervation areas of the glossopharyngeal, hypoglossal, and vagus nerves, with the vertebral artery and medulla oblongata in the deep layer. An existing study showed that stimulating this acupoint could improve blood supply to the cerebral artery. The deep part of the lianquan point is at the root of the tongue, and jinjin and yuye are located at the veins on both sides of the lingual frenum. Sensory afferent fibers of the hypoglossal nerve and glossopharyngeal nerve can be found in these areas, and the glossopharyngeal muscle group is dominated by the submaxillary hyoid muscle, the anterior abdomen of the digastric muscle, the genioglossus muscle, the pharyngeal constrictor muscle, and the cricothyroid muscle. These nerves and muscles represent the structural basis for normal swallowing function. An existing study revealed that conducting acupuncture at the above acupoints could directly stimulate nerve terminal receptors and reflexively enhance the regulation ability of the swallowing center in the brainstem. Accordingly, efferent impulses are transmitted to the effector (muscle) to realize the reconstruction of the swallowing nerve pathway and the recovery of neuromuscular function.[18]
Brainstem auditory evoked potential is a reliable method for detecting brainstem function following a stroke.[19] In this study, BAEP was used to evaluate changes in brainstem function before and after treatment.
The results showed that the PL and IPL of each wave of BAEP were significantly improved after treatment, and the improvement was more significant in the observation group. This suggested that electro-acupuncture at fengchi, lianquan, and other acupoints could improve the auditory conduction function of the brain stem. The mechanism in this regard may be the mechanical stimulation of the glossopharynx and the vagus nerve beneath the acu
留言 (0)