In recent years, the incidence of allergic diseases, such as allergic rhinitis and conjunctivitis, has increased worldwide due to environmental and lifestyle changes [6, 9, 10]. In Japan, over half of the population reported some form of allergic disease; thus, allergic diseases are an important nationwide issue [4]. Seasonal allergic rhinitis due to cedar pollen is Japan’s most prevalent allergic condition. A Japanese epidemiological survey demonstrated a remarkable increase in the overall prevalence of cedar pollinosis in recent years. The rate of cedar pollinosis increased from 19.4% in 1996 to 28.2% in 2006 and 45.6% in 2016 [11]. Symptoms caused by allergic rhinitis, such as nasal congestion, runny or stuffy nose, nose itching, and sneezing, often lead to fatigue, sleep disorders, and other issues that reduce the patient’s quality of life [12]. Furthermore, this condition can cause substantial economic losses [13]. Therefore, treatments for cedar pollen allergy are becoming increasingly important.
SLIT is an effective allergen immunotherapy for allergic rhinitis and conjunctivitis. However, several allergic side effects have been reported, including pharyngeal and throat edema, oral pruritus, throat irritation, altered oral sensation, ear pruritus, and systemic allergic reactions [5, 6]. In addition, the present case report highlights EoE as an important side effect associated with SLIT for cedar pollinosis.
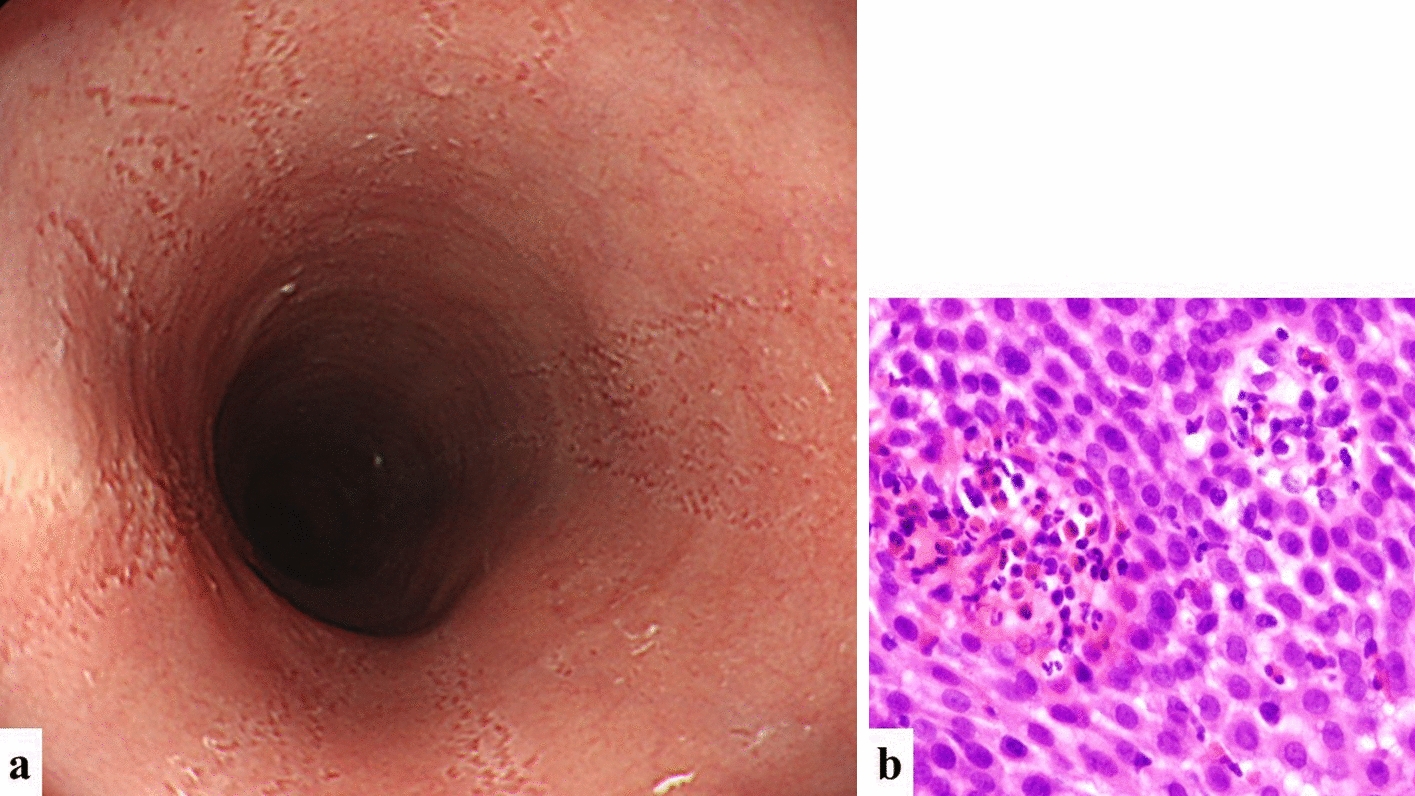
EoE is a clinicopathological disease characterized by esophageal symptoms and eosinophil-predominant inflammation. Over the past two decades, the incidence of EoE has been increasing, primarily in the United States [14]. International guidelines indicate that the diagnosis of EoE should include symptoms related to esophageal functional impairment, such as swallowing difficulties or a sensation of food getting stuck in the throat. Additionally, at least 15 eosinophils per high-power field must be observed in esophageal mucosal biopsies [1].
In our case, the patient had not undergone any laboratory test and endoscopic examination before initiating SLIT for cedar pollinosis because the patient had no symptoms. Therefore, definitive confirmation of the association between SLIT and newly occurrence of EoE was difficult. However, the patient had no gastrointestinal symptoms before starting SLIT therapy. Given that the patient’s esophageal symptoms appeared immediately after starting SLIT, specifically after increasing the cedar pollen extract to a high dose of 5,000 JAU, and the patient’s symptom improved after switching the swallow to the spit method, it was reasonable to strongly suspect EoE triggered by SLIT.
EoE is a distinct form of food allergy, and a significant portion of EoE patients are sensitized to food allergens and aeroallergens [15]. Removal of food antigens or inhaled antigens such as pollen leads to a response, and the reintroduction of similar antigens can cause a recurrence of EoE. Cross-sensitization between food allergens and aeroallergens may contribute to esophageal inflammation [16, 17]. Thus, EoE may develop in response to chronic antigen exposure introduced from the oral side [17, 18]. Previous case reports showed that EoE induced by SLIT for aeroallergens improved after discontinuation of SLIT [19,20,21,22,23,24,25,26,27], suggesting that SLIT-induced EoE may be reversible.
The number of patients with SLIT will increase in the future as the prevalence of allergic rhinitis and conjunctivitis such as cedar pollinosis increases. Therefore, the importance of SLIT-triggered EoE will increase in clinical practice. However, SLIT-triggered EoE has not been widely reported. Table 2 summarizes the EoE cases associated with SLIT [19,20,21,22,23,24,25,26,27,28]. Among the 16 cases of EoE (including our case), SLIT was discontinued in 10 cases to improve symptoms, and patients switched from the swallow to the spit method in 5 cases, including our case. In the 5 patients who switched to the spit method, the outcome of one case was unknown and symptoms improved in 3 cases. Therefore, switching from the swallow to the spit method is an acceptable strategy in patients with SLIT-triggered EoE before discontinuing SLIT. In our case, the patient adopted the spit method and held the cedar pollen tablet under the tongue for 2 min before spitting it out along with the saliva. Furthermore, based on the comprehensive literature review, we notably found that the duration from initiating SLIT to the onset of EoE varied. In patients with multiple allergic conditions, the onset of EoE can occur within a month after initiating SLIT, as observed in our case. Conversely, EoE may occur as long as three years after starting SLIT, especially in patients without multiple allergic conditions.
Table 2 Summary of previous reports on eosinophilic esophagitis associated with sublingual immunotherapySymptoms such as heartburn, dysphagia, or abdominal and thoracic discomfort are similar in EoE and reflux esophagitis. Difficulties in distinguishing EoE from reflux esophagitis based on clinical features and endoscopic findings were described in previous reports [29]. Therefore, inquiring about SLIT use is essential for differentiating reflux esophagitis and EoE when patients present with reflux esophagitis-like symptoms.
In conclusion, SLIT for cedar pollinosis can trigger EoE. Clinicians should inquire about SLIT use before performing endoscopic examinations in patients with reflux esophagitis-like symptoms. The onset of EoE can occur within a month after initiating SLIT in patients with multiple allergic conditions, as observed in our case. Furthermore, switching from the swallow to the spit method may be an effective strategy for alleviating SLIT-triggered EoE.




留言 (0)