
記住我

Developmental dysplasia of the hip (DDH), including hip dysplasia, hip subluxation, and hip dislocation, is the most common disease of the hip joint in children. In the absence of timely treatment, DDH can lead to walking difficulties and secondary spinal and pelvic deformities, seriously affecting children’s health.[1] Early detection and treatment play a crucial role in the universally recognized principles of DDH treatment. Earlier treatment can be performed with a simpler method and brings more favorable outcomes.[2,3] We mainly studied infants and toddlers who had undergone physical examination in our hospital. After the high-risk screening, clinical screening, and ultrasound and X-ray examination, children with DDH were identified and early intervention was considered.
2. Materials and methods 2.1. General informationFrom January 2016 to December 2017, we selected infants and toddlers who had undergone physical examination at the Department of Child Health Care and the Outpatient Clinic of Pediatric Orthopedics at the Affiliated Hospital of Zunyi Medical University. Inclusion criteria were as follows: those who were diagnosed before the age of 24 months and exhibited high-risk symptoms such as asymmetric gluteal folds, unequal length of lower limbs, limited hip joint abduction, abnormal gait, and abnormal internal or external rotation of the lower limbs. In total, 1485 cases were selected for this study, comprising 517 males and 968 females. Early active and individualized treatment and regular follow-ups were considered for children diagnosed with DDH. Cases with the first choice of conservative treatment were retained. The follow-up period ranged from 1 to 3 years. Exclusion criteria were as follows: cases with incomplete data, those who lost follow-ups, and those with the first choice of surgical treatment. Written informed consent was obtained from the patients’ legal guardians. This study was approved by the Medical Ethics Committee of Affiliated Hospital of Zun Yi Medical University.
2.2. Methods 2.2.1. Examination methods.The Graf ultrasound examination method was adopted for infants under the age of 4 months. The Graf ultrasound examination method and/or anteroposterior X-ray examination of both hip joints were used for infants aged 4 to 6 months. X-ray was performed for infants and toddlers over 6 months.
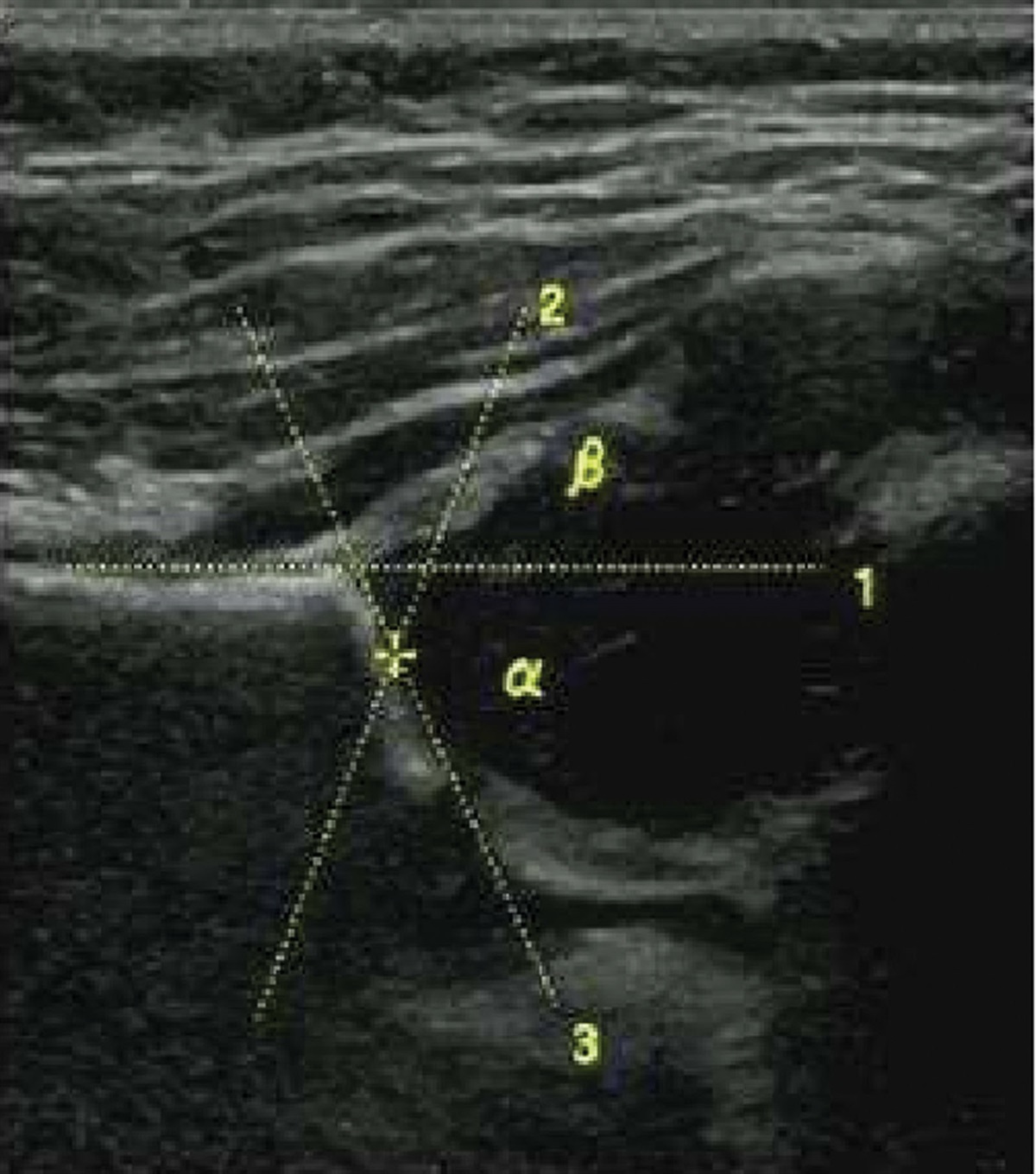
2.2.2. Examination indicators and evaluation criteria.In the Graf ultrasound examination method, the standard cross-section and anatomical landmarks of the hip joint were located according to the Graf method. A standard image was determined by the lower edge of the ilium in the acetabular fossa and straight ilium and acetabulum. In a standard image, the straight ilium, arcuate osseous acetabular top, cartilaginous acetabular top, and the lowest point of the ilium must be seen. We measured angles α and β. Angle α is formed by the intersection of the osseous acetabular top line with the baseline of the ilium echo, and angle β is formed by the intersection of the cartilaginous acetabular top line (Fig. 1). The hip joint was classified based on acetabular morphology, the relationship between the femoral head and the acetabulum, and angles α and β[4] (Table 1). Type I was defined as a normal hip joint, Type IIa was defined as a physiologically immature hip joint, and Type IIb and above were defined as DDH, necessitating early intervention and treatment. In the anteroposterior X-ray of both hip joints, the Y-line connects the upper edges of the Y-shaped cartilage on both sides of the acetabulum. The Perkin line (P-line) is a vertical line extending from the upper outer edge of the acetabulum to the Hilgenreiner line (H-line). The acetabular index represents the angle formed by the line connecting the centers of the Y-shaped cartilage on both sides to the line connecting the upper and lower edges of the acetabular surface. The center-edge angle is the angle between the P-line and the line connecting the outer edge of the acetabulum to the ossification center of the femoral head (Fig. 2). The diagnostic criteria are outlined in Table 2. Those classified as Type II and above are considered to have DDH and thus require early intervention and treatment.[5]
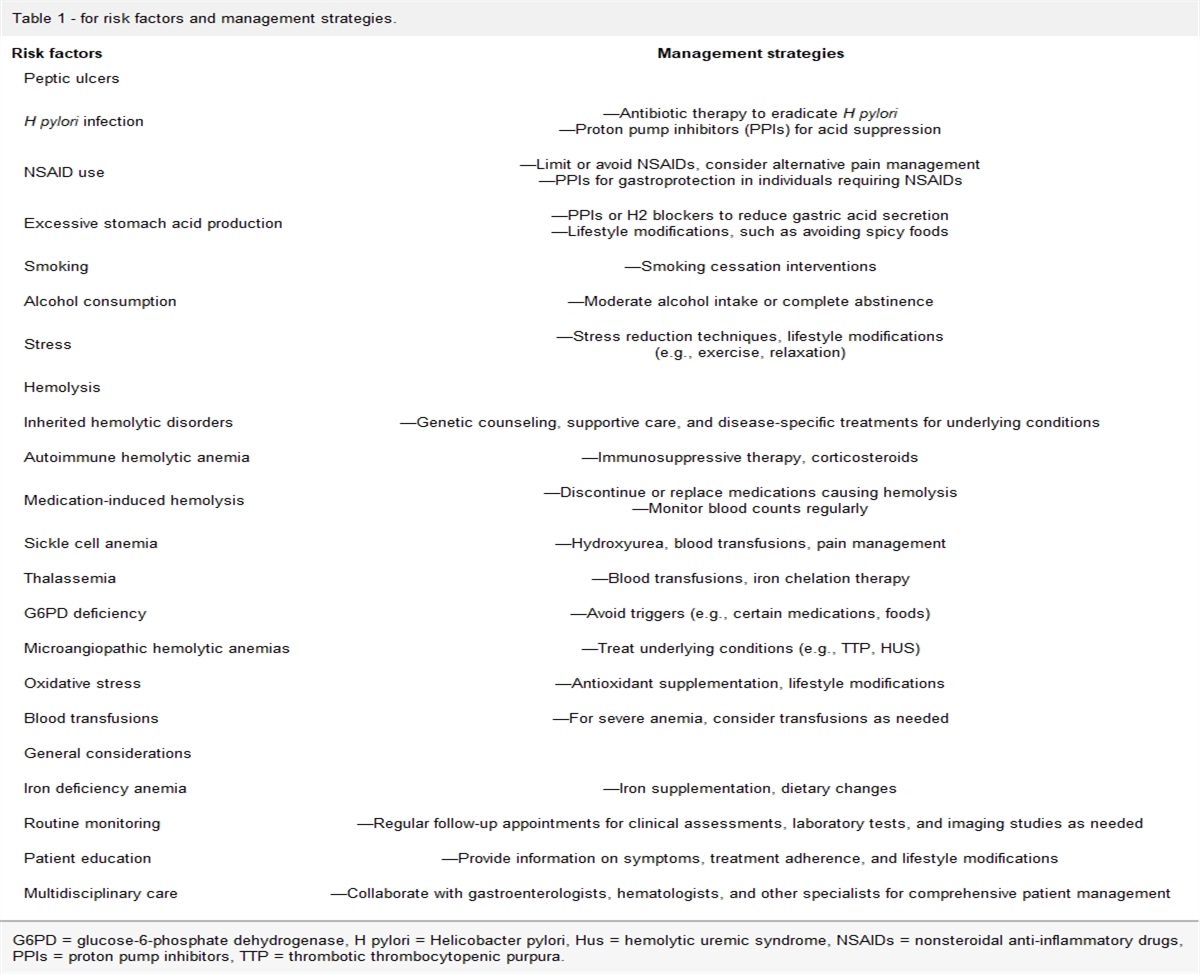
Table 1 - Graf diagnostic criteria for ultrasonic examination of the hip joint. Type α angle (°) β angle (°) Age Ⅰa (normal hip joint) ≥60 ≤55 Any age Ⅰb (normal hip joint) ≥60 >55 Any age Ⅱa (immature hip joint) 50–59 55–77 <3 mo Ⅱb (unstable hip joint) 50–59 55–77 >3 mo Ⅱc (underdeveloped hip joint) 43–49 ≤77 Any age D (semi-dislocated hip joint) 43–49 >77 Any age Ⅲ (semi-dislocated hip joint) <43 >77 Any age Ⅳ (dislocated hip joint) <43 Cannot be measured Any ageAI = acetabular index, CEA = center-edge angle.
 Figure 1.:
Figure 1.: Ultrasound of normal infant hip at 3 months.
 Figure 2.:
Figure 2.: X-ray of normal hip joint of a 1-year-old child.
2.2.3. Treatment methods.For children with DDH under 6 months of age, Pavlik harness or bilateral hip abduction brace was used for treatment. For children with DDH over 6 months old, individualized corrective treatment was used according to the diagnostic classification. For children with hip dysplasia but without dislocation, conservative treatment with bilateral hip human position brace fixation was performed. For children with complete dislocation and ages between 6 and 18 months, after 2 weeks of skin traction on both lower limbs, adductor tenotomy was performed under anesthesia, followed by human position tubular plaster fixation. For children between 18 and 24 months with grade I dislocation, acetabular index < 35°, and stable reduction, we consulted with their family members and informed them of the treatment measures, risks, complications, prognosis, etc. For those who chose conservative treatment, adductor tenotomy was performed under anesthesia after 2 weeks of skin traction on both lower limbs, followed by human position tubular plaster fixation. Surgical treatment was performed for children over 18 months old with a high degree of dislocation and unstable reduction. These cases were excluded from this study. Children with DDH were reexamined with anteroposterior X-ray of both hips 6 months after treatment, and the angle of the hip joint was measured to evaluate the efficacy of treatment. Regular examinations were also conducted for follow-up. The follow-up time ranged from 1 to 3 years. Typical case (Figs. 3–6). Clinical cure was considered if the acetabular head was repositioned and the acetabular index decreased to normal. For those with hip dysplasia, subluxation, or even re-dislocation, individualized treatment was performed according to their condition.
 Figure 3.:
Figure 3.: Right developmental hip dislocation in a 7-month-old girl.
 Figure 4.:
Figure 4.: Manual reduction and conservative treatment with hip human position plaster.
 Figure 5.:
Figure 5.: Review after 1 year of treatment.
 Figure 6.:
Figure 6.: Review after 3 years of treatment.
2.3. Statistical analysisWe used composition ratios and rates for statistical description. The χ2 test was applied for comparing groups. All statistical analyses were conducted using SPSS version 25 (IBM Corp, Armonk, NY). P < .05 was deemed statistically significant.
3. Results 3.1. Early screening dataThe detection rates of DDH in children aged 0 to 6 months, 7 to 12 months, 13 to 18 months, and 19 to 24 months were 24.0%, 2.8%, 9.3%, and 12.2%, respectively. The difference in DDH detection rate between different age groups was statistically significant (χ2 = 213.01, P < .01) (Table 3).
Table 3 - Comparison of abnormal results of DDH screening in different age groups of 1485 cases. Initial diagnosis age (mo) Cases (persons/hips) Males (persons/hips) Abnormal (persons/hips) Females (persons/hips) Abnormal (persons/hips) Total abnormal (persons/hips) Abnormal rate (%) 0–6 295/590 115/230 28/51 180/360 53/91 81/142 24.0 7–12 662/1324 230/460 3/5 432/864 20/32 23/37 2.8 13–18 356/712 128/256 4/4 228/556 39/62 43/66 9.3 19–24 172/344 44/88 2/2 128/256 25/40 27/42 12.2 Total 1485/2970 517/1034 37/62 968/1936 137/225 174/287 9.7DDH = developmental dysplasia of the hip.
In children with DDH, the number of abnormal hip joints with underdevelopment, semi-dislocation, and complete dislocation in each age group is shown in Table 4. The difference in the composition ratio of different types of DDH in different age groups was statistically significant (χ2 = 135.99, P < .01).
Table 4 - The composition of DDH children at different ages in the North Guizhou region. Initial diagnosis age (mo) Abnormal hips Underdeveloped hip joints (hips/percentage) Semi-dislocated hip joints (hips/percentage) Dislocated hip joints (hips/percentage) 0–6 142 109/76.8% 13/9.2% 20/14% 7–12 37 17/45.9% 5/13.5% 15/40.5% 13–18 66 10/15.2% 5/7.6% 51/77.2% 19–24 42 0/0% 1/2.4% 41/97.6%DDH = developmental dysplasia of the hip.
After examining 1485 cases, early active and individualized treatment and regular follow-ups were considered for children diagnosed with DDH. Cases with the first choice of conservative treatment were retained; cases with incomplete data, lost follow-ups, and those with the first choice of surgical treatment were excluded. After treatment, the hip joints returned to normal. Residual hip joint underdevelopment or semi-dislocation was observed until 4 to 5 years of age, but if the acetabular index and center-edge angle showed no improvement, surgical intervention was considered. When dislocation recurred, surgical open reduction was done. The cure rates of DDH in infants aged 0 to 6 months, 7 to 12 months, 13 to 18 months, and 19 to 24 months were 87.0%, 65.7%, 41.0%, and 16.7%, respectively. The difference in the cure rates of conservative treatment of DDH was statistically significant (χ2 = 40.93, P < .01) between different age groups (Table 5).
Table 5 - The outcome of conservative treatment of children with abnormal hip development in the North Guizhou region. Initial age of treatment (mo) Abnormal hips Normal hips Remaining abnormal hips Cure rate (%) 0–6 115 100 15 87.0 7–12 35 23 12 65.7 13–18 39 16 23 41.0 19–24 6 1 5 16.7DDH is a group of abnormalities affecting the bone, cartilage, and surrounding soft tissue structures, which impair the relationship between the femoral head and the acetabulum.[6,7] Some children do not experience early-onset hip dislocation after birth, but growth and developmental process leads to hip dislocation in the future.[8,9] Over the last decades, with in-depth research on the occurrence, development, and treatment of DDH, it has been found that most structures in infant hip joints are composed of cartilage with strong plasticity. Earlier detection can result in simpler treatment and complete restoration of hip joint structure and function.[10–12] For children who are diagnosed after 18 months of age, surgery is the first choice of treatment. Late diagnosis often leads to complications such as joint dysfunction and avascular necrosis of the femoral head, severely affecting the growth and development of the child.[13]
Our study found that the cure rate of conservative treatment of DDH is 87.0% in children aged 0 to 6 months. However, the cure rate of conservative treatment of DDH reduces to 41% in children aged 13 to 18 months and to only 16.7% in children aged 18 to 24 months. The effectiveness of conservative treatment in these cases is not satisfactory, and surgical treatment is generally preferred. Among children with DDH aged 18 to 24 months, 27 cases were only discovered after a long period of limping once they started to walk. Therefore, early screening for DDH in infants younger than 6 months can greatly reduce the incidence of late-stage DDH.
The latest Clinical Diagnosis and Treatment Guidelines for Developmental Dysplasia of the Hip (0–2 years) in China recommend clinical screening for DDH in all infants.[4] A physical examination, including Ortolani and Barlow tests, is conducted by a neonatologist immediately after birth. Within 42 days after birth and 4 to 6 months after birth, a child healthcare physician conducts a screening examination for limitation of hip joint abduction, asymmetrical hip lines, and unequal lengths of the lower limbs.[14] For those with high-risk factors for DDH, such as (1) a family history of DDH; (2) high incidence areas and ethnic groups for DDH; (3) presence of congenital clubfoot, joint laxity, muscular torticollis, and other limb deformities; (4) breech or cesarean delivery; (5) asymmetrical buttock lines; and (6) female infants, selective ultrasound examination can be conducted.[15] Ultrasound examination is an important means of diagnosing DDH, and ultrasound screening can also be used in areas with medical conditions.[16] For infants over 4 months old, ultrasound and/or anteroposterior X-ray examination of both hip joints can be performed; for infants over 6 months old, X-ray examination is used.[17]
This study found that the incidence of abnormal hip joint findings in early DDH screening was 9.7% in children younger than 24 months, and the detection rate was as high as 24.0% among infants aged 0 to 6 months. The incidence of DDH significantly varies worldwide, ranging from 1.5‰ to 109‰.[18–21] Reports from China indicate that the incidence of DDH in places like Beijing, Tianjin, and Shanghai is between 1.1‰ and 3.8‰.[22,23] This could be due to factors such as race, geographic region, examination methods, diagnostic criteria, and different ages of participants. Additionally, inclusion of cases with hip dysplasia and subluxation beyond complete hip dislocation can significantly change the incidence rates. Some reports showed that the incidence rates under different statistical standards are 7.0% and 23.0%, respectively.[24] The incidence rate in this study was higher than that in other regions of China, which may be primarily due to our focused examination of cases with high-risk factors such as asymmetrical buttock creases, internal and external rotation of the lower limbs, unequal lengths of the lower limbs, limited hip joint abduction, and abnormal gait.[25] This approach allows us to conduct more targeted clinical screenings rather than general screenings for all infants and toddlers. We must also consider that swaddling is common in this region, and some cases have a positive family history.
This study found that the main peak of development dysplasia of hip can be observed in infants aged 0 to 6 months. However, complete hip dislocation becomes the primary abnormality in those aged 19 to 24 months. This suggests that hip joint abnormalities in infants and toddlers worsen with age. In the absence of early intervention, hip dysplasia can gradually progress to complete hip dislocation. This not only complicates treatment but also worsens the quality of life and prognosis of patients and imposes a greater burden on patients.
The limitation of this study lies in the small number and scope of infant screening, which only reflects the situation of some areas of Guizhou, China, but is also related to the underdeveloped economy and fewer pediatricians in this region. Despite some limitations of this study, this screening model is more efficient, with less demand for physicians and less cost. We plan to further work with the government’s health sector to expand training for primary doctors on DDH disease, expand the scope of screening for infants and young children, and strive to popularize hip screening for all newborns.
Our study explored the examination of infants with high-risk factors for DDH (such as asymmetric buttock pattern, unequal lower limbs, limited hip abduction, etc), and the active early intervention of the detected abnormal cases, which confirmed that this screening method was effective. We believe that this is a suitable screening model for most less economically developed areas.
AcknowledgmentsThe authors would like to express their gratitude to EditSprings for the expert linguistic services provided.
Author contributionsConceptualization: Xin Lv, Song Yu.
Data curation: Xin Lv, Xiaohong Yang.
Formal analysis: Song Yu, Tianjiu Zhang.
Methodology: Yanpeng Xu.
Supervision: Tangjiang Li.
Writing – original draft: Xin Lv.
References [1]. Canavese F, Castaneda P, Hui J, et al. Developmental dysplasia of the hip: promoting global exchanges to enable understanding the disease and improve patient care. Orthop Traumatol Surg Res. 2020;106:1243–4. [2]. Pavone V, de Cristo C, Vescio A, et al. Dynamic and static splinting for treatment of developmental dysplasia of the hip: a systematic review. Children (Basel). 2021;8:104. [3]. Li R, Wang W. Diagnostic progress of developmental dysplasia of the hip and discussion of screening model in China. Med Recapitulate. 2018;24:2817–22. [4]. Orthopaedic Group of the Chinese Society of Pediatric Surgery, Pediatric Trauma Orthopaedic Group of the Chinese Orthopaedic Association. Detection and treatment of pediatric developmental dysplasia of the hip in children up to two year of age: clinical practice guideline. Chin J Orthop. 2017;37:641–50. [5]. Li T, Wang Y, Zhang M, et al. A new radiographic classification of ‘three lines & one point’ for developmental dysplasia of the hip. Chin J Pediatr Surg. 2017;38:516–20. [6]. de Hundt M, Vlemmix F, Bais JM, et al. Risk factors for developmental dysplasia of the hip: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2012;165:8–17. [7]. Shi L, Ma R. Conservative treatment of hip dysplasia in infants. Orthop J Chin. 2004;12:700–2. [8]. Colta RC, Stoicanescu C, Nicolae M, et al. Hip dysplasia screening epidemiological data from Valcea county. J Med Life. 2016;9:106–11. [9]. Vafaee AA, Baghdadi T, Baghdadi A, et al. DDH epidemiology revisited: do we need new strategies. Arch Bone Joint Surg. 2017;5:440–2. [10]. Li Y, Liu Y, Wu J, et al. Proper timing for discontinuing Pavlik harness treatment in children with developmental dysplasia of the hip. Chin J Pediatr Surg. 2022;43:550–5. [11]. Kelley SP, Feeney MM, Maddock CL, et al. Expert-based consensus on the principles of Pavlik harness management of developmental dysplasia of the hip. JB JS Open Access. 2019;4:e0054. [12]. Westacott DJ, Perry DC. The treatment of neonatal hip dysplasia with splints in the United Kingdom: time for consensus? J Child Orthop. 2020;14:112–7. [13]. Yu J, Chen T. Clinical application of ultrasound in the diagnosis and treatment of developmental hip dysplasia. Chin J Med Ultrasound(Electron Ed). 2015;12:6–10. [14]. Zhang J. Early screening for DDH should take the first step. Shandong Pharm. 2011;51:5–6. [15]. Sun S, Gao X, Huang Z. Clinical screening of developmental hip dysplasia in infants aged 0~6 months. Chin J Woman Child Health Res. 2019;30:1380–4. [16]. Chen B, Li Y, Yang J, et al. Early diagnosis of developmental dysplasia of hip in infants: preliminary report of ultrasonographic examination of 391 cases. Chin J Pediatr Surg. 2003;24:344–7. [17]. Deng X, Yang L, Wang Y, et al. Application and clinical significance of ultra-sound in the diagnosis of hip dysplasia in children. Chin J Child Health Care. 2020;28:1276–1278,1282. [18]. Tréguier C, Chapuis M, Branger B, et al. Pubo-femoral distance: an easy sonographie screening test to avoid late diagnosis of developmental dysplasia of the hip. Eur Radiol. 2013;23:836–44. [19]. Mulpuri K, Song KM, Gross RH, et al. The American Academy of Orthopaedic Surgeons evidence-based guideline on detection and nonoperative management of pediatric developmental dysplasia of the hip in infants up to six months of age. J Bone Joint Surg Am. 2015;97:1717–8. [20]. Kitay A, Widmann RF, Doyle SM, et al. Ultrasound is an alternative to X-ray for diagnosing de-velopmental dysplasia of the hips in 6-month-old children. HSS J. 2019;15:153–8. [21]. Zhao L, Ma Q, Feng X, et al. Screening for developmental dysplasia of the hip in infants in Tibet identifies increased prevalence associated with altitude. Med Sci Monit. 2019;25:5771–5. [22]. Zhang W, Yuan X, Chen X. Study on a new synchronous screening model for congenital heart disease and developmental dysplasia of the hip during the period of the newborn infants visit in Beijing. Chin J Child Health Care. 2011;19:149–51. [23]. Zhang N, Chen X, Wang L. Ultrasonic screening of developmental dysplasia of the hip in infants-screening analysis of 130 cases. Chin J Woman Child Health Res. 2016;27:376–8. [24]. Shen J, Liao H, Tang J, et al. Ultrasound screening analysis of 825 cases of developmental hip joint abnormalities in infants and young children. Chongqing Med J. 2011;40:3300–2. [25]. Gao X, Zhou J. Diagnosis and treatment progress of hip dysplasia. Orthop J Chin. 2010;18:401–4.
留言 (0)